
Abstract
Background
Non-erosive reflux disease (NERD) includes a heterogeneous patient group with varying clinical and pathophysiological characteristics. This study aims to elucidate the pathogenesis of persistent NERD despite of continuous proton-pump inhibitors (PPI) treatment using 24-h combined multichannel intraluminal impedance-pH monitoring (MII-pH).
Methods
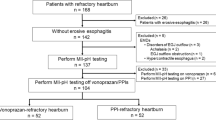
We enrolled fifty-four consecutive Japanese patients with typical gastroesophageal reflux disease symptoms, despite treatment with 10-mg rabeprazole twice daily. All patients underwent upper endoscopy, esophageal high-resolution manometry (HRM), and 24-h MII-pH monitoring.
Results
Twenty-nine (53.7 %) of the patients had a positive and 25 (46.3 %) had a negative Symptom Index (SI). The number of mean reflux episodes over 24 h in an upright position was significantly greater in the SI-positive than the SI-negative group. The majority of episodes were non-acid reflux, while the proportion of proximal reflux episodes consisting of non-acid, liquid or mixed components were significantly greater in the SI-positive group in comparison to the SI-negative group (50.4 vs. 33.1 %, P < 0.001, 46.1 vs. 32.3 %, P < 0.001, 54.4 vs. 40.9 %, P < 0.001, respectively). The SI-positive group had a higher rate of abnormal motility as measured by HRM.
Conclusions
Reflux reaching the proximal esophagus and defective esophageal motility play key roles in the pathogenesis of NERD. The majority of PPI-resistant NERD patients showed no association with acid reflux. The SI patterns suggest that NERD patients are a heterogeneous group. Therefore, therapy may be tailored to each patient according to SI patterns.


Similar content being viewed by others


References
Fujiwara Y, Arakawa T. Epidemiology and clinical characteristic of GERD in the Japanese population. J Gastroenterol. 2009;44:518–34.
Kahrilas PJ. Gastroesophageal reflux disease. JAMA. 1996;276:983–8.
Fass R. Erosive esophagitis and nonerosive reflux disease (NERD): comparison of epidemiologic, physiologic, and therapeutic characteristics. J Clin Gastroenterol. 2007;41:131–7.
Fass R. Epidemiology and pathophysiology of symptomatic gastroesophageal reflux disease. Am J Gastroenterol. 2003;98:S2–7.
Quigley EM. Gastroesophageal reflux disease: spectrum or continuum? QJM. 1997;90:75–8.
Adachi K, Hashimoto T, Hamamoto N, Hirakawa K, Niigaki M, Miyake T, Tanimura H, Ono M, Kaji T, Suetsugu H, Yagi J, Kamazawa Y, Mihara T, Katsube T, Fujishiro H, Shizuku T, Hattori S, Yamamoto S, Kinoshita Y. Symtom relief in patients with reflux esophagitis:comparative study of omeprazole, lansoprazole and rabeprazole. J Gastroenterol Hepatol. 2003;18:1392–8.
Dean BB, Gano AD Jr, Knight K, Ofman JJ, Fass R. Effective of proton pump inhibitors in nonerosive reflux disease. Clin Gastroenterol Hepatol. 2004;2:656–64.
Furuta T, Shimatani T, Sugimoto M, Ishihara S, Fujiwara Y, Kusano M, Koike T, Hongo M, Chiba T, Kinoshita Y. The Acid-Related Symptom Research Group. J Gastroenterol. 2011;46:1273–83.
Frazzoni M, Canigliaro R, Melotti G. Weakly acidic refluxes have a major role in the pathogenesis of proton pump inhibitor-resistant oesophagitis. Aliment Pharmacol Ther. 2011;33:601–6.
Tsoukali E, Sifrim D. The role of weakly acidic reflux in proton pump inhibitor failure, has dust settled? J Neurogastroenterol Motil. 2010;16:258–64.
Tamhankar AP, Peters JH, Portale G, Hsieh CC, Hagen JA, Bremner CG, et al. Omeprazole dose not reduce gastroesophageal reflux: new insights using multichannel intraluminal impedance technology. J Gastrointest Surg. 2004;8:890–7 (discussion 897–898).
Vela MF, Camacho-Lobato L, Srinivasan R, Tutuian R, Katz PO, Castell DO. Simultaneous intraesophageal impedance and pH measurement of acid and nonacid gastroesophageal reflux: effect of omeprazole. Gastroenterology. 2001;120:1599–606.
Wiener GJ, Richter JE, Cooper JB, et al. The symptom index: a clinically important parameter of ambulatory 24-hour esophageal pH monitoring. Am J Gastroenterol. 1988;83:358–9.
Sifrim D, Castell D, Dent J, Kaharilus PJ. Gastro-oesophageal reflux monitoring: review and consensus report on detection and definitions of acid, non-acid, and gas reflux. Gut. 2004;53:1024–31.
Bredenoord AJ, Fox M, Kahrilas PJ, Pandolfino JE, Schwizer W, Smout AJPM. Chicago classification criteria of esophageal motility disorders defined in high resolution esophageal pressure topography. Neurogastroenterol Motil. 2012;24:57–65.
Weusten B, Roelofs JM, Akkermans LM, Van Berge Henegouwen GP, Smout AJ. The symptom-association probability: an improved method for symptom analysis of 24-hour esophageal pH data. Gastroenterology. 1994;107:1741–5.
Savarino E, Zentilin P, Tutuian R, Pohl D, Casa D, Frazzoni M, Cestari R, Savarino V. The role of non-acid reflux in NERD-lessons learned from impedance-pH monitoring in 150 patients off therapy. Am J Gastroenterol. 2008;103:2685–93.
MaColl E, Junghard O, Wiklund I, Revicki DA. Assessing symptom in gastroesophageal reflux disease: how well do clinician’s assessments agree with hose of their patients? Am J Gastroenterol. 2005;100:11–8.
Zerbib F, Duriez A, Roman S, Capdepont M, Mion F. Determinants of gastro-oesophageal reflux perception in patients with persistent symptoms despite proton pump inhibitors. Gut. 2008;57:56–60.
Emerenziani S, Ribolsi M, Sifrim D, Bkondeau K, Cicala M. Regional oesophageal sensitivity to acid and weakly acidic reflux in patients with non-erosive reflux disease. Neurogastroenterol Motil. 2009;21:253–8.
Iwakiri K, Sano H, Tanaka M, Kawami N, Umezawa M, Futagami S, Hoshihara Y, Nomura T, Miyashita M, Sakamoto C. Characteristics of symptomatic reflux episodes in patients with non-erosive reflux disease who have a positive symptom index on proton pump inhibitor therapy. 2010;82:156–61.
Penagini R, Heobard G, Horowitz M, et al. Motor function of the proximal stomach and visceral perception in gastro-oesophageal reflux disease. Gut. 1998;43:251–7.
Bhat YM, Bielefeldt K. Capsaicin receptor (TRPV1) and non-erosive reflux disease. Eur J Gastroenterol Hepatol. 2006;18:263–70.
Karamanolis G, Stevens W, Vos R, Tack J, Clave P, Sifrim D. Oesophageal tone and sensation in the transition zone between proximal striated and distal smooth muscle oesophagus. Neurogastroenterol Motil. 2008;20:291–7.
Sengupta JN, Kauvar D, Goyal R. Characteristics of vagal esophageal tension-sensitive afferent fibers in the opossum. J Neurophysiol. 1989;61:1001–10.
Savarino E. Impedance-pH reflux patterns can differentiate non-erosive reflux disease from functional heartburn patients. J Gastroenterol. 2012;49:159–68.
MartineK J, Benes M, Hucl T, Drastich P, Stirand P, Spicak J. Non-erosive and erosive gastroesophageal reflux disease: no difference with regard to reflux pattern and motility abnormalities. Scand J Gastroenterol. 2008;43:794–800.
Wu JC, Cheung CM, Wong VW, Sung JJ. Distinct clinical characteristics between patients with nonerosive reflux disease and those with reflux esophagitis. Clin Gastroenterol Hepatol. 2007;5:690–5.
Frazzoni M, Manta R, Mirante VG, Conigliaro R, Frazzoni L, Melotti G. Esophageal chemical clearance is impaired in gastro-esophageal reflux disease—a 24-h impedance-pH monitoring assessment. Neurogastroenterol Motil. 2013;25:399–406.
Sifrim D, Mittal R, Fass R, Smout A, Castell D, Tack J, Gregersen H (2007) Acidity and volume of the refluxare in the genesis of gastroesophageal reflux disease symptom. Aliment Pharmacol Ther 23:1003-1-15.
Chen Chien-Lin, Yi Chih-Hsun, Liu Tso-Tsai. Relevance of ineffective esophageal motility to secondary peristalsis in patients with gastroesophageal reflux disease. J Gastroenterol and Hepatol. 2014;29:296–300.
Kasapidis P, Xynos E, Mantides A, Chrysos E, Demonakou M, Nikolopoulos N, Vassilakis JS. Differences in manometry and 24-h ambulatory pH-metry between patients with and without endoscopic or histological esophagitis in gastroesophageal reflux disease. Am J Gastroenterol. 1993;88:1893–9.
Modlin IM, Hunt FH, Malfertheiner P, Moayyedi P, Quigley EM, Tytgat GNJ, Tack J, Headung RC, Holtman G, Moss SF, on behalf of the Vevey NERD Consensus Group. Diagnosis and management of non-erosive reflux disease—The Vevey NERD Consensus Group. Digestion. 2009;80:74–88.
Galmiche JP, Hatlebakk J, Attwood S, Ell C, Fiocca R, Eklund S, Langstrom G, Lind T, Lundell L. Laparoscopic antireflux surgery vs. esomeprazole treatment for chronic GERD the LOTUS randomized clinical trial. JAMA. 2011;19:1969–77.
Zhang Q, Lehmann A, Rigda R, Dent J, Holloway RH. Control of transient lower oesophageal sphincter relaxations and reflux by the GABAB agonist baclofen in patients with gastro-oesophageal reflux disease. Gut. 2002;50:19–24.
Orr WC, Goodrich S, Wright S, Shepherd K, Mellow M. The effect of baclofen on nocturnal gastroesophageal reflux and measures of sleep quality: a randomized, cross-over trial. Neurogastroenterol Motil. 2012;24:553–9.
Ciccaglione AF, Marzio L. Effect of acute and chronic administration of the GABAB agonist baclofen on 24 hour pH metry and symptoms in control subjects and in patients with gastro-esophageal reflux disease. Gut. 2003;52:464–70.
Medici M, Pebet M, Ciblis D. A double-blind, long term study of tizanidine(‘Sirdalud’) in spasticity due to cerebrovascular lesion. Curr Med Res Opin. 1989;11:398–407.
Blondeau R. Treatment of gastro-esophageal reflux disease: the new kids to block. Neurogastroenterol Motil. 2010;22:836–40.
Ethical Statement
We conformed with the Helsinki Declaration of 1975, as revised in 2000 and 2008 concerning Human and Animal Rights, and that we followed out policy concerning Informed Consent as shown on Springer.com.
Conflict of interest
The authors have no conflict of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Yamashita, H., Ashida, K., Kawaguchi, S. et al. The pathogenesis of persistent non-erosive reflux disease treated with proton-pump inhibitors as measured with the Symptom Index. Esophagus 12, 50–56 (2015). https://doi.org/10.1007/s10388-014-0452-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10388-014-0452-6