
Abstract
Background
As autistic children are being diagnosed at a younger age, the need to identify appropriate early supports has increased. Therapist-delivered and parent-mediated autism intervention may benefit children and parents.
Objective
This pilot study examined developmental outcomes for autistic pre-schoolers and mental health and wellbeing outcomes for their parents (n = 53) following a 10-month intervention period.
Methods
All families were accessing therapist-delivered interventions—the Early Start Denver Model (ESDM) or usual community services—and some families also received additional parent-coaching ESDM (P-ESDM). Families were assessed at 3 timepoints.
Results
Overall children made significant gains in cognitive skills and adaptive behaviour, with no differences between groups. Parents overall reported increased parenting stress over time. P-ESDM conferred no added benefit for child outcomes, and similarly, no clear benefit for parent outcomes.
Conclusions
Our findings suggest that children receiving early intervention make developmental gains, regardless of type of intervention, and challenges assumptions that, as an adjunct to other intervention programs, P-ESDM improves child or parent outcomes. Further research is needed to explore the effects of parent-mediated programs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Autism is characterised by challenges in social communication alongside the presence of repetitive, intense, narrow interests and behaviours and sensory sensitivities or aversions (American Psychiatric Association, 2013). These characteristics emerge within the first two years life (Cleary et al., 2023; Tanner & Dounavi, 2021), with children usually receiving a diagnosis between 3 and 4 years of age (van’t Hof et al., 2021). As autistic children are being diagnosed at a younger age there is an increased need to identify appropriate early supports (Fuller & Kaiser, 2020).
Supports for young autistic children include a wide range of services and programs that can be classified according to their theoretical principles, methods, and intended outcomes: behavioural, developmental, Naturalistic Developmental Behavioural Intervention (NDBI), Treatment and Education of Autistic and Related Communication Handicapped Children (TEACCH), sensory-based, animal-assisted, and technology-based (Daniolou et al., 2022; Sandbank et al., 2020). Interventions may be applied one-on-one with a trained practitioner (e.g., Joint Attention, Symbolic Play, Engagement, and Regulation (JASPER); Kasari et al., 2006) or in a group setting (e.g., Hanen's More than Words (HMTW); Sussman, 1999). Alternatively, an increasing number of interventions are available in a parent-mediated format, such as the parent-mediated communication focused support for children at higher likelihood of being autistic (iBASIS-Video Interaction to Promote Positive Parenting (iBASIS-VIPP); Green et al., 2013) and diagnosed autistic children (Paediatric Autism Communication Thearapy (PACT); Green et al., 2010) and the PEERS® for Preschoolers (P4P) program (Factor et al., 2022). While some interventions focus broadly on core autism features, such as JASPER and the Early Start Denver Model (ESDM; Rogers & Dawson, 2010), other focus on targeted skills, such as social skills (e.g., P4P) or social communication (e.g., PACT and iBASIS-VIPP). Recently, a more holistic approach incorporating the effective components from various interventions has been developed for young children with diagnosed or suspected developmental delays or disabilities that focuses on child social communication and behaviour as well as parent wellbeing (WHO Caregiver Skills Training (CST) Program; Salomone et al., 2019).
Some parent-mediated intervention have been linked to improved child outcomes, including communication (Salomone et al., 2021; Sengupta et al., 2023; Whitehouse et al., 2021), social interactions (Antezana et al., 2023; Factor et al., 2022, 2023a, 2023b; Sengupta et al., 2023), adaptive behaviour (Sengupta et al., 2023), and challenging behaviours (Antezana et al., 2023; Lau et al., 2022). In a recent RCT of a pre-emptive parent-mediated intervention, infants who received iBASIS-VIPP showed significant reductions in level of autism traits, odds of meeting particular diagnostic criteria, and likelihood of overall autism diagnosis at three years of age (Whitehouse et al., 2021). Parents in the iBASIS-VIPP group reported significant improvements in their child’s expressive and receptive language and gestures compared to treatment as usual. The related parent-mediated intervention for diagnosed autistic children, PACT, has consistently shown similar benefits for child developmental outcomes (Green et al., 2010; Jurek et al., 2021; Pickles et al., 2016). Despite some evidence of improvements in child cognition and language from therapist-delivered ESDM (e.g., Estes et al., 2015; Mirenda et al., 2022; Vivanti et al., 2013), RCTs of parent coaching ESDM (P-ESDM; Rogers et al., 2012a, 2012b) have shown little-to-no evidence of improved child developmental outcomes (Rogers et al., 2019, 2022, 2012a, 2012b; Vismara et al., 2018). Although various adaptations have been made to ESDM and P-ESDM (e.g., dosage, autism-specific vs inclusive settings, telehealth P-ESDM, enhanced low-intensity P-ESDM, group P-ESDM), child outcomes have not differed among the variations, suggesting that providing early intervention at a lower intensity or through an adapted format did not improve child outcomes relative to comparison or no intervention (Fuller & Kaiser, 2020; Rogers et al., 2019; van Noorden et al., 2022; Vismara et al., 2018; Vivanti et al., 2019). Newer parent-mediated interventions for autistic children (i.e., P4P) and children with any diagnosed or suspected developmental delay or disability (i.e., WHO CST) have shown promising early evidence of benefits for child outcomes (Antezana et al., 2023; Factor et al., 2022, 2023a, 2023b; Lau et al., 2022; Salomone et al., 2021; Sengupta et al., 2023).
Parent-mediated interventions that focus on child outcomes may serve as an indirect avenue through which supports may positively impact parental mental health and wellbeing, perhaps through increased sense of parenting efficacy or improved relationship quality with their child. Parents of autistic children have reported more mental health difficulties (i.e., stress, anxiety, and depression) than parents of non-autistic children (Ingersoll & Hambrick, 2011; Padden & James, 2017; Quintero & McIntyre, 2010; Schnabel et al., 2020), as well as lower levels of wellbeing (Green et al., 2021; Salomone et al., 2018). Individual differences in mental health and wellbeing in parents of autistic children have been linked to a broad range of factors, including use of coping strategies (Benson, 2014; Vernhet et al., 2019), social supports (Benson, 2020; Catalano et al., 2018), cultural background (Smith et al., 2021a, 2021b), mindfulness (Cheung et al., 2019; Green et al., 2021), personality (Green et al., 2021), and autistic traits (Ingersoll & Hambrick, 2011; Lau et al., 2014; Pruitt et al., 2018). Child related characteristics have also been associated with parent mental health and wellbeing, including the child’s autistic presentation (Green et al., 2021; Ingersoll & Hambrick, 2011; Mathew et al., 2019; Yamada et al., 2007), emotional and behaviour problems (Cheung et al., 2019; Pruitt et al., 2018; Salomone et al., 2018; Smith, Sulek, Green, et al., 2021), and relationship quality with the parent (Derguy et al., 2016; Hastings et al., 2006). Individual studies and trials of parenting-mediated interventions have demonstrated benefits for parenting stress (Dababnah & Parish, 2016; Estes et al., 2014; Salomone et al., 2021; Sengupta et al., 2023; van Noorden et al., 2022; Zhou et al., 2018), parental wellbeing (Lau et al., 2022; Leadbitter et al., 2018; Palmer et al., 2020), parental self-efficacy (Factor et al., 2023a, 2023b; Salomone et al., 2021; Schertz et al., 2020), parental responsiveness (Whitehouse et al., 2021), parent–child interactions (Factor et al., 2023a, 2023b; Salomone et al., 2021)and parenting skills and knowledge (Ho & Lin, 2020; Sengupta et al., 2023).
The Current Study
Among currently available manualised autism interventions, one of the most widely used is the ESDM (Rogers & Dawson, 2010). The ESDM is a type of NDBI with adaptations for direct delivery by a therapist, either one-to-one (ESDM; Rogers & Dawson, 2010) or in group-based format (G-ESDM; Vivanti et al., 2014), as well as via parent coaching (P-ESDM; Rogers et al., 2012a, 2012b).
While therapist-delivered supports have been shown to improve developmental outcomes in young autistic children (Tachibana et al., 2017), it is less clear what benefit parent-delivered supports may have for children and their parents (Jhuo & Chu, 2022). In this pilot study, we examined outcomes for children and parents following access to various types of early intervention in a community-based Australian cohort of autistic pre-schoolers and their parents. Specifically, we aimed to compare outcomes over an approximate 10-month period for: (1) children receiving ESDM across various therapist-delivered modes (i.e., individual, group) compared to children accessing community services; (2) children participating in parent coaching ESDM as an adjunct to therapist-delivered ESDM compared to children participating in therapist-delivered ESDM only; and (3) parents participating in parent coaching ESDM compared to therapist-delivered ESDM only. We hypothesised that: (1) there would be no significant differences in child outcomes by delivery mode of ESDM (i.e., group, individual, parent-delivered); (2) children receiving ESDM by any delivery mode would show significant improvements in cognitive skills over time, and significant improvements compared to the community services group; and (3) parents involved in parent coaching ESDM would show reduced parenting stress compared to parents of children receiving therapist-delivered ESDM only.
Method
Participants and Procedure
Autistic pre-schoolers aged 17 to 44 months (M = 35.44, SD = 6.31) and their parents were recruited between 2017 and 2020 from various community early intervention services, including a university-affiliated service providing ESDM-based supports. All eligible families at the university-affiliated service were invited to participate. Families accessing community intervention services were recruited from the university-affiliated service’s waitlist and from the Olga Tennison Autism Research Centre participant registry. Families were eligible for this study if children had: (1) autism, confirmed by Autism Diagnostic Observation Schedule (ADOS-2; Lord et al., 2012) at intake; and (2) non-verbal developmental age-equivalence ≥ 12 months, confirmed by Mullen Scales of Early Learning (MSEL; Mullen, 1995). Families were ineligible if: (1) they did not intend to remain living in the area for the study duration; (2) the participating child had an autistic twin; (3) the parent’s English proficiency would compromise their ability for full participation; or (4) the parent had significant unmanaged depression or anxiety such that participation might exacerbate their condition. Participant characteristics are presented in Table 1. Most parents were mothers with at least a tertiary level education. Nearly two-thirds self-identified as culturally and/or linguistically diverse (CALD). There were no between-group differences in demographic factors. Children in the current study had similar levels of autistic traits, developmental/cognitive skills, and adaptive behaviour compared to previously reported on Australian cohorts of autistic pre-schoolers accessing community-based interventions (Berends et al., 2023; Vivanti et al., 2019).
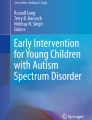
Participants were assessed at three timepoints (hereafter Time 1 (T1), Time 2 (T2), and Time 3 (T3)), approximately 5 months apart, corresponding to the start, middle, and end of a year-long intervention placement for the university-affiliated service. All assessments were conducted at the university-affiliated service. A subset (n = 18) of families (those recruited between 2017 and 2019) were randomised immediately after their T2 assessment for additional P-ESDM sessions. P-ESDM was offered between T2 and T3 assessments, with 17 families taking up this offer. There were no differences in demographic factors between participants who were loss to follow-up (n = 5) and those retained. Enrolment characteristics are presented in Fig. 1. Approval for this study was obtained from the La Trobe University Human Research Ethics Committee (HREC # 16–136) and parents provided informed consent for their own and their child’s participation. Parents received a written report summarising their child’s ADOS-2 and MSEL assessments; no other incentives were given.

Study enrolment and participation characteristics. Eligible participants were assessed at three timepoints. Immediately after Time 2, a subset of participants were randomised to be offered P-ESDM
Deviations from Original Protocol
The intended sample size was N = 90, with P-ESDM randomisation occurring for all groups. However, the COVID-19 pandemic resulted in multiple prolonged periods of lockdown in the region, impacting on recruitment for the Community Services group, and P-ESDM could no longer be offered. The final sample size (N = 53 at T1) was therefore underpowered for a robust test of the efficacy of parent coaching as an adjunct to other therapist-delivered intervention, and the trial was therefore reframed as an evaluation of the preliminary efficacy of P-ESDM and an evaluation of the relative gains for children engaged in different types of therapist-delivered intervention.
Design and Intervention Approaches
At T1 families were enrolled into one of three groups: ESDM (n = 10), G-ESDM (n = 26), and Community Services (n = 17). Children received ESDM and G-ESDM through the Victorian Autism Specific Early Learning and Care Centre (ASELCC), a university-based service that offers intervention within an early learning and long day care program.
Children in the ESDM group received one-to-one ESDM within a mainstream childcare setting (n = 3) and/or the home environment (n = 7) for at least 10 h of intervention per week. This ESDM format mirrors the one-to-one approach manualised by Rogers and Dawson (2010) but was adapted for delivery by trained paraprofessional staff (therapy assistants) under the supervision of an ESDM certified therapist and with consultation from the ASELCC allied health team. The paraprofessional staff were trained childhood educators with a diploma or Certificate III qualification. Most ESDM certified therapists had a tertiary level qualification (Bachelor degree or higher) prior to ESDM training. Following initial training, therapy assistants submitted video footage from two sessions for a formal fidelity check by the supervising ESDM certified therapist. Over the course of the child’s program, the ESDM certified therapist conducted further formal fidelity checks, twice per 12-weekly goal cycle, and provided further coaching as required.
Children in the G-ESDM group participated in group-based ESDM in an autism-specific childcare setting. Intervention delivery was by a core classroom staff of early childhood educators who were trained as ESDM paraprofessionals, with at least one ESDM certified therapist per room. Intervention hours were focused between 9:30am and 2:30 pm, and most children attended three days per week, totalling approximately 15 h of intervention per week. See Vivanti et al. (2014) for further details.
The Community Services group comprised children who were accessing services outside of the ASELCC. Supports included allied health and other intervention programs (e.g., ABA). Intervention hours varied, ranging from 0 to 25 h per week. The type and quantity of interventions accessed by the Community Services group were representative of the early interventions generally accessed by Australian pre-schoolers, who mostly engage in low-frequency allied health services (i.e., speech pathology and occupational therapy) and generic (i.e., not autism-specific) early intervention (Carter et al., 2011).
A subset of families were randomised after their T2 assessment to receive adjunctive parent coaching ESDM (P-ESDM; Rogers et al., 2012a, 2012b) (Parent Coaching group). Randomisation was stratified by initial enrolment group, T2 child age (< vs ≥ 36 months), and T2 Clarke modification of the Holroyd Questionnaire on Resources and Stress (CQRS; Konstantareas et al., 1992) score (median split at < vs ≥ 2.40). The project officer informed parents of the randomisation outcome. Researchers administering T3 assessments were blind to randomisation outcomes, and were kept separate from the allied health team who were delivering P-ESDM. A total of 13, hour-long, weekly, clinic-based P-ESDM sessions were offered, for completion between T2 and T3. Initial P-ESDM sessions involve children being assessed by an ESDM certified parent coach (with a tertiary level qualification), and the coach and parent formulating learning objectives. During subsequent sessions, parents received hands-on practice implementing ESDM techniques with guidance from the coach. Parent coaches were ESDM certified therapists who participated in a P-ESDM training workshop, completed coaching sessions with at least one practice family, and achieved fidelity on one video submission prior to commencing work with families in the study. P-ESDM coaches conducted monthly peer supervision sessions throughout the duration of the study. See Rogers et al., (2012a, 2012b) and Rogers et al., (2012a, 2012b) for more details about P-ESDM.
Measures
Child Outcomes
Autism traits were measured at T1 and T3 using the ADOS-2 (Lord et al., 2012), a semi-structured behavioural assessment for autism. Assessments were administered by the research team who were trained to research-level reliability. The ADOS-2 is available in five modules, depending on the individual’s age and expressive language ability. The modules used within the current study included the Toddler Module (for children aged 12–30 months), Module 1 (for children aged 31 months and older with no/limited speech), and Module 2 (for children using phrase speech). Calibrated Severity Scores (CSS; Esler et al., 2015) were calculated for analysis (range 1–10; higher scores reflecting more autism traits). The CSS has shown strong test re-test reliability across all modules (ICC = 0.71–0.89, p < 0.05) (Janvier et al., 2022).
Developmental/cognitive skills were assessed at each timepoint using the MSEL (Mullen, 1995). The MSEL is a standardised assessment of verbal (receptive and expressive language) and non-verbal (visual reception and fine motor) abilities, normed for use from birth to 5 years and 8 months of age. An overall developmental quotient (DQ) was computed for analysis (i.e., age equivalent average/chronological age × 100) with scores at/near 100 reflecting skills near chronological age expectations, with higher scores indicating greater developmental abilities. The MSEL has good internal reliability and strong test–retest and inter-scorer reliability (Mullen, 1995), as well as construct, convergent, and divergent validity (Swineford et al., 2015). The MSEL is routinely used to measure developmental skills in autistic children (e.g., Vivanti et al., 2019; Whitehouse et al., 2021).
Adaptive skills were measured at each timepoint using the Vineland Adaptive Behavior Scales 2nd Edition (VABS-II; Sparrow et al., 2005) parent interview form, which is suitable for use across the lifespan. The Adaptive Behavior Composite (ABC) Standard Score was used in analysis (population M = 100; SD = 15; higher scores reflecting greater adaptive abilities). The VABS-II has strong internal consistency, test–retest reliability, inter-interviewer reliability, and validity (Sparrow et al., 2005), and is regularly used to measure adaptive skills in autistic children (e.g., Vivanti et al., 2019; Whitehouse et al., 2021).
Parent Outcomes
Wellbeing was measured at each timepoint using the Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS; R Tennant et al., 2007a, 2007b). The WEMWBS is a 14-item questionnaire measuring subjective and psychological components of wellbeing, with items rated on a 5-point Likert-type scale (1 = None of the time; 5 = All of the time). Items are positively worded (e.g., “I’ve been feeling optimistic about the future), with higher scores reflecting greater wellbeing. Total scores were used in analyses (range 14–70). The WEMWBS has good validity and high reliability (Ruth Tennant et al., 2007a, 2007b) and is sensitive to change across populations and in diverse public health interventions and programs (Stewart-Brown et al., 2011).
Psychological distress was measured using the Depression Anxiety Stress Scales (DASS-21; Lovibond & Lovibond, 1995). The DASS-21 is a 21-item questionnaire, with items rated on a 4-point Likert-type scale (0 = Did not apply to me at all; 3 = Applied to me very much, or most of the time). Items are negatively worded (e.g., I find it hard to wind down), with higher scores indicating greater problems across three subscales measuring depression, anxiety, and stress. Total scores were used in analyses (range 0–120). The DASS-21 has a more robust factor structure than the DASS, and high reliability and convergent validity with other comparable measures (Henry & Crawford, 2005).
Parenting-related stress and resources were measured using the Clarke modification of the Holroyd Questionnaire on Resources and Stress (CQRS; Konstantareas et al., 1992), designed for use with families with children with neurodevelopmental conditions. The CQRS is a 78-item questionnaire, with items rated on a 4-point Likert-type scale (1 = Strong agreement with statement; 4 = Strong disagreement with statement). Statements are either positively (e.g., “Our relatives have been helpful”) or negatively worded (e.g., “I have too much responsibility”), with negatively worded items reverse scored, so that higher scores indicate more parenting stress and fewer resources. Mean scores were retained for analyses (range 1–4). The CQRS has been shown to have good internal consistency, split-half reliability, and coefficient of stability, as well as acceptable construct and concurrent validities (Konstantareas et al., 1992).
Finally, parenting sense of competence was measured using the Parenting Sense of Competence Scale (PSOC; Johnston & Mash, 1989). The PSOC is a 17-item questionnaire, with items rated on a 6-point Likert-type scale (1 = Strongly Agree; 6 = Strongly Disagree). Statements are either positively (e.g., “I meet my own personal expectations for expertise in caring for my child”) or negatively worded (e.g., “My mother/father was better prepared to be a good mother/father than I am”), with positively worded items reverse scored, so that higher scores reflect greater parenting sense of competence. Mean scores were used in analyses (range 1–6). The PSOC has been shown to have good reliability and validity (Karp et al., 2015; Ohan et al., 2000; Rogers & Matthews, 2004).
Statistical Procedure
We conducted a series of 2(group) × 2(time) mixed analyses of variance (ANOVAs), with each child outcome measure as the dependent variable. A two-stage approach was followed to compare child outcomes across: 1) ESDM vs. G-ESDM vs. Community Services; and 2) Parent Coaching vs No Parent Coaching. We took a similar approach for parent outcomes, but included any potentially confounding child characteristics as covariates in an ANCOVA. Significant omnibus effects were followed up with post-hoc tests with Bonferroni correction. Extreme outliers—4 data points for MSEL DQ, 1 for VABS ABC, and 2 for DASS-21 total score—were Winsorised to within 2.5 standard deviations of the mean, and other assumptions for ANOVA were met. Face-to-face assessments for some participants in the Community Services group (n = 10 at T2; n = 11 at T3) were impacted due to the COVID-19 pandemic, during which the local region experienced multiple, protracted periods of lockdown (i.e., stay-at-home order); therefore, analyses of child outcomes that include the Community Services group include the timepoints with the most data available. JASP (Version 0.17.1.0) open source software was used for analyses (JASP Team, 2023).
Results
Child Outcomes after Therapist-Delivered Interventions
Figure 2 presents child outcomes over time for the ESDM, G-ESDM, and Community Services groups. Mean scores and results from the two-way mixed ANOVA models are presented in Table 2. No significant main effects of time, group, or two-way interaction were found for ADOS CSS. For MSEL DQ, a significant main effect was found for time (p = 0.005), but neither effect of group nor the two-way interaction of group*time was significant. Post hoc Bonferroni-corrected tests showed that MSEL DQ was significantly higher at T3 compared to T1 (p = 0.005). For VABS ABC, there was a significant main effect of time (p < 0.001), but not of group, and there was a trend for a two-way interaction (p = 0.055). VABS ABC was significantly higher at T3 compared to T1 (p < 0.001).

Mean Scores for Child Outcome Measures Over Time for ESDM, G-ESDM and Community Services Groups. Mean scores at each available timepoint for ESDM, G-ESDM, and Community Services groups for ADOS CSS (2a), MSEL DQ (2b), and VABS ABC (2c). Significant differences were found between MSEL DQ scores at Time 1 and Time 3, and between VABS ABC scores between Time 1 and Time 3
Child Outcomes After Parent Coaching
Child outcomes over time were then compared between children who received P-ESDM as an adjunct to therapist-delivered ESDM (Parent Coaching group) to children who only received therapist-delivered ESDM (No Coaching group). Mean scores and results from separate two-way mixed ANOVA models for child outcomes are presented in Fig. 3 and Table 3. There were no significant main effects of time or group, or two-way interaction on ADOS CSS. For MSEL DQ, a significant effect of time (p < 0.001) and significant time*group interaction (p = 0.010) were found. Post hoc tests showed that MSEL DQ was significantly higher at T3 vs. T1 (p < 0.001) and at T3 vs T2 (p = 0.033) for the No Coaching group only (p < 0.001), with no significant differences across timepoints for the Parent Coaching group. For VABS ABC, a significant effect of time (p < 0.001) was found reflecting higher scores at T2 vs T1 (p = 0.026) and at T3 vs. T2 (p = 0.003). There was no main effect of group nor interaction of group*time.

Mean Scores for Child Outcome Measures Over Time for Parent Coaching vs No Coaching. Mean scores at each available timepoint for the Parent Coaching and No Coaching groups for ADOS CSS (3a), MSEL DQ (3b), and VABS ABC (3c). Significant differences were found between MSEL DQ scores at Time 1 vs Time 3 and at Time 3 vs Time 2 for the No Coaching group. Significant differences were also found in VABS ABC scores at Time 1 vs Time 2 and at Time 3 vs Time 2
Parent Outcomes after Parent Coaching
Mean scores for parent outcomes are depicted in Fig. 4, and results from separate two-way mixed ANCOVA models for each outcome measure (controlling for MSEL DQ at T1) are presented in Table 4. There were no significant main effects of time or group, nor time*group interaction for either the DASS-21 total score or WEMWBS total score. A significant main effect of time (p = 0.008) was found for the CQRS, reflecting higher levels of parenting stress at T3 vs. T2 and T3 vs. T1 (both p < 0.001). There was a significant time*group interaction (p = 0.018), but not main effects, for PSOC total scores, driven by a trend (p = 0.051) for the No Coaching group to have lower levels of sense of competence at T3 vs. T1.

Mean Scores for Parent Outcome Measures Over Time for Parent Coaching, No Coaching, and Community Services Groups. Mean scores at each timepoint for the Parent Coaching group, No Coaching group, and Community Services group for WEMWBS total (4a), DASS-21 total (4b), CQRS total (4c) and PSOC total (4d). Significant differences were found between CQRS scores at Time 1 and Time 3, and at Time 2 and Time 3. A significant interaction between time and group was found for PSOC total scores, with a trend for the No Coaching group to have lower PSOC scores at Time 3 compared to Time 1
Discussion
Therapist-delivered supports have been shown to improve some developmental outcomes in young autistic children (Tachibana et al., 2017); however, it is less clear what impact parent-delivered supports may have for children, or their parents (Jhuo & Chu, 2022). In this pilot study, we assessed child and parent outcomes after receiving ESDM via various delivery models and community services over an approximate 10-month period. We found that children’s developmental/cognitive skills and adaptive behaviour improved over time, and that parenting stress increased over time. However, we did not find evidence suggesting that children or their parents may benefit more from any one model of intervention.
As expected, children made similar and significant gains in cognitive skills irrespective of which therapist-delivered ESDM model they were involved in. This finding is consistent with previous research comparing outcomes in an autism-specific setting to an inclusive setting (Vivanti et al., 2019). We also found significant improvement in parent-reported adaptive behaviour. These findings are broadly in line with much of the early intervention literature (Tachibana et al., 2017) and with previous studies of ESDM which have demonstrated positive effects for children’s cognitive skills (Dawson et al., 2010; Vivanti et al., 2013, 2014, 2016). The evidence suggesting that ESDM may have a positive effect on adaptive behaviour however has been mixed (Dawson et al., 2010; Vivanti et al., 2014). Overall, the findings from the current study in conjunction with previous literature suggest that the ESDM approach itself may be more important to child outcomes than particular aspects about the delivery, such as the setting, dosage, or level of training of the therapist.
Interestingly, we did not find clear evidence suggesting that children involved in ESDM models of intervention had better developmental outcomes than children in the Community Services group. While the types of services that children in the Community Services group accessed varied substantially, their experience reflected the range of locally available services. While some studies have found that participating in ESDM was associated with better child outcomes compared to other intervention types (e.g., Estes et al., 2015; Mirenda et al., 2022; Vivanti et al., 2013), others have not (e.g., Vinen et al., 2022; Vivanti et al., 2014). This is an encouraging message for parents who may not have access to high-intensity autism-specific models of intervention. At this stage, ESDM is not widely available in Australia, including for families in regional or disadvantaged areas. Our findings suggest that accessing the least costly intervention could be the most pragmatic approach for families.
Furthermore, we did not find evidence that parent coaching impacted child outcomes. Rather, children in the No Coaching group showed significant gains in developmental/cognitive skills, in contrast to the Parent Coaching group. This is consistent with evidence that P-ESDM has little effect on child outcomes (Rogers et al., 2019, 2012a, 2012b). It is possible that child outcomes may be associated more with intervention hours, dosage, and child age, than with the parent-delivered component itself. However, given the small sample size of each group in the current study, particularly for the Community Services group, caution must be applied to the interpretation of any potential group differences.
We hypothesised that parents engaged in P-ESDM would show reduced parenting stress compared to other parents; however, we found that on average parents reported more parenting stress over time, which was felt similarly between groups. Furthermore, we did not find clear evidence to suggest that parent coaching benefits parenting sense of competence, and instead found only a non-significant trend for parents in the No Coaching group to experience deteriorating parenting sense of competence over time. Our findings are in contrast to Estes et al. (2014), who found that parents in the P-ESDM group did not report an increase in parenting stress, unlike the community services group; however, Estes et al. also found that parenting sense of competence did not differ between the groups. One possible explanation for these findings is that any association between engaging in parent-mediated intervention and decreased parenting stress may be mediated by parenting sense of competence. Because P-ESDM did not have a clear effect on parenting sense of competence in the current study, participating in P-ESDM may not have positively impacted on parenting stress.
Limitations
Our findings suggest beneficial effects of early intervention for autistic children, with no model having an advantage over another. However, the results should be interpreted within the context that this was a quasi-experimental study associated with access to community-based services. Families were not randomised into the ESDM, G-ESDM, or Community Services groups, and therefore selection bias may be present. The P-ESDM component was randomised, and while our stratification plan achieved comparability for child age and parental mental health for the Parent Coaching and No Coaching groups at baseline, these groups were significantly different on developmental quotient. However, developmental quotient was accounted for in analyses of parent outcomes, and therefore unlikely to have substantially impacted the results. Nonetheless, future studies might consider including developmental quotient when stratifying their groups.
Recruitment spanned 2017–2020, meaning that some data collection occurred during the COVID-19 pandemic. Due to extensive COVID-19 lockdowns in the region through most of 2020 and 2021, some participants in the Community Services group experienced delays in their T2 and T3 assessments. However, these delays did not impact the P-ESDM component, which was completed prior to the pandemic. It is possible that disruption to educational and intervention services during lockdowns may have impacted children’s learning and development. Follow-up data for this cohort is not available, and unfortunately precludes us from examining durability of treatment effects, and any possible impact that COVID-19 lockdowns may have had on development.
The high ratio of male to female children and of mothers to fathers precluded us from examining potential gender effects; future studies may consider making a concerted effort to recruit more autistic girls and their fathers, who are generally under-represented in autism research. Finally, the current study used distal standardised child outcome measures, rather than proximal measures. Proximal measures of child developmental outcomes that are linked to target behaviours may be more sensitive to intervention-related change than standardised measures (Rogers et al., 2012a, 2012b). However, the validity of proximal measures is unknown. While (Rogers et al., 2019) found their proximal measure highly correlated (r = 0.90) with the MSEL, changes were only found on the proximal measure. Ideally a combination of both proximal and distal measures, including follow-up, would be included in future studies.
Future Research
There is a need for low-intensity and cost-effective supports for young autistic children and their caregivers (Lappé et al., 2018). This is particularly true in Australia, where, despite the increasing need for early supports, there has been no proportionate increase in service provision, resulting in a gap that leaves families struggling to cope, especially marginalised families (Australian Government, 2023; Commonwealth of Australia, 2023; Smith et al., 2023). Future trials are needed to evaluate the efficacy of low-intensity, low-resource, and cost-effective supports that have demonstrated promising benefits for autistic children and their parents. Additional focus may be placed on recruitment of autistic girls and their fathers, to allow for examination of gender effects. The addition of proximal measures may provide further insight into change in developmental outcomes, as they may be more sensitive to change. Alternatively, the reliable change index (Jacobson & Truax, 1992) may provide a psychometrically reliable way of measuring individual-level of change. Moreover, different parent outcome measures may be more appropriate for use in parent-mediated interventions (Wainer et al., 2017). Furthermore, identifying potential moderators of parenting sense of competence and parent stress, such as continuity of intervention and support services or participating in parent-mediated intervention, could lead to better supports for parents of young autistic children, and ultimately benefit children.
References
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
Antezana, L., Albright, J., Scarpa, A., Richey, J. A., Laugeson, E. A., & Factor, R. S. (2023). PEERS® for Preschoolers preliminary outcomes and predictors of treatment response. Journal of Autism and Developmental Disorders, 53(12), 4671–4684.
Australian Government. (2023). What we have heard: moving towards development of a National Autism Strategy. Australia
Benson, P. R. (2014). Coping and psychological adjustment among mothers of children with ASD: An accelerated longitudinal study. Journal of Autism and Developmental Disorders, 44(8), 1793–1807.
Benson, P. R. (2020). Examining the links between received network support and marital quality among mothers of children with ASD: A longitudinal mediation analysis. Journal of Autism and Developmental Disorders, 50(3), 960–975.
Berends, D., Bent, C. A., Vivanti, G., Dissanayake, C., & Hudry, K. (2023). Developmental Skills Moderate the Association Between Core Autism Features and Adaptive Behaviour in Early Childhood. Journal of Autism and Developmental Disorders, 1–11.
Carter, M., Roberts, J., Williams, K., Evans, D., Parmenter, T., Silove, N., Clark, T., & Warren, A. (2011). Interventions used with an Australian sample of preschool children with autism spectrum disorders. Research in Autism Spectrum Disorders, 5(3), 1033–1041.
Catalano, D., Holloway, L., & Mpofu, E. (2018). Mental health interventions for parent carers of children with autistic spectrum disorder: Practice guidelines from a critical interpretive synthesis (CIS) systematic review. International Journal of Environmental Research and Public Health, 15(2), 341.
Cheung, R. Y., Leung, S. S., & Mak, W. W. (2019). Role of Mindful Parenting, Affiliate Stigma, and Parents’ Well-being in the Behavioral Adjustment of Children with Autism Spectrum Disorder: Testing Parenting Stress as a Mediator. Mindfulness, 10(11), 2352–2362.
Cleary, D. B., Maybery, M. T., Green, C., & Whitehouse, A. J. (2023). The first six months of life: A systematic review of early markers associated with later autism. Neuroscience and Biobehavioral Reviews, 105304.
Commonwealth of Australia. (2023). Working together to deliver the NDIS - Independent Review into the National Disability Insurance Scheme: Final Report. Australia
Dababnah, S., & Parish, S. L. (2016). Incredible years program tailored to parents of preschoolers with autism: Pilot results. Research on Social Work Practice, 26(4), 372–385.
Daniolou, S., Pandis, N., & Znoj, H. (2022). The efficacy of early interventions for children with autism spectrum disorders: A systematic review and meta-analysis. Journal of Clinical Medicine, 11(17), 5100.
Dawson, G., Rogers, S., Munson, J., Smith, M., Winter, J., Greenson, J., Donaldson, A., & Varley, J. (2010). Randomized, controlled trial of an intervention for toddlers with autism: The Early Start Denver Model. Pediatrics, 125(1), e17–e23.
Derguy, C., & M’bailara, K., Michel, G., Roux, S., & Bouvard, M. (2016). The need for an ecological approach to parental stress in autism spectrum disorders: The combined role of individual and environmental factors. Journal of Autism and Developmental Disorders, 46(6), 1895–1905.
Esler, A., Bal, V., Guthrie, W., Wetherby, A., Weismer, S., & Lord, C. (2015). The autism diagnostic observation schedule, toddler module: Standardized severity scores. Journal of Autism and Developmental Disorders, 45(9), 2407–2720.
Estes, A., Munson, J., Rogers, S. J., Greenson, J., Winter, J., & Dawson, G. (2015). Long-term outcomes of early intervention in 6-year-old children with autism spectrum disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 54(7), 580–587.
Estes, A., Vismara, L., Mercado, C., Fitzpatrick, A., Elder, L., Greenson, J., Lord, C., Munson, J., Winter, J., & Young, G. (2014). The impact of parent-delivered intervention on parents of very young children with autism. Journal of Autism and Developmental Disorders, 44(2), 353–365.
Factor, R. S., Rea, H. M., Dahiya, A. V., Albright, J., Ollendick, T. H., Laugeson, E. A., & Scarpa, A. (2022). An initial pilot study examining child social skills, caregiver styles, and family functioning in the PEERS® for Preschoolers program for young autistic children and their caregivers. Research in Developmental Disabilities, 121, 104152.
Factor, R. S., Rea, H. M., Dahiya, A. V., Laugeson, E. A., & Scarpa, A. (2023a). Pilot Study examining caregiver-child and family functioning in PEERS® for preschoolers. Journal of Child and Family Studies, 32(6), 1694–1707.
Factor, R. S., Rea, H. M., Laugeson, E. A., & Scarpa, A. (2023b). Examining feasibility and outcomes of the PEERS® for preschoolers program. Journal of Autism and Developmental Disorders, 53(5), 1821–1833.
Fuller, E. A., & Kaiser, A. P. (2020). The effects of early intervention on social communication outcomes for children with autism spectrum disorder: A meta-analysis. Journal of Autism and Developmental Disorders, 50(5), 1683–1700.
Green, C. C., Smith, J., Bent, C. A., Chetcuti, L., Sulek, R., Uljarević, M., & Hudry, K. (2021). Differential predictors of well-being versus mental health among parents of pre-schoolers with autism. Autism, 25(4), 1125–1136.
Green, J., Charman, T., McConachie, H., Aldred, C., Slonims, V., Howlin, P., Le Couteur, A., Leadbitter, K., Hudry, K., & Byford, S. (2010). Parent-mediated communication-focused treatment in children with autism (PACT): A randomised controlled trial. The Lancet, 375(9732), 2152–2160.
Green, J., Wan, M. W., Guiraud, J., Holsgrove, S., McNally, J., Slonims, V., Elsabbagh, M., Charman, T., Pickles, A., & Johnson, M. (2013). Intervention for infants at risk of developing autism: A case series. Journal of Autism and Developmental Disorders, 43, 2502–2514.
Hastings, R. P., Daley, D., Burns, C., & Beck, A. (2006). Maternal distress and expressed emotion: Cross-sectional and longitudinal relationships with behavior problems of children with intellectual disabilities. American Journal on Mental Retardation, 111(1), 48–61.
Henry, J., & Crawford, J. (2005). The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. British Journal of Clinical Psychology, 44, 227–239. https://doi.org/10.1348/014466505X29657
Ho, M.-H., & Lin, L.-Y. (2020). Efficacy of parent-training programs for preschool children with autism spectrum disorder: A randomized controlled trial. Research in Autism Spectrum Disorders, 71, 101495.
Ingersoll, B., & Hambrick, D. Z. (2011). The relationship between the broader autism phenotype, child severity, and stress and depression in parents of children with autism spectrum disorders. Research in Autism Spectrum Disorders, 5(1), 337–344.
Jacobson, N. S., & Truax, P. (1992). Clinical significance: a statistical approach to defining meaningful change in psychotherapy research.
Janvier, D., Choi, Y. B., Klein, C., Lord, C., & Kim, S. H. (2022). Brief report: Examining test-retest reliability of the autism diagnostic observation schedule (ADOS-2) calibrated severity scores (CSS). Journal of Autism and Developmental Disorders, 1–7.
Jhuo, R.-A., & Chu, S.-Y. (2022). A review of parent-implemented early start Denver model for children with autism spectrum disorder. Children, 9(2), 285.
Johnston, C., & Mash, E. J. (1989). A measure of parenting satisfaction and efficacy. Journal of Clinical Child Psychology, 18(2), 167–175.
Jurek, L., Occelli, P., Denis, A., Amestoy, A., Maffre, T., Dauchez, T., Oreve, M.-J., Baghdadli, A., Schroder, C., & Jay, A. (2021). Efficacy of parent-mediated communication-focused treatment in toddlers with autism (PACT) delivered via videoconferencing: A randomised controlled trial study protocol. British Medical Journal Open, 11(4), e044669.
Karp, S. M., Lutenbacher, M., & Wallston, K. A. (2015). Evaluation of the parenting sense of competence scale in mothers of infants. Journal of Child and Family Studies, 24, 3474–3481.
Kasari, C., Freeman, S., & Paparella, T. (2006). Joint attention and symbolic play in young children with autism: A randomized controlled intervention study. Journal of Child Psychology and Psychiatry, 47(6), 611–620.
Konstantareas, M. M., Homatidis, S., & Plowright, C. (1992). Assessing resources and stress in parents of severely dysfunctional children through the Clarke modification of Holroyd’s Questionnaire on Resources and Stress. Journal of Autism and Developmental Disorders, 22(2), 217–234.
Lappé, M., Lau, L., Dudovitz, R. N., Nelson, B. B., Karp, E. A., & Kuo, A. A. (2018). The diagnostic odyssey of autism spectrum disorder. Pediatrics, 141(Supplement_4), S272-S279.
Lau, J. S.-P., Lai, S. M.-K., Ip, F. T.-S., Wong, P. W.-C., Team, W., Servili, C., Salomone, E., Pacione, L., Shire, S., & Brown, F. L. (2022). Acceptability and feasibility of the World Health Organization's Caregiver Skills Training Programme (WHO CST) delivered via eLearning, videoconferencing, and in-person hybrid modalities in Hong Kong. Frontiers in psychiatry, 1855.
Lau, W.Y.-P., Gau, S.S.-F., Chiu, Y.-N., & Wu, Y.-Y. (2014). Autistic traits in couple dyads as a predictor of anxiety spectrum symptoms. Journal of Autism and Developmental Disorders, 44(11), 2949–2963.
Leadbitter, K., Aldred, C., McConachie, H., Le Couteur, A., Kapadia, D., Charman, T., Macdonald, W., Salomone, E., Emsley, R., & Green, J. (2018). The autism family experience questionnaire (AFEQ): An ecologically-valid, parent-nominated measure of family experience, quality of life and prioritised outcomes for early intervention. Journal of Autism and Developmental Disorders, 48(4), 1052–1062.
Lord, C., Rutter, M., DiLavore, P., Risi, S., Gotham, K., & Bishop, S. (2012). Autism Diagnostic Observation Schedule, 2nd Edition (ADOS-2). Western Psychological Services.
Lovibond, S., & Lovibond, P. (1995). Manual for the Depression Anxiety Stress Scales (2 ed.). Psychological Foundation.
Mathew, N. E., Burton, K. L., Schierbeek, A., Črnčec, R., Walter, A., & Eapen, V. (2019). Parenting preschoolers with autism: Socioeconomic influences on wellbeing and sense of competence. World Journal of Psychiatry, 9(2), 30.
Mirenda, P., Colozzo, P., Smith, V., Kroc, E., Kalynchuk, K., Rogers, S. J., & Ungar, W. J. (2022). A randomized, community-based feasibility trial of modified ESDM for toddlers with suspected autism. Journal of Autism and Developmental Disorders, 1–20.
Mullen, E. M. (1995). Mullen Scales of Early Learning (AGS ed.). American Guidance Service, Inc.
van Noorden, L. E., Sigafoos, J., & Waddington, H. L. (2022). Evaluating a Two-Tiered Parent Coaching Intervention for Young Autistic Children Using the Early Start Denver Model. Advances in Neurodevelopmental Disorders, 1–21.
Ohan, J. L., Leung, D. W., & Johnston, C. (2000). The parenting sense of competence scale: Evidence of a stable factor structure and validity. Canadian Journal of Behavioural Science/revue Canadienne Des Sciences Du Comportement, 32(4), 251.
Padden, C., & James, J. E. (2017). Stress among parents of children with and without autism spectrum disorder: A comparison involving physiological indicators and parent self-reports. Journal of Developmental and Physical Disabilities, 29(4), 567–586.
Palmer, M., Cáceres, S. J., & A., Tarver, J., Howlin, P., Slonims, V., Pellicano, E., & Charman, T. (2020). Feasibility study of the National Autistic Society EarlyBird parent support programme. Autism, 24(1), 147–159.
Pickles, A., Le Couteur, A., Leadbitter, K., Salomone, E., Cole-Fletcher, R., Tobin, H., Gammer, I., Lowry, J., Vamvakas, G., & Byford, S. (2016). Parent-mediated social communication therapy for young children with autism (PACT): Long-term follow-up of a randomised controlled trial. The Lancet, 388(10059), 2501–2509.
Pruitt, M. M., Rhoden, M., & Ekas, N. V. (2018). Relationship between the broad autism phenotype, social relationships and mental health for mothers of children with autism spectrum disorder. Autism, 22(2), 171–180.
Quintero, N., & McIntyre, L. L. (2010). Sibling adjustment and maternal well-being: An examination of families with and without a child with an autism spectrum disorder. Focus on Autism and Other Developmental Disabilities, 25(1), 37–46.
Rogers, H., & Matthews, J. (2004). The parenting sense of competence scale: Investigation of the factor structure, reliability, and validity for an Australian sample. Australian Psychologist, 39(1), 88–96.
Rogers, S. J., & Dawson, G. (2010). Early Start Denver Model for Young Children with Autism: Promoting language, learning, and engagement. Guilford Press.
Rogers, S. J., Dawson, G., & Vismara, L. A. (2012a). An early start for your child with autism: Using everyday activities to help kids connect, communicate, and learn. Guilford Press.
Rogers, S. J., Estes, A., Lord, C., Vismara, L., Winter, J., Fitzpatrick, A., Guo, M., & Dawson, G. (2012b). Effects of a brief Early Start Denver Model (ESDM)–based parent intervention on toddlers at risk for autism spectrum disorders: A randomized controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry, 51(10), 1052–1065.
Rogers, S. J., Estes, A., Vismara, L., Munson, J., Zierhut, C., Greenson, J., Dawson, G., Rocha, M., Sugar, C., & Senturk, D. (2019). Enhancing low-intensity coaching in parent implemented Early Start Denver Model intervention for early autism: A randomized comparison treatment trial. Journal of Autism and Developmental Disorders, 49(2), 632–646.
Rogers, S. J., Stahmer, A., Talbott, M., Young, G., Fuller, E., Pellecchia, M., Barber, A., & Griffith, E. (2022). Feasibility of delivering parent-implemented NDBI interventions in low-resource regions: A pilot randomized controlled study. Journal of Neurodevelopmental Disorders, 14, 1–14.
Salomone, E., Settanni, M., McConachie, H., Suma, K., Ferrara, F., Foletti, G., Salandin, A., Shire, W. C. T. F. L. B. L. P. S., Servili, C., & Adamson, L. B. (2021). Pilot randomized controlled trial of the WHO caregiver skills training in public health services in Italy. Journal of Autism and Developmental Disorders, 1–15.
Salomone, E., Leadbitter, K., Aldred, C., Barrett, B., Byford, S., Charman, T., Howlin, P., Green, J., Le Couteur, A., & McConachie, H. (2018). The association between child and family characteristics and the mental health and wellbeing of caregivers of children with autism in mid-childhood. Journal of Autism and Developmental Disorders, 48(4), 1189–1198.
Salomone, E., Pacione, L., Shire, S., Brown, F. L., Reichow, B., & Servili, C. (2019). Development of the WHO caregiver skills training program for developmental disorders or delays. Frontiers in Psychiatry, 10, 769.
Sandbank, M., Bottema-Beutel, K., Crowley, S., Cassidy, M., Dunham, K., Feldman, J. I., Crank, J., Albarran, S. A., Raj, S., & Mahbub, P. (2020). Project AIM: Autism intervention meta-analysis for studies of young children. Psychological Bulletin, 146(1), 1.
Schertz, H. H., Lester, J. N., Erden, E., Safran, S., & Githens, P. (2020). Challenges and contributors to self-efficacy for caregivers of toddlers with autism. Autism, 24(5), 1260–1272.
Schnabel, A., Youssef, G. J., Hallford, D. J., Hartley, E. J., McGillivray, J. A., Stewart, M., Forbes, D., & Austin, D. W. (2020). Psychopathology in parents of children with autism spectrum disorder: A systematic review and meta-analysis of prevalence. Autism, 24(1), 26–40.
Sengupta, K., Shah, H., Ghosh, S., Sanghvi, D., Mahadik, S., Dani, A., Deshmukh, O., Pacione, L., Dixon, P., & Salomone, E. (2023). World health organisation-caregiver skills training (WHO-CST) Program: Feasibility of delivery by non-specialist providers in real-world urban settings in India. Journal of Autism and Developmental Disorders, 53(4), 1444–1461.
Smith, J., Sulek, R., Green, C. C., Bent, C. A., Chetcuti, L., Bridie, L., Benson, P. R., Barnes, J., & Hudry, K. (2021). Relative predictive utility of the original and Autism-Specific Five-Minute Speech Samples for child behaviour problems in autistic preschoolers: A preliminary study. Autism, 13623613211044336.
Smith, J., Aulich, A., Bent, C. A., Constantine, C., Franks, K., Goonetilleke, N., Green, C. C., Lee, P., Ma, E., & Said, H. (2023). “What is early intervention? I had no idea”: Chinese parents’ experiences of early supports for their autistic children in Australia. Research in Autism Spectrum Disorders, 108, 102227.
Smith, J., Sulek, R., Abdullahi, I., Green, C. C., Bent, C. A., Dissanayake, C., & Hudry, K. (2021a). Comparison of mental health, well-being and parenting sense of competency among Australian and South-East Asian parents of autistic children accessing early intervention in Australia. Autism, 25(6), 1784–1796.
Sparrow, S., Cicchetti, D., & Balla, D. (2005). The Vineland Adaptive Behavior Scales, 2nd Edition (VABS-II). NCS Pearson Inc.
Stewart-Brown, S. L., Platt, S., Tennant, A., Maheswaran, H., Parkinson, J., Weich, S., Tennant, R., Taggart, F., & Clarke, A. (2011). The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): A valid and reliable tool for measuring mental well-being in diverse populations and projects. Journal of Epidemiology and Community Health, 65(Suppl 2), A38–A39.
Sussman, F. (1999). More Than Words: Helping parents promote communication and social skills in children with autism spectrum disorder. The Hanen Centre.
Swineford, L. B., Guthrie, W., & Thurm, A. (2015). Convergent and divergent validity of the Mullen Scales of Early Learning in young children with and without autism spectrum disorder. Psychological Assessment, 27(4), 1364.
Tachibana, Y., Miyazaki, C., Ota, E., Mori, R., Hwang, Y., Kobayashi, E., Terasaka, A., Tang, J., & Kamio, Y. (2017). A systematic review and meta-analysis of comprehensive interventions for pre-school children with autism spectrum disorder (ASD). PLoS ONE, 12(12), e0186502.
Tanner, A., & Dounavi, K. (2021). The emergence of autism symptoms prior to 18 months of age: A systematic literature review. Journal of Autism and Developmental Disorders, 51(3), 973–993.
Team, J. (2023). JASP. In (Version 0.17.1.0)
Tennant, R., Hiller, L., Fishwich, R., Platt, S., Joseph, S., Weich, S., Parkinson, J., Secker, J., & Stewart-Brown, S. (2007a). The Warwick-Edinburgh mental well-being scale (WEMWBS): Development and UK validation. Health and Quality of Life Outcomes, 5(1), 63.
Tennant, R., Hiller, L., Fishwick, R., Platt, S., Joseph, S., Weich, S., Parkinson, J., Secker, J., & Stewart-Brown, S. (2007b). The Warwick-Edinburgh mental well-being scale (WEMWBS): Development and UK validation. Health and Quality of Life Outcomes, 5(1), 63.
Van’t Hof, M., Tisseur, C., van Berckelear-Onnes, I., van Nieuwenhuyzen, A., Daniels, A. M., Deen, M., Hoek, H. W., & Ester, W. A. (2021). Age at autism spectrum disorder diagnosis: A systematic review and meta-analysis from 2012 to 2019. Autism, 25(4), 862–873.
Vernhet, C., Dellapiazza, F., Blanc, N., Cousson-Gélie, F., Miot, S., Roeyers, H., & Baghdadli, A. (2019). Coping strategies of parents of children with autism spectrum disorder: A systematic review. European Child and Adolescent Psychiatry, 28(6), 747–758.
Vinen, Z., Clark, M., & Dissanayake, C. (2022). Social and Behavioural Outcomes of School Aged Autistic Children Who Received Community-Based Early Interventions. Journal of Autism and Developmental Disorders, 1–12.
Vismara, L. A., McCormick, C. E., Wagner, A. L., Monlux, K., Nadhan, A., & Young, G. S. (2018). Telehealth parent training in the Early Start Denver Model: Results from a randomized controlled study. Focus on Autism and Other Developmental Disabilities, 33(2), 67–79.
Vivanti, G., Dissanayake, C., Duncan, E., Feary, J., Capes, K., Upson, S., Bent, C. A., Rogers, S. J., & Hudry, K. (2019). Outcomes of children receiving group-early start Denver model in an inclusive versus autism-specific setting: A pilot randomized controlled trial. Autism, 23(5), 1165–1175.
Vivanti, G., Dissanayake, C., Zierhut, C., & Rogers, S. J. (2013). Brief report: Predictors of outcomes in the Early Start Denver Model delivered in a group setting. Journal of Autism and Developmental Disorders, 43(7), 1717–1724.
Vivanti, G., Paynter, J., Duncan, E., Fothergill, H., Dissanayake, C., & Rogers, S. J. (2014). Effectiveness and feasibility of the Early Start Denver Model implemented in a group-based community childcare setting. Journal of Autism and Developmental Disorders, 44(12), 3140–3153.
Vivanti, G., Dissanayake, C., & Victorian ASELCC Team. (2016). Outcome for children receiving the Early Start Denver Model before and after 48 months. Journal of Autism and Developmental Disorders, 46(7), 2441–2449.
Wainer, A. L., Hepburn, S., & McMahon Griffith, E. (2017). Remembering parents in parent-mediated early intervention: An approach to examining impact on parents and families. Autism, 21(1), 5–17.
Whitehouse, A. J., Varcin, K. J., Pillar, S., Billingham, W., Alvares, G. A., Barbaro, J., Bent, C. A., Blenkley, D., Boutrus, M., & Chee, A. (2021). Effect of preemptive intervention on developmental outcomes among infants showing early signs of autism: A randomized clinical trial of outcomes to diagnosis. JAMA Pediatrics, 175(11), e213298–e213298.
Yamada, A., Suzuki, M., Kato, M., Suzuki, M., Tanaka, S., Shindo, T., Taketani, K., Akechi, T., & Furukawa, T. A. (2007). Emotional distress and its correlates among parents of children with pervasive developmental disorders. Psychiatry and Clinical Neurosciences, 61(6), 651–657.
Zhou, B., Xu, Q., Li, H., Zhang, Y., Wang, Y., Rogers, S. J., & Xu, X. (2018). Effects of parent-implemented Early Start Denver Model intervention on Chinese Toddlers with autism spectrum disorder: A non-randomized controlled trial. Autism Research, 11(4), 654–666.
Acknowledgements
The Victorian Autism Specific Early Learning and Care Centre (ASELCC) Team: Kristy Capes, Jessica Feary, Carolyne Jones, Abby Marshall, Dianna Rodset, Shannon Upson. We thank the children and their parents for their participation in this study. We also thank staff at the Victorian ASELCC and La Trobe University Community Children’s Centre for supporting family engagement, as well as the following colleagues who supported data collection activities: Alexandra Aulich, Daniel Berends, Lillian Bridie, Zoe Lazaridis, Marissa Leisos, Katherine Natoli, Madeleine Russell-Maynard. Funding was provided by the Australian Government Department of Social Services (DSS). MU was funded by a Discovery Early Career Researcher Award (DECRA) from the Australian Research Council. The funders have had no role in the study design, manuscript drafting or decision to submit the manuscript for publication.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interests
The Victorian ASELCC Team and authors KP, and GT have been employed by and received salary to provide early intervention services to children/families participating in this study alongside their enrolment at the La Trobe University Community Children’s Centre. Authors CG, CB, JS, LC, and KH have previously received salary from grant funding to conduct research with families enrolled at the Victorian ASELCC and related work, including the current study, and thus held prior affiliations with this clinical provider.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Green, C.C., Bent, C.A., Smith, J. et al. An Evaluation of Child and Parent Outcomes Following Community-Based Early Intervention with Randomised Parent-Mediated Intervention for Autistic Pre-Schoolers. Child Youth Care Forum (2024). https://doi.org/10.1007/s10566-024-09792-x
Accepted:
Published:
DOI: https://doi.org/10.1007/s10566-024-09792-x