
Abstract
Purpose
An analysis of patients in the United States Immunodeficiency Network (USIDNET) registry previously described a discordance in the reported prevalence of humoral immune deficiency in patients with DiGeorge syndrome (DGS) and its treatment. The primary purpose of this study is to evaluate the rates of humoral immunodeficiency and immune globulin replacement therapy (IGRT) use in patients with DiGeorge syndrome in the USIDNET registry as of September 2016, and to correlate IGRT use with prior infections and laboratory evidence of immune deficiency.
Methods
Current patients in the USIDNET registry with DGS were identified. Patients who were treated with immune globulin replacement therapy (IGRT) were compared with those who were untreated with respect to their laboratory findings and clinical history.
Results
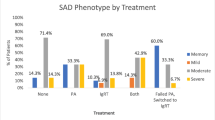
Four hundred seventy-three patients were identified. The use of IGRT in patients with DGS has increased over time from 3 to 6.6%. IGRT was more common in patients with humoral immune deficiency (18.2% of those with hypogammaglobulinemia, 39.1% of those with documented low vaccine titers), but most patients with evidence of humoral immune deficiency remain untreated with IGRT. Patients treated with IGRT were more likely to have experienced episodes of pneumonia, sepsis, and bacterial skin infections (p < 0.01 for all).
Conclusions
Humoral immune deficiencies were more common among patients with DGS than previously reported. IGRT was used most commonly in patients with DGS who demonstrated frequent or severe bacterial infections. There is still a significant deficit between those with DGS who have laboratory evidence of a humoral immune deficiency and those being treated for it.


Similar content being viewed by others


Data Availability
The USIDNET registry database is available to contributing researchers at usidnet.org. The laboratory data reported in this study is reported as supplementary materials.
References
Maggadottir SM, Sullivan KE. The diverse clinical features of chromosome 22q11.2 deletion syndrome (DiGeorge syndrome). J Allergy Clin Immunol Pract. 2013;1:589–94.
Sullivan KE, Jawad AF, Randall P, Driscoll DA, Emanuel BS, McDonald-McGinn DM, et al. Lack of correlation between impaired T cell production, immunodeficiency, and other phenotypic features in chromosome 22q11. 2 deletion syndromes. Clin Immunol Immunopathol. 1998;86:141–6.
Patel K, Akhter J, Kobrynski L, Gathman B, Davis O, Sullivan KE. Immunoglobulin deficiencies: the B-lymphocyte side of DiGeorge syndrome. J Pediatr. 2012;161:950–3.
Tam PI, McAllister SC. Vaccine responses and immunologic characteristics of pediatric patients with DiGeorge syndrome. Clin Pediatr. 2015;54(13):1290–2.
Maggadottir SM, Maurer KA, Sullivan KE. Defective B-cell maturation in chromosome 22q11.2 deletion syndrome. J Allergy Clin Immunol. 2013;131(2, Supplement):AB8.
Sullivan KE, Puck JM, Notarangelo LD, et al. USIDNET: a strategy to build a community of clinical immunologists. J Clin Immunol. 2014;34(4):428.
Seeborg FO, Seay R, Boyle M, Boyle J, Scalchunes C, Orange JS. Perceived health in patients with primary immune deficiency. J Clin Immunol. 2015;35:638–50. https://doi.org/10.1007/s10875-015-0196-7.
Jolliff CR, Cost KM, Stivrins PC, Grossman PP, Nolte CR, Franco SM, et al. Reference intervals for serum IgG, IgA, IgM, C3, and C4 as determined by rate nephelometry. Clin Chem. 1982;28:126–8.
Author information
Authors and Affiliations
Contributions
Dr. Bennett conceived of the study, assisted with protocol design, and data analysis, and interpretation. Dr. Soshnick assisted with protocol design and performed data analysis. Dr. Joseph assisted with protocol design and data analysis. All authors contributed to the manuscript preparation and revision.
Corresponding authors
Ethics declarations
Ethical Approval
Institutional review board approval was granted by Connecticut Children’s Medical Center (CCMC) in Hartford Connecticut. The research was judged exempt from review and consent was not required due to the nature of it being a retrospective study of non-identified data.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Competing Interests
NB is a speaker/consultant for Horizon Pharma (maker of Actimmune) and has clinical trial support from Baxalta (makers of Gammagard, Cuvitru and Hyqvia). SS and TJ have no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Soshnick, S.H., Joseph, T. & Bennett, N.J. Humoral Immunodeficiency and Immune Globulin Replacement Therapy (IGRT) Usage in DiGeorge Syndrome. J Clin Immunol 41, 1208–1212 (2021). https://doi.org/10.1007/s10875-021-01012-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10875-021-01012-8