
Abstract
Objectives
The aim of this systematic review was to evaluate the prognosis of at-home dental bleaching using low concentration bleaching products.
Materials and methods
This review was conducted was performed following the recommendations of the 2020 PRISMA statement and was registered in the International Prospective Register of Systematic Reviews (PROSPERO-CRD42022360530). The PICO question was “What is the prognosis of home teeth whitening treatment?”. An advanced electronic search was made in three databases: PubMed, Web of Science, and Embase.
Results
The database search led to the retrieval of 225 articles. After elimination of duplicate references, the titles and abstracts of the articles were analyzed with respect to the eligibility criteria, and 24 studies were included for the development of the systematic review.
Conclusions
Most authors state that the color remains stable between 1 and 2.5 years regardless of the type of bleaching agent or the forms of administration, and color stability in cases of severe discolorations presents a higher degree of recurrence.
Clinical relevance
Given the growing demand for dental cosmetic treatments, the following systematic review may aid the clinician’s continuing education and evidence-based practice by providing knowledge on the field of at-home dental bleaching agents and their long-term effects.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Nowadays, esthetic procedures are widely required in daily dental practice. Patients seeking an attractive smile have been increasing significantly, especially in terms of tooth color [1]. Dental bleaching is considered the treatment of choice to improve patient satisfaction in terms of tooth discoloration, due to its non-invasive approach and low cost compared to other cosmetic dentistry procedures [2]. Many types of color problems can affect the appearance of teeth, and the causes of tooth discoloration must be carefully evaluated to establish a correct diagnosis [3, 4].
Discolorations are classified as either extrinsic or intrinsic. Extrinsic discolorations result from the accumulation of chromogenic substances on the external surface of the tooth [3,4,5]. They are secondary to the habitual intake of chromogenic dietary sources such as wine, coffee, tea, carrots, oranges, chocolate, tobacco, some mouthwashes, or poor or incorrect oral hygiene habits. These discolorations, most of the times, can be eliminated mechanically by professional prophylaxis treatments [3,4,5,6,7].
As for intrinsic discolorations, they occur after a change in the structural composition or thickness of the dental tissues. They can be caused by systemic or local factors. Systemic causes include those related to drugs (e.g., tetracycline), alterations in the structure or thickness of dental tissues [5, 7]. Local causes include pulp necrosis, intrapulpal hemorrhage, remnants of pulp tissue in the chamber after root canal treatment, root canal filling materials, some coronal restorative materials, enamel microcracks, caries, and aging. These discolorations are treated by tooth bleaching techniques [3,4,5,6, 8]. Historically, bleaching techniques were introduced to the clinic in 1848 as a treatment for discolorations of non-vital teeth, using chloride of lime [9]. In 1864, Truman introduced a more effective technique for bleaching non-vital teeth that consisted in the application of a solution formed by chlorine and acetic acid [10].
At the end of the nineteenth century, other bleaching agents such as potassium cyanide, oxalic acid, sulfurous acid, aluminum chloride, sodium hypophosphate, pyrozone, hydrogen dioxide, and sodium peroxide were also successfully used in bleaching non-vital teeth [11,12,13,14,15,16]. Finally, in 1868, whitening techniques for vital teeth were introduced, using oxalic acid, pyrozone, and later hydrogen peroxide (HP) [11,12,13,14,15,16]. Dental bleaching techniques can be classified into vital and non-vital bleaching techniques. The former are classified as: in-office bleaching, at-home bleaching supervised by the dentist and at-home bleaching without supervision, using over-the-counter bleaching products [17].
Bleaching in the clinic uses bleaching products in high concentrations (25–40% HP). This procedure is carried out after having performed some previous maneuvers such as hard tissue prophylaxis and soft tissue protection through the application of physical barriers. The agents applied can be activated chemically or by light [18]. Alternatively, at-home dental bleaching involves the use of bleaching products with lower concentrations [5]. Originally, these techniques consisted of the application of 10% carbamide peroxide (CP) in individualized splints applied overnight (6–8 h). Currently, gels with concentrations up to 20% are applied [1, 19, 20].However, the industry has developed products that act more quickly compared to those described above and are more attractive to some patients. These products are presented in the form of gels containing HP in concentrations between 3 and 10%, mainly applied during the day [21, 22].
Supervision by the dentist takes place during check-up appointments [1, 19,20,21,22,23]. The advantages of this technique include: self-administration by the patient, less time in the dental chair, high degree of safety, fewer adverse effects, and low cost [24]. The disadvantages include the need for high patient collaboration since the result is linked to the diligence with which the indicated guidelines are respected. Excessive or prolonged use of the treatment may cause increased tooth sensitivity and soft tissue irritation. Sometimes both techniques can be combined [11, 24].
The third technique, also known as “over-the-counter,” involves the use of over-the-counter products containing low concentration bleaching agents. These products are purchased and applied without professional supervision and come in the form of toothpaste, whitening strips, mouthwashes, and prefabricated splints [5, 25].
The literature describes a wide variety of protocols and methods for applying the products described above, although there is still no single accepted protocol [23]. As for the stability of the color obtained after bleaching, this depends to a large extent on diet and habits as they contribute to the development of extrinsic discolorations [5].
The literature on the effectiveness of home bleaching is abundant and has already been reviewed [26, 27]. The term “effectiveness” refers to the ability of dental bleaching to produce an effect (color change). Alternatively, the term “prognosis” defines the stability and duration of the obtained effect, maintained over time. A series of studies on the prognosis of home dental bleaching have been performed. However, no efforts have been made to assess such evidence. Thus, the aim of this systematic review is to perform a qualitative synthesis of available studies on the prognosis of home dental bleaching using low-concentration products on vital teeth, in terms of duration of the effects achieved after being exposed to the treatment.
Materials and methods
Protocol and registration
This study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO-CRD42022360530).
Search strategy
This systematic review of the literature was performed following the recommendations of the PRISMA statement updated in 2020 [28]. A literature search was conducted in digital databases PubMed, Web of Science, and Embase in May 2022 and was updated on the 29th of March 2023. No language or time restrictions were applied. The search strategy employed three main fields: field #1, keywords regarding prognosis (prognosis or dura*); field #2, keywords regarding dental bleaching (“tooth bleaching” or “teeth bleaching” or “dental bleaching” or “dental whitening” or bleaching or whitening); and field #3, keywords regarding at-home dental bleaching specifically (home). Keyword selection was based on the descriptors used in previous studies in the field. Whenever possible, both controlled and uncontrolled terms were used. See Supplementary Table 1 for the specific search strategy for each database. Restrictions to publication date and language were not applied. The PICO question guiding the search was: What is the prognosis of home dental bleaching treatment? Which can be subdivided as follows:
P (population): individuals undergoing home dental bleaching; I (intervention): home bleaching using specific low concentration bleaching agent/s with specific application method/s; C (comparison): home bleaching using other specific low concentration bleaching agent/s and/or other specific application method/s; and O (outcomes).
The search strategy, study selection process, data extraction, and quality assessment (risk of bias assessment) were performed by two independent investigators (R.F. and M.M). In case of doubt, a third investigator was consulted (JL.S).
Eligibility criteria
Studies were selected based on previously established inclusion criteria: (1) RCT; (2) clinical trials; (3) home bleaching protocols using HP in concentrations lower than 10% or CP in concentrations lower than 28%, with post-treatment follow-up times of no less than 2 months; (4) in vivo studies in patients of any age group. Studies in which in-office bleaching protocols were applied with concentrations not dispensable for home use, combined bleaching techniques, home VS in-office bleaching techniques, retrospective studies, in vitro, cohort, clinical cases, and case series were excluded.
Study selection, data extraction, and synthesis of the evidence
All the selected articles were imported into a citation management software (Mendeley. Elsevier, Amsterdam, Netherlands), and duplicate articles were eliminated. A first screening of the articles according to title and abstract was then performed according to the search strategy described above, and finally a second screening of the full text of the eligible studies was performed.
The following bibliometric data were extracted from each study: author and year of publication. As for the methodological variables, the following were extracted: study type, diagnostic method, number of participants and dropout, bleaching protocol, bleaching product application method, age range, and bleaching method. Lastly, the following outcome variables were extracted: results in terms of DSGU/ΔE; results in terms of color change in ΔE values (if spectrophotometer was used); and results in terms of color change in DSGU (shade guide unit) values (if a shade guide was used).
After data extraction, a synthesis of the evidence was performed. To do so, the extracted variables were assessed to search for similarities and/or contradictions among the included studies’ results. Lastly, a qualitative synthesis of the studies’ data regarding the primary outcomes of this review (prognosis of home bleaching, measured over time by analysis of ΔE and color change in DSGU dental units) was performed.
Quality assessment
Quality assessment of the selected studies was carried out using Cochrane Collaboration tools for risk of bias: ROB-2 for randomized controlled trials (RCTs) and ROBINS-I for controlled trials (CTs) [29]. No other analyses could be performed due to the heterogeneity of the data.
Results
Study selection
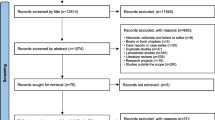
The database search led to the retrieval of 225 articles: 33 in Web of Science, 138 in PubMed, and 54 in Embase. After elimination of duplicate references, the titles and abstracts of the articles were analyzed with respect to the eligibility criteria, and 24 articles were selected for full-text reading. All of the assessed studies were eligible for the qualitative synthesis (Fig. 1).

Study selection flow diagram
Study methodology
The characteristics of the 24 selected studies are described in Table 1 (methodology) and Table 2 (results). Sixteen randomized clinical trials [1, 2, 19,20,21,22,23, 30,31,32,33,34,35,36,37,38] and 8 clinical trials [39,40,41,42,43,44,45,46] were selected. In total, 1197 subjects were exposed to home bleaching using different bleaching agents such as HP at concentrations of 3% [35], 5% [20] 5.3% [20] 6% [21, 22, 34, 43], 7.5% [21, 40], and 10% [1, 21] and CP at concentrations of 10% [1, 2, 19, 22, 23, 30,31,32,33, 36,37,38,39, 42,43,44,45,46], 15% [34, 41, 46], 16% [23, 30, 38], 20% [46], and 28% [37]. A total of 8 studies analyzed the color change combining the use of spectrophotometer and visual color guides (classic vita pan type or similar) [1, 2, 19, 22, 23, 30, 36, 38], while 8 studies used color guides as the only recording method [20, 21, 33, 35, 39, 42, 44, 45]. One study used a spectrophotometer to determine color changes [37], 3 studies combined the use of colorimeter and color guides [40, 41, 46], and 4 studies used only a colorimeter [31, 32, 34, 43]. Some authors used customized splints adapted to the size of the sensor of the spectrophotometer or colorimeter, in order to favor the reproducibility of the measurements [1, 2, 19, 31, 32, 36, 40, 41]. Others simply placed the sensor in the center of the tooth, which is not as precise as the method described above [22, 23, 30, 37, 38, 43, 46].
The study with the lowest number of patients included 20 of them [37] and those with the highest number included 92 [22, 23, 30, 38]. Most of the studies opted for customized bleaching splints with a reservoir as the method of application of the bleaching agent [1, 2, 19,20,21,22,23, 30, 34, 36,37,38, 41,42,43,44, 46]. Six studies applied the agent in customized splints without a reservoir [31,32,33, 35, 39, 40]. Two studies applied the agent using customized splints with and without a reservoir, following a split-mouth design [
Regarding the bleaching agent application protocols, different patterns were observed. Most of the studies chose short exposure times between 30 min and 3 h [1, 19,20,21, 23, 30, 34,35,36,37,38, 40, 41, 43, 45]. The remaining studies opted for long exposure times between 6 and 8 h, maintaining a nocturnal pattern
Study results
Authors who measured color stability using objective techniques after 2 [43] and 3 months [2, 34, 40, 41] reported homogeneous results between groups. Slight recurrences were also described. However, they did not reach statistically significant values (p < 0.04). The studies that performed a 6-month follow-up [19, 22, 30,31,32,33, 35, 44] reported similar results. Authors who measured both ΔE and DSGU did not reach statistical significance ((p = 0.3, p = 0.7) [30] and (p > 0.05) [19]). Authors who only measured ΔE recorded stable values [31, 32]. The variations recorded indicated a slight regression of the color, but they were not statistically significant (p < 0.05). Three studies only performed DSGU measurements, two of them reported no recurrence [33, 35], and the third study [44] reported a setback of 1 DSGU unit and a recurrence of 12%.
Authors who performed follow-ups after 1 year post bleaching, did not report significant differences between the color change from immediate post bleaching and after 1 year. One study highlighted differences between beach guides, which were clinically significant after ΔE calculation [36]. Two studies [23, 38], in the annual and 2 years post-bleaching follow-ups, reported color stability in terms of the ΔE values.
In a study in which smokers were compared to non-smokers 2.5 years post bleaching [45], DSGU measurement showed a slight but statistically significant color recurrence in both groups. Two studies assessed patients with intrinsic discolorations secondary to the intake of tetracyclines [42, 46]. Follow-ups were performed at 5 and 7.5 years. The first study, ΔE results, showed that the result achieved after the treatment had maintained 68%, 67%, and 66% of the applied concentrations of CP (10%, 15%, and 20%, respectively) [46]. The second study, after 90 months, showed that 60% of the subjects reported no visible changes, 7% reported a slight recurrence, and another 7% showed a moderate recurrence [42].
Risk of bias
All studies were rated using the Cochrane Collaboration tools for risk of bias: RoB2 was used for rating RCT and ROBINS-I for CT (Figs. 2 and 3).

Quality assessment of the included RCTs using RoB-2. A Table format. B Graphical format

Quality assessment of the included CTs using ROBINS-I. A Table format. B Graphical format
RCT studies were classified as unclear for the following elements: bias arising from the randomization process [2, 19, 21, 22, 37], bias due to deviations from the intended intervention [2, 19, 22, 23, 30, 32,33,34,35,36,37,38], and bias in outcome measurement [2]. Other studies were classified as high risk for the following elements analyzed: bias arising from the randomization process [32] and bias due to deviations from the intended intervention [1, 21, 31]. The remaining studies were classified as low risk for the following elements: bias arising from the randomization process [1, 20, 23, 30, 31, 33,34,35,36, 38], bias due to deviations from the intended intervention [20], bias due to missing data on outcomes [1, 2, 19,20,21,22,23, 30,31,32,33,34,35,36,37,38], bias in outcome measurement [1, 19,20,21,22,23, 33,34,35,36,37,38,39,40,41], and bias in selection of the reported outcome [1, 2, 19,20,21,22,23, 30,31,32,33,34,35,36,37,38].
CT studies were classified as low risk for the following elements: bias due to confounding [39,40,41,42,43,44,45,46], bias due to the selection of participants [39,40,41,42,43,44,45,46], bias in classification of interventions [39,40,41,42,43,44,45,46], bias due to deviations from intended interventions [39,40,41,42,43,44,45,46], bias due to missing data [40, 41], bias in measurement of outcomes [40, 44], and bias in the selection of the reported result [39,40,41,42,43,44,45,46]. Other studies were classified as unclear for the following elements: bias due to missing data [39, 43,44,45,46] and bias in measurement of outcomes [39, 41,42,43, 45, 46]. Only one study was classified as high risk for the following element: bias due to missing data [42].
Discussion
Concern has been expressed about the duration of the effects of dental bleaching. This has been the subject of several studies over the years [3, 4]. Multiple variables such as effectiveness, intra- and post-treatment sensitivity, and long-term color stability have been analyzed [47]. The great heterogeneity in the designs of the research methodologies, the lack of a single clinical and follow-up protocol (or at least a minimum for conducting studies), and the different techniques applied to obtain the data make it difficult to reach a consensus. Nevertheless, the results obtained in the included studies highlight that the color obtained after home dental bleaching remains stable between 1 and 2.5 years regardless of the bleaching agent used or its forms of administration.
The selected studies compared the performance of at-home bleaching products by applying different experimental protocols with the aim of monitoring their long-term prognosis. The number of participants was different among the studies, ranging from 20 to 92. The remaining articles included an average of 51 participants, and only a few studies performed a sample size calculation [1, 19, 22, 23, 30, 36, 38].
The studies included variables such as the presence or absence of a reservoir in the bleaching splints to determine if its presence influenced the result [41, 42]. Color measurements were performed by objective technique, such as the spectrophotometer [37] or colorimeter [31, 32, 34, 43], or subjective operator dependent techniques, using shade guides sorted according to dental brightness [20, 21, 33, 35, 39, 42, 44, 45]. Other studies used a combination of both techniques [1, 2, 19, 22, 23, 30, 36, 38, 40, 41, 46].
The analysis and comparison of the data obtained from the different studies present some limitations since the authors performed the measurements not only in different ways, but also at different times and with different apparatus. In addition, when the measurements were performed with the same apparatus (spectrophotometer or colorimeter), they were not carried out in the same way. In the case of measurements using subjective techniques, it should be noted that the same shade guides were not used in all the studies. This hinders the comparability between studies.
The clinical and follow-up protocols were diverse. The results obtained in the studies regarding the effectiveness of the method of application of the bleaching agent were similar. Therefore, it can be deduced that the form of application of the treatment does not influence the final result. The extent of treatment over time varied between 1 and 3 weeks. In the case of intrinsic staining treatments secondary to drugs (tetracyclines), the treatment was extended up to 6 months [42, 46]. Follow-up times were also heterogenous, ranging from 2 months to 7.5 years.
Authors who measured color stability using objective techniques after 2 [43] and 3 months [2, 34, 40, 41] and who used HP between 6% [34, 43] and 7.5% [40] and CP between 10% [2, 41, 43], 15% [34, 41], and 20% [40] reported homogeneous results between groups. Slight recurrences were also described. However, they did not reach statistically significant values (p < 0.04). Such results could be attributed to the short follow-up time.
The studies that performed 6-month follow-up and applied CP from 10% [19, 22, 30,31,32,33, 44] to 16% [30] and HP at 3% [35] and 6% [22] and performed the measurements subjectively [33, 35, 44], objectively [31, 32], and by means of a combination of both [19, 22, 30] and reported similar results. Rosentisel et al. [32] and Matis et al. [31] measured color using a colorimeter. Both applied 10% CP overnight but differed in the extent of treatment: 5 days and 3 weeks, respectively. They agree that after the color measurements and subsequent CIELAB analysis calculating ΔE, the color was stable when compared to the post-bleaching values. Also, the variations recorded indicated a slight regression of the color, but they were not statistically significant (p < 0.05).
In the studies by Meireles et al. [30] and Darriba et al. [19], in which color measurements were made using both techniques, despite having applied different bleaching protocols, the authors reported a slight recurrence in both groups studied. However, again, data did not reach statistical significance ((p = 0.3, p = 0.7) [30] (p > 0.05) [19]). Color measurement by means of color guides confirmed the results obtained after calculation of ΔE value. On the other hand, Aka et al. [22] observed a statistically significant (p < 0.05) recurrence (ΔE) in the CP group at 10%, and the measurement of color using guides showed better brightness values in the CP group compared to the HP group.
Alternatively, Russell et al. [33], Mayers et al. [35], and Medeiros et al. [44] performed the measurements only by using shade guides. The first two reported no recurrence, while Medeiros et al. [44] reported a setback of 1 DSGU unit and a recurrence of 12%, without attributing this result to a specific cause. The subjectivity of the technique and the difficult comparability of the values derived from it with the values provided by objective techniques, which are capable of recording what the human eye cannot always record, or at least not with such precision, make it difficult to compare the studies with each other.
Other authors performed follow-ups after 1 year post bleaching. Martini et al. [36] performed color measurements using a spectrophotometer and color guides. They reported no significant differences between the color change from immediate post bleaching and after 1 year using the classic vita pan shade guide unit (mean difference = 0.1 ΔSGU; 95% central incisor, 0.2 to 0.4; p = 0.53; and at 1 year, mean difference = 0.3 95% central incisor 1.0 to 1.6; p = 0. 62). However, significant differences were observed using the VITA Bleachedguide (VITA Zahnfabrik, Bad Säckingen, Germany) (mean difference = 1.4 ΔSGU; 95% central incisor 0.7 to 2.1; p < 0.01). After calculation of ΔE, these differences were defined as not clinically important, since they were below the 50:50 perception threshold for shade changes in dentistry [36].
Another factor that hinders the comparison of the results of studies using subjective techniques is the diversity between guides. This generates a certain degree of uncertainty about the reliability of the results obtained. Authors such as Mailart et al. [1] and Martini et al. [36] performed follow-up at 1 year using a spectrophotometer and two different color guides and concluded that the color remains stable since no statistically significant differences were observed between the groups after ΔE analysis. In addition, no color discrepancies were reported upon comparison with the two guides. Meireles et al. [23, 38] also performed the color measurements using a spectrophotometer and color guide. In the annual and biennial post-bleaching follow-ups, the results were not significantly different in terms of the ΔE values, and the median tooth color did not show statistically significant changes (p > 0.2).
Pinto et al. [21] and Auschill et al. [20] analyzed the shade stability using vita 3DMASTER (VITA Zahnfabrik, Bad Säckingen, Germany) and vita pan classic (VITA Zahnfabrik, Bad Säckingen, Germany) shade guides, respectively. In the study by Pinto et al. [21], all groups showed color stability at 12 months post bleaching. Auschill et al. [20], after 18 months of follow-up, reported recurrence in both groups studied when compared with the results obtained after bleaching, reporting values from 2.88 (p = 0.24) to 3.3 (p = 0.001) DSGU.
The origin of discolorations will be decisive in determining both the effect and the prognosis of bleaching. The study conducted by De Geus et al. [45] selected a different sample from the previously mentioned studies, composed of smokers vs. nonsmokers. The aim of their study was to evaluate the stability of whitening at 2.5 years using measurement techniques using classic vita pan and vita bleach 3dmaster shade guides (VITA Zahnfabrik, Bad Säckingen, Germany). At 30 months, a homogeneous high dropout rate (28%) was reported in both groups: 5 participants stopped smoking and 4 reduced the number of cigarettes consumed daily. In the measurements, a slight but statistically significant color recurrence could be detected in both groups. Therefore, the recurrence is not only attributable to extrinsic staining potentially caused by smoking, although in view of the changes in the smoking group, the comparison is not completely fair. The authors whose samples consisted of patients with intrinsic discolorations secondary to the intake of drugs (tetracyclines) were Matis et al. [46] and Leonard et al. [42], who applied similar clinical protocols: nocturnal application of CP for 6 months, at 10%, 15%, and 20% in the case of Matis et al. [46] and only 10% in the case of Leonard et al. [42]. The color measurement techniques and follow-up times varied between the two studies. In the first study [46], they followed up at 5 years using a colorimeter and Vitalescence Esthetic Ultradent shade guides (Vitalescence Esthetic Restorative Masters Shade Guide, Ultradent Products, Inc.), and in the second study [42], they followed up at 7.5 years measuring shade changes using classic vita pan shade guides. Matis et al. [46] reported ΔE results, which showed that concentrations of 10%, 15%, and 20% had maintained 68%, 67%, and 66% of the color achieved after bleaching, respectively. The results of Leonard et al. [42] also showed recurrences. After 90 months, 60% of the subjects reported no visible changes, 7% reported a slight recurrence, and another 7% showed a moderate recurrence, but never matching the pretreatment color. In addition, 27% of the subjects reported having undergone further bleaching sessions before 90 months. Both studies showed higher levels of recurrence than studies whose samples did not include patients with intrinsic staining, which is evidence of a greater degree of difficulty in maintaining the results in these groups of patients.
The main limitation of the present systematic review is based on the great diversity of clinical and follow-up protocols employed in the included studies. In addition, a wide range of measurement methods were used, which make it difficult to compare the results obtained in the studies. Therefore, there is a need to establish a single experimental protocol to facilitate the interpretation of the data obtained.
Conclusions
Although many studies have demonstrated the general efficacy of bleaching gels, the long-term benefits of the treatment related to color maintenance are not well established in the literature. Most authors state that the color remains stable between 1 and 2.5 years regardless of the type of bleaching agent or the forms of administration such as individualized cuvette with reservoir, individualized cuvette without reservoir, and preformed cuvette provided by the manufacturer. Color stability in cases of severe discolorations such as tetracycline staining presents a higher degree of recurrence.
References
Mailart MC, Sakassegawa PA, Santos KC et al (2021) One-year follow-up comparing at-home bleaching systems outcomes and the impact on patient’s satisfaction: randomized clinical trial. J Esthet Restor Dent 33:1175–1185. https://doi.org/10.1111/jerd.12814
Meireles SS, de Oliveira RDB, Barbosa MTG et al (2022) Efficacy and tooth sensitivity of at-home bleaching in patients with esthetic restorations: a randomized clinical trial. Clin Oral Investig 26:565–573. https://doi.org/10.1007/s00784-021-04035-y
Kwon SR, Wertz PW (2015) Review of the mechanism of tooth whitening. J Esthet Restor Dent 27:240–257. https://doi.org/10.1111/jerd.12152
Alqahtani MQ (2014) Tooth-bleaching procedures and their controversial effects: a literature review. Saudi Dent J 26:33–46. https://doi.org/10.1016/j.sdentj.2014.02.002
Alkahtani R, Stone S, German M, Waterhouse P (2020) A review on dental whitening. J Dent 100:103423. https://doi.org/10.1016/j.jdent.2020.103423
Viscio D, Gaffar A, Fakhry-Smith S, Present (2000) Present and future technologies of tooth whitening. Compend Contin Educ Dent suplement 28:36–43
Nathoo SA (1997) The chemistry and mechanisms of extrinsic and intrinsic discoloration. J Am Dent Assoc 128:6S-10S. https://doi.org/10.14219/jada.archive.1997.0428
Dodson D, Bowles W (1991) Production of minocyclines pigment by tissue extracts. J Dent Res 70:424
Dwinelle WH, Harris CA, Cleveland JA et al (1848) Ninth annual meeting of the American society. Am J Dent: 143–147
Kirk E (1889) The chemical bleaching of teeth. Dent Cosm 31:273–283
Haywood VB (1992) History, safety, and effectiveness of current bleaching techniques and applications of the nightguard vital bleaching technique. Quintessence Int 23:471–488
Kingsbury C (1861) Discoloration of dentine. Dent Cosm 3:57–60
Franchi GJ (1950) A practical technique for bleaching discolored crowns of young permanent incisors. J Dent Child 20:68–69
E bogue, (1872) Bleaching teeth. Dent Cosm 1872:141–143
Harlan A (1891) The dental pulp, its destruction, and methods of treatment of teeth discolored by its retention in the pulp chamber or canals. Dent Cosm 33:137–141
Atkinson C (1892) Fancies and some facts. Dent Cosm 34:968–972
Kihn PW (2007) Vital tooth whitening. Dent Clin North Am 51:319–331. https://doi.org/10.1016/j.cden.2006.12.001
Powell LV, Bales DJ (1991) Tooth bleaching: its effect on oral tissues. J Am Dent Assoc 122:50–54. https://doi.org/10.14219/jada.archive.1991.0310
Darriba IL, Cabirta Melón P, GarcíaSartal A et al (2019) Influence of treatment duration on the efficacy of at-home bleaching with daytime application: a randomized clinical trial. Clin Oral Investig 23:3229–3237. https://doi.org/10.1007/s00784-018-2744-z
Auschill TM, Schneider-Del Savio T, Hellwig E, Arweiler NB (2012) Randomized clinical trial of the efficacy, tolerability, and long-term color stability of two bleaching techniques: 18-month follow-up. Quintessence Int 43:683–694
Pinto MM, Gonçalves MLL, da Mota ACC et al (2017) Controlled clinical trial addressing teeth whitening with hydrogen peroxide in adolescents: a 12-month follow-up. Clinics 72:161–170. https://doi.org/10.6061/clinics/2017(03)06
Aka B, Celik EU (2017) Evaluation of the efficacy and color stability of two different at-home bleaching systems on teeth of different shades: a randomized controlled clinical trial. J Esthet Restor Dent 29:325–338. https://doi.org/10.1111/jerd.12296
Meireles SS, Santos IS, Della BA, Demarco FF (2010) A double-blind randomized clinical trial of two carbamide peroxide tooth bleaching agents: 2-year follow-up. J Dent 38:956–963. https://doi.org/10.1016/j.jdent.2010.08.003
Setien VJ, Roshan S, Nelson PW (2008) Clinical management of discolored teeth. Gen Dent 56:294–304
Zantner C, Beheim-Schwarzbach N, Neumann K, Kielbassa AM (2007) Surface microhardness of enamel after different home bleaching procedures. Dent Mater 23:243–250. https://doi.org/10.1016/j.dental.2006.06.044
De Geus JL, Wambier LM, Kossatz S et al (2016) At-home vs in-office bleaching: a systematic review and meta-analysis. Oper Dent 41:341–356. https://doi.org/10.2341/15-287-LIT
Luque-Martinez I, Reis A, Schroeder M et al (2016) Comparison of efficacy of tray-delivered carbamide and hydrogen peroxide for at-home bleaching: a systematic review and meta-analysis. Clin Oral Investig 20:1419–1433. https://doi.org/10.1007/s00784-016-1863-7
Yepes-Nuñez JJ, Urrútia G, Romero-García M, Alonso-Fernández S (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Rev Esp Cardiol 74:790–799. https://doi.org/10.1016/j.recesp.2021.06.016
Sterne JAC, Savović J, Page MJ et al (2019) RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 366:. https://doi.org/10.1136/bmj.l4898
Meireles SS, Heckmann SS, Santos IS et al (2008) A double blind randomized clinical trial of at-home tooth bleaching using two carbamide peroxide concentrations: 6-month follow-up. J Dent 36:878–884. https://doi.org/10.1016/j.jdent.2008.07.002
Matis B, Cochran M, Eckert G (1998) the efficacy and safety of a 10% carbamide peroxide bleachinng gel. J Esthet Restor Dent 29:555–563
Rosenstiel SF, Gegauff AG, Johnston WM (1996) Randomized clinical trial of the efficacy and safety of a home bleaching procedure. Quintessence Int 27:413–424
Russell CM, Dickinson GL, Johnson MH et al (1996) Dentist-supervised home bleaching with ten percent carbamide peroxide gel: a six-month study. J Esthet Restor Dent 8:177–182. https://doi.org/10.1111/j.1708-8240.1996.tb00422.x
Botelho MG, Chan AWK, Newsome PRH et al (2017) A randomized controlled trial of home bleaching of tetracycline-stained teeth. J Dent 67:29–35. https://doi.org/10.1016/j.jdent.2017.05.003
Myers ML (2003) Clinical evaluation of a 3% hydrogen peroxide tooth-whitening gel. J Esthet Restor Dent: 50–56. https://doi.org/10.1007/978-3-319-33355-7_21
Martini EC, Favoreto MW, de Andrade HF et al (2021) One-year follow-up evaluation of reservoirs in bleaching trays for at-home bleaching. J Esthet Restor Dent 33:992–998. https://doi.org/10.1111/jerd.12797
Türkün M, Çelik EU, Aladǎ A, GÖkay N (2010) One-year clinical evaluation of the efficacy of a new daytime at-home bleaching technique. J Esthet Restor Dent 22:139–146. https://doi.org/10.1111/j.1708-8240.2010.00325.x
Meireles SS, Da Silva Dos Santos I, Delia Bona Á, Demarco FF (2009) A double-blind randomized controlled clinical trial of 10 percent versus 16 percent carbamide peroxide tooth-bleaching agents. J Am Dent Assoc 140:1109–1117. https://doi.org/10.14219/jada.archive.2009.0337
Swift EJ Jr, May KN Jr, Wilder AD Jr, Heymann HO, Bayne SC (1999) Two-year clinical evaluation of tooth whitening using an at-home bleaching system. J Esthet Restor Dent: 11:36–42
Mokhlis GR, Matis BA, Cochran MA, Eckert GJ (2000) A clinical evaluation of carbamide peroxide and hydrogen peroxide whitening agents during daytime use. J Am Dent Assoc 131:1269–1277. https://doi.org/10.14219/jada.archive.2000.0380
Matis BA, Hamdan YS, Cochran MA, Eckert GJ (2002) A clinical evaluation of a bleaching agent used with and without reservoirs. Oper Dent 27:5–11
Leonard RH Jr, Van Haywood B, Caplan DJ, Tart ND (2003) Nightguard vital bleaching of tetracycline-stained teeth: 90 months post treatment. J Esthet Restor Dent 15:142–52; discussion 153
Hannig C, Lindner D, Attin T (2007) Efficacy and tolerability of two home bleaching systems having different peroxide delivery. Clin Oral Investig 11:321–329. https://doi.org/10.1007/s00784-007-0128-x
Medeiros MCDS, De Lima KC (2008) Effectiveness of nightguard vital bleaching with 10% carbamide peroxide - A clinical study. J Can Dent Assoc (Tor) 74:163–163e
De Geus JL, Fernández E, Kossatz S et al (2017) Effects of at-home bleaching in smokers: 30-month follow-up. Oper Dent 42:572–580. https://doi.org/10.2341/16-126-C
Matis BA, Wang Y, Eckert GJ et al (2006) Extended bleaching of tetracycline-stained teeth: a 5-year study. Oper Dent 31:643–651. https://doi.org/10.2341/06-6
Fiorillo L, Laino L, De Stefano R et al (2019) Dental whitening gels: strengths and weaknesses of an increasingly used method. Gels 5:. https://doi.org/10.3390/gels5030035
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature.
Author information
Authors and Affiliations
Contributions
M.M. contributed to investigation, conceptualization, methodology, writing-original draft, writing —review and editing.
L.F. contributed to formal analysis, conceptualization writing — review and editing.
J.L.S. contributed to translation, review and editing of the manuscript.
R.F. contributed to investigation, conceptualization, methodology, writing-original draft, writing — review and editing. All authors contributed to preparation and approval of the final version of the manuscript.
Corresponding author
Ethics declarations
Ethical approval
Not applicable.
Informed consent
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fioresta, R., Melo, M., Forner, L. et al. Prognosis in home dental bleaching: a systematic review. Clin Oral Invest 27, 3347–3361 (2023). https://doi.org/10.1007/s00784-023-05069-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-023-05069-0