
Abstract
Purpose
There is an increased demand for surgical solutions to treat craniocervical instability. This retrospective study demonstrates the clinical and radiological outcomes of unstable craniocervical junction treated with occipitocervical fusion.
Material and methods
The mean age of 52 females and 48 males was 56.89 years. The clinical and radiological outcomes were assessed, including NDI, VAS, ASIA score, imaging, complications and bony fusion in two used constructs: a modern occipital plate–rod–screw system (n = 59) and previous bilateral contoured titanium reconstruction plates–screws (n = 41).
Results
Clinically and on imaging, patients presented with neck pain, myelopathy, radiculopathy, vascular symptoms and craniocervical instability. The mean follow-up was 6.47 years. A solid bony fusion was achieved in 93.81% of the patients. The NDI and the VAS improved significantly from 28.3 and 7.67 at the presentation to 16.2 and 3.47 at the final follow-up. The anterior and posterior atlantodental interval (AADI and PADI), the clivus canal angle (CCA), the occipitoaxial angle (OC2A) and the posterior occipitocervical angle (POCA) improved significantly. Six patients required early revision.
Conclusion
Occipitocervical fusion can yield excellent results regarding clinical improvement and long-term stability with a high fusion rate. Simple reconstruction plates, though more demanding surgically, achieve similar results. Preserving a neutral patient’s position for fixation avoids postoperative dysphagia and may help prevent adjacent segment disease development.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The craniocervical junction (CCJ) is a sophisticated biomechanical area that links the skull to the cervical spine. Instability at the CCJ can cause compression of the spinal cord and medulla oblongata resulting in myelopathy and progressive disability [1, 2]. Occipitocervical fusion (OCF) combined with reconstruction of the anatomical relationship aims to stabilize a mechanically compromised CCJ, correct displacement and improve the available space for neural structures [2, 3]. OCF significantly reduces head movements that cause discomfort and can be associated with complications most commonly implant-related and wound complications. Therefore, a thorough preoperative evaluation and workup are necessary to select the proper management of this condition [4]. This study aimed to assess the long-term clinical and radiological outcomes after surgical treatment of unstable CCJ with OCF from 1995 to 2019 and a comparison of 2 different constructs: bilateral contoured titanium reconstruction plates with screws (Reco-S) from 1995 to 2007 and later on occipital plate with contoured rods and screws (Occ-R-S).
Material and methods
A retrospective review of the prospectively collected database of patients undergoing OCF was performed. These patients presented with intractable neck pain or progressive neurological insult and instability as underlying pathology, verified by imaging including plain X-rays, CT and MRI.
Indications for surgery
Depending on the clinical, laboratory and imaging investigations, the patients were subclassified into the following groups: inflammatory, traumatic, degenerative, congenital, infection, neoplastic and revision surgery. Patients where C1–C2 fusions were sufficient or who did not complete a minimum postoperative follow-up of 2 years were excluded. The search in the surgical database revealed a total of 100 individuals fulfilling these criteria. In these patients, posterior occipitocervical fixation and fusion with or without transoral release or odontoidectomy were performed between the occiput and the C2 vertebra or subaxial spine according to accompanying subaxial stenosis or instability. Instrumentation using either a median occipital plate with contoured rods and polyaxial screws (Occ-S-R) or in early cases, before the advent of the occipital plates, by bilateral contoured reconstruction plates (Reco-S) was used and fixed to the lateral masses by Magerl’s technique and to the paramedian occiput.
Ethical approval was obtained from our Institutional Review Board (IRB) before the conduct of the study.
Surgical planning
Whereas the posterior approach offers the best option for fixation, it remains insufficient regarding the mobilization of rigid dislocations or stenosis from the anterior. In these cases, an additional anterior or high anterolateral approach can get necessary. Usually, the sequence to be planned is anteroposterior, but in dislocations fused in deformity, a back–front–back strategy was used. To gain optimal access to the joints on either side and the predental space, in this study, the transoral route was preferred.
Surgical technique
After fiber optic oral endotracheal intubation, surgery was done in prone position with the face lying on special foamed pads and the arms tucked by the patient’s side. A midline posterior approach from external occipital protuberance to the desired level of caudal extension with the subperiosteal dissection of paravertebral muscles was performed. A median occipital plate or 2 contoured titanium reconstruction plates (AO 3.5 plates) were applied to the occiput and fixed with bicortical screws. The upper cervical vertebrae were connected using the described techniques [3, 5] via transarticular C2/C1 or pedicle/pars screws placed at C2 and to the lateral mass subaxially in the appropriate levels. Two C arms were used perpendicularly for assessment of reduction and fixation. A high-speed drill was utilized to decorticate the posterolateral spinal elements and to expose cancellous bone at all desired arthrodesis levels. Preparation of fusion was completed by countered iliac bone graft between occiput and spinous process of C2, fixed by non-absorbable sutures. A local closed system negative suction drain was inserted for 48 h.
An anterior transoral approach was used to address ventral pathology when needed as described in Shousha et al. [6]. A detailed postoperative guideline for the transoral approach was followed including the use of a postoperative gastric tube, the use of antibiotics and regular wound care. Postoperatively, a cervical collar was applied for a period of 6–12 weeks and at least 12 weeks in cases treated with Reco-S constructs.
Outcome assessment
The pre-, intra- and postoperative data were collected. All radiological studies were taken, stored and measured in digital form. The intraoperative profile assessment included: patient classification according to the American Society of Anaesthesiologists (ASA) grading system, operative time, blood loss and intraoperative complications. In the postoperative phase, the presence and degree of dysphagia were assessed and documented.
The clinical and radiographic follow-up was 77.64 ± 26.52 ranging from (24–291) months, with a minimum of 24 months. The neck disability index (NDI) and the visual analogue scale (VAS) were recorded as clinical outcome parameters. The questionnaire was completed immediately before surgery, during the first visit after the surgery and at the final follow-up. The neurological status was assessed by American Spinal Injury Association (ASIA) score pre- as well as postoperatively and at the final follow-up. Plain cervical spine radiographs were obtained on the first postoperative day and the last day before discharge under loading (either in a standing or sitting position) followed by regular evaluation over the follow-up period.
The following radiological parameters (Fig. 1) were measured pre- and postoperatively:
-
Anterior atlantodental interval (AADI): from the posterior aspect of C1 to the anterior aspect of dens.
-
Posterior atlantodental interval (PADI): from the posterior surface of dens to the anterior surface of the posterior arch of C1 that reflects the space available for the cord (SAC).
-
Clivus canal angle (CCA): angle formed at the posterior border of clivus and posterior vertebral C2 line.
-
Occipitoaxial angle (OC2A): measured by the angle between McGregor’s line and a line along the inferior end plate of C2 (where McGregor’s line is drawn from the tip of the posterior margin of the hard palate to the undermost surface of the occiput) [7].
-
Posterior occipitocervical angle (POCA) is defined as the angle formed by the intersection of a line drawn tangential to the flat posterior aspect of the occiput between the foramen magnum and occipital protuberance and the line determined by the posterior aspect of the third and fourth cervical facets [8].

Different measurements obtained (A anterior atlantodental interval—AADI, B posterior atlantodental interval—PADI, C occipitoaxial angle—OC2A, D clivus canal angle—CCA, E posterior occipitocervical angle—POCA)
Radiographic fusion
Fusion was determined according to lateral cervical spine X-rays. It was confirmed by the presence of solid body mass between the occiput and the spinous process of C2 vertebra without lucencies or failure of the construct (loosening or fracture of plates or screws).
When computed tomography (CT) was available, fusion was defined as the presence of bony trabeculae across the graft–host interface. Any reoperation during the follow-up period was reported and analyzed regarding cause, clinical presentation, radiological assessment and surgical intervention.
Statistical analysis
Analysis of those collected data using the SPSS program was performed on an IBM compatible computer. Demographic data and frequencies were calculated using mean and standard deviation. Clinical and radiological parameters were analyzed using paired t-test. The results of both groups Reco-S and Occ-S-R were compared, and statistical significance was established at a P value of less than 0.05.
Results
Perioperative data
Among the 100 patients, 52 were females and 48 were males. The mean age at surgery was 56.89 ± 19.18 years. The main complaint was neck pain in 86%, followed by myelopathy in 11%, radiculopathy in 10%, neurological defect in 9%, vertigo in 4%, torticollis in 3% and dysphagia in 2% of the patients. Usually, multiple complaints were combined. The causes for surgery were inflammatory (35), traumatic (21), degenerative (16), congenital (12), revision surgery (10), infection (3) and neoplasm (3).
Most patients were graded in ASA III (63), in ASA II (32) and in ASA I (5) according to the system of the American Society of Anaesthesiologists (ASA). The mean operative time (including graft removal and transoral procedures) was 210.3 ± 69.58 min, and the mean amount of blood loss was 570 ± 251.06 ml. Posterior-only approach was used in 73 while the remaining 27 needed combined anterior transoral plus posterior surgery (Fig. 2). In 59 patients, Occ-R-S was used, and in 41, Reco-S was used (Fig. 3).

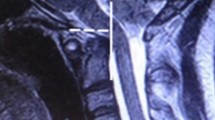
A 33-year-old male presented with atlantooccipital assimilation and basilar invagination was treated with anterior transoral partial odontoidectomy and posterior OCF (A pre-X-ray, B pre-CT, C pre-MRI, D postoperative anteroposterior X-ray, E postoperative lateral X-ray, F: postoperative MRI, G follow-up after 4 years)

A 45-year-old female patient presented with posttraumatic degenerative arthritis: A pre-X-ray, B pre-CT, C postoperative anteroposterior X-ray, D postoperative lateral X-ray, E 1 year postoperative F 18 years postoperative
Lower instrumented vertebrae were C2 in 48 patients, subaxial (C3 toC7) in 41 and 11 fixations spanned to the thoracic spine. C2 fixation was achieved in 4 different methods: transarticular C1-C2 screws (145 screws were inserted), pars (31 screws), pedicle (4 screws) and lamina (1 screw). In 11 patients with fixation to a lower level, C2 was skipped in 3 cases on one side and in 8 cases on both sides.
Clinical outcome
The neurological status improved from the time of presentation to the final follow-up with no permanent neurological worsening. The mean VAS for neck pain improved significantly from 7.67 ± 1.45 preoperatively to 3.47 ± 2.31 at the final follow-up (P0.01 and t = − 19.39) and the mean value for the NDI improved significantly from 28.38 ± 7.75 at presentation to 16.24 ± 9.56 at the final follow-up (P0.01 and t = − 27.19). A transient mild postoperative dysphagia was recorded in three patients, all improved before discharge (Table 1).
Radiological outcome
All radiological outcomes showed improvement. AADI improved from a mean of 4.91 ± 2.68 to 2.84 ± 0.89 mm, PADI from 11.35 ± 3.96 to 15.62 ± 2.4 mm and CCA from 147.68 ± 14.63 to 156.58 ± 10.88°. OC2A was increased from a mean of 28.84 to 33.09°, and all previous measurements were statistically significant. POCA changed from a mean of 104.37 ± 13.75 to 103.73 ± 12.47° remaining statistically insignificant (Table 2).
Complications
Among 43 patients presenting with complications 3 occurred during surgery and 40 postoperatively. Intraoperative complications were 2 incidental durotomies and 1 fracture of the posterior arch of C1 during decortication for the grafting. In the early postoperative phase, six patients required reoperation. The first presented with postoperative vertebral artery thrombosis, cerebellar edema and ataxic gait followed by symptoms of increased intracranial pressure. MRI showed right cerebellar infarction and vertebral artery origin stenosis. On revision, no cause could be found in the operative field, and six weeks postoperatively, the patient had a complete clinical recovery. The second presented with pharyngeal wound dehiscence and developed a left cerebellar abscess. He recovered fully after evacuation and revision of the transoral wound. The third presented with postoperative infection of the posterior wound and pressure necrosis with loosening of the construct. Removal of the reconstruction plates and refixation using transarticular screws was done. After 4 months, this patient was exposed to trauma and again pullout of screws occurred. He finally fused after reoperation with reconstruction plates and lateral mass fixation. Rapidly increasing subaxial stenosis in the fourth patient required additional anterior surgery. The fifth presented with a type II odontoid fracture after a previous subaxial fusion and developed postoperative loosening of occipital screws occurred requiring revision. The last patient presented with canal stenosis due to diffuse idiopathic skeletal hyperostosis (DISH). Postoperative displacement of the left rod requiried repositioning and posterior decompression of C 5–6. So implant-related and wound problems were the most common postoperative complications (Table 3).
Fusion
Fusion was detected in 93.81% (91/97) of patients while the remaining 3 patients were temporarily fixed without the aim of fusion.
An analysis of the pre-, intra- and postoperative data of patients treated either using Reco-S or Occ-S-R was performed. Comparison revealed no statistically significant difference between these constructs (Table 4).
Discussion
The CCJ functions a transition zone between the occiput and subaxial spine [1]. Various pathologies may occur in this area resulting in a variety of symptoms ranging from asymptomatic, accidentally discovered problems to severe myelopathy and brain stem compression that may endanger patients’ life [2]. Different causes may result in CCJ instability and objectives for OCF are stabilization, decompression, restoration of sagittal and coronal alignment and lastly arthrodesis through decortication of bone and grafting [2, 3, 9]. Due to the nature and location of this surgery, adverse events such as neurological impairment, vascular injury, infection, instrumentation failure, pseudoarthrosis, persisting instability and pain can occur. Numerous surgical methods for occipitocervical fusion have evolved with improved alignment, a higher rate of successful arthrodesis and less complications [9,10,11]. As in systematic review by Winegar et al. [9], most publications deal with a single pathology or few patients. In this study, we aimed to assess the neurological and radiological outcomes of a large number of patients with different pathologies. We compared the results achievable by two fixation methods Reco-S and Occ-R-S with long follow-up.
This series comprised 100 patients with almost equal sex distribution and an average age of 56.89 ± 19.18. Symptoms as well as diagnoses and indications for surgery were comparable with other series in the literature [9, 12,13,14,15].
Surgical techniques
While all patients were operated via a posterior approach, in 27 an anterior transoral procedure was combined. This is similar to Bhatia et al. [15] who treated 100 patients: 81 through posterior and 19 combined anteroposterior. In many other studies, patients were approached from posterior only [12,13,14].
In 59 patients an Occ-S-R was used, whereas 41 CCJs were fixed using Reco-S. Occ-S-R implants typically allow easier handling and a greater degree of intraoperative correction. Reco-S can be contoured to adapt the CCJ morphology but have significant limitations regarding placement and angle stability of screws. Different rigid instrumentation was used in other studies: Nockels et al. [12] employed 2 contoured plates in 68% and occipital plate with contoured rods plus screws in 32% of his patients, whereas others [14, 15] used only Occ-R-S. The occipitocervical geometry represents a major obstacle to implant fixation in C1. With a contoured bilateral plate, it is virtually impossible and even the present-day occipital plate constructs rarely allow space for fixation of C1 in addition to C2 / the occiput.
In these studies [9, 12], the authors did not find a clinically or radiologically significant difference regarding the improvement and healing depending on the implants used. This finding could be confirmed in the present study with no significant differences using either Occ-R-S or Reco-S as both constructs were used in an equal set of pathologies in both cohorts.
The median number of levels instrumented was three from occiput to C3 (O-C3) ranging from 2 levels (O-C2) to 13 levels (O-T6). This was mainly attributable to these patients’ pathology and condition of their subaxial spine. Other studies showed comparable results: In Nockels et al. [12], the mean number of levels instrumented was 3.7 (range 2–10), and in Martinez-Del-Campo et al. [13], the median number of levels was 5 (O-C4) ranging from 1 level (O-C1) to 13 levels (O-T6). Upadhyaya et al. [14] reported that the levels ranged from C2 to C6, mostly ending at C2, and in Bhatia et al. [15], the lower instrumented levels ranged between C 3 and T 3. Pan et al. [16] compared one group with short-segment fixation (SSF) to C2 with another group fixed to C3 and found no statistical difference between the two groups in terms of fusion. He concluded that SSF should be preferred when no subaxial instability was involved and patients with severe osteoporosis or other diseases affecting the stability of instrumentation should receive individualized treatment.
In biomechanical study, Finn et al. [17] proved that the best option for fixation is C1-C2 transarticular fixation followed by C1 lateral mass plus C2 pedicle or pars screws. This mirrors our experience and it is reflected in utilization of transarticular screws in 145 of 200 fixations.
Sawin et al. [18] reported that autologous grafts harvested from the iliac crest have been widely used for cervical arthrodesis. Similarly, in this study an iliac bone graft was used in all except three cases of temporary fixation. Other grafting options were also described in the literature like ribs, fibular grafts, morselized allografts and locally collected bone [9, 12,13,14,15]. Fusion rates and time to fusion in different studies are summarized in Table 5.
Clinical outcomes
In the present study, there was no postoperative permanent neurological worsening. In patients presenting with a preoperative neurological deficit, an improvement in the postoperative follow-up by one grade in the ASIA score could be documented, which is comparable with other studies [9, 12, 13].
The VAS also improved from 7.67 ± 1.45 preoperatively to 3.47 ± 2.31 at the final follow-up. This is comparable to results obtained by Upadhyaya et al. [14] in which VAS improved from 6.65 ± 1.1 to 2.42 ± 0.49 at the last follow-up. The NDI improvement of the present study was comparable to that of Bhatia et al. [15] who found significant improvement in both rheumatoid and trauma patients while the tumor cases showed minor and insignificant improvement.
Radiological outcomes
AADI in this study improved from a mean of 4.91 ± 2.68 to 2.84 ± 0.89 mm, which is in the normal range of 3 mm. Upadhyaya et al. [14] showed improvement in AADI from a mean of 4.2 ± 1.7 mm to 2.5 ± 1.9 mm. PADI that represents SAC and normally accounts for > 14 mm showed improvement from 11.35 ± 3.96 to 15.62 ± 2.4 mm. Improvement of the neurological deficit is related to the proper decompression of the space available for the cord and this explains the improvement in our study. Also, the CCA was improved from 147.68 ± 14.63 to 156.58 ± 10.88°, the CCA in normal adult and neutral position measuring 145–160° [19].
Different studies showed a significant correlation between OC2 angle and the development of postoperative dyspnea and dysphagia. It was concluded that this angle should be kept at least at more than the preoperative OC2A in the neutral position [20,21,22]. A decrease in OC2A > 5° than preoperative should be avoided since it may result in dysphagia [21, 22]. In our study, the OC2A was increased from a mean of 24.34 ± 8.72 preoperative to 29.73 ± 7.9°. No case of dysphagia persisted postoperatively. Upadhyaya et al. [14] reported an increase from 15.81 ± 1.88 to 21.67 ± 1.08° in the postoperative OC2A.
The POCA in patients with uneventful course measured 103.26° in average. A subgroup that later on needed revision for adjacent segment disease had a distinctly higher POCA value of 110° after primary surgery. It is interesting to note that after the revision the mean angle was decreased to 104.24°. This suggests a positive correlation between increased POCA and the occurrence of adjacent segment degeneration. Maulucci et al. [23] concluded that an elevated POCA may result in the need for reoperation due to increased biomechanical stress upon adjacent segments. Our explanation for this failure is: In order to maintain forward gaze, the CCJ and the construct itself need to be held in maximum extension, thus inducing rapid adjacent segment degeneration. In his series, the patients requiring revision showed a mean of 109.5°. In the series of Upadhyaya et al. [14], POCA was changed from a preoperative mean of 118.67 ± 12.29 to 107.15 ± 12.05° postoperatively. In consequence, it seems important to avoid a postoperative increase of the POCA and by that adjacent segment disease or construct failure.
Follow-up and fusion
Fusion was achieved in 93.81% (91/97) of patients, comparable with fusion obtained in other studies ranging from 88 to 97% [9, 12,13,14,15]. Symptomatic non-fusions were revised surgically according to the individual pathology. In most cases, a revision of the implant with bone grafting resulted in a fusion and improvement of the symptoms (Table 5).
Sawin et al. [18] reported an overall rate of bony fusion using iliac crest graft of approximately 91%. In our study, always autografts were harvested from the iliac crest with a fusion rate of 93.81% (91 of the 97fusion patients).
The mean time to fusion was 13.38 months, which is similar to the mean of 11.039 months obtained by Upadhyaya et al. [14]. Winegar et al. [9] reported fusion occurring in cases ≥ 4 months. Martinez-Del-Campo et al. [13] found fusion taking place in 89.2% of patients during the first year of follow-up. The longer time established for fusion in our work may be due to our method of fusion assessment. We strictly depend on documentation of solid bony mass in lateral X-rays. The detailed manner of how fusion was diagnosed in the other studies remains unclear [9, 12,13,14,15].
Complications
We experienced complications in 43 patients comparing to a range between 10 and 40% in the other reported series [9, 10, 12, 13]. Zileli [4] with 52% found a higher rate. A parallel finding to Zileli [4] is the predominance of implant-related and wound problems. In our series these were fifteen cases followed by 13 wound complications. Table 3 compares complications observed in the two constructs: Reco-S and Occ-R-S. Most of the complications, especially wound problems occurred in patients with ASA III, so it is important to control the patient’s general condition that to help preventing complications.
Fu et al. [24] described a high correlation between the ASA score of patients undergoing spinal surgery and their postoperative morbidity and mortality. In our study, nine patients needed serial dressing and in some cases. Four patients needed wound revision. Implant removal which is not a standard procedure after OCF was done in eleven cases: six patients due to pain and five due to infection. In all these cases, after instrumentation removal they had significantly less pain (low VAS) and improved NDI.
Adjacent segment degeneration occurred in 7 patients after a mean of 5 years (Fig. 4). It is unclear what role primary etiology played in susceptible patients and what effect increased stress over lower instrumented vertebrae exerted. To our knowledge, this is the first study mentioning a time course between OCF and occurrence of ASD. This may be due to relatively short follow-up in other studies [9, 12,13,14,15].

A 81-year-old femal patient presented with degenerative atlantoaxial arthritis, A pre-X-ray, B pre-sagittal CT, C preaxial CT, D postoperative, E 1 year postoperative, F flexion film 1.5 years postoperative, G extension film and both showing adjacent segment disease, H after revision and extension of fixation to C4
Since the long-term results of both methods are comparable, why should an expensive implant be preferred? There are two reasons: The handling is much easier and the construct stability higher. The adaptation of bilateral reconstruction plates which by their arrangement of screw holes dictate the location of anchor points at the craniocervical junction can be quite demanding. In particular, when a corrected position of the head has to be achieved and maintained. Above that, for geometrical reasons, the 2 reconstruction plates of this method cannot be placed in the median area, where the skull provides best and safest purchase. Since the plate–screw connection is not angle stable, longer postoperative external fixation is necessary.
These difficulties might be secondary for colleagues who have to treat patients in low-income countries where the recent construct is not available, difficult to obtain and/or unaffordable for the patient. Thus, the long-term results of this study suggest a continuous role for the old method since the main treatment goal for craniocervical instabilities can be reached similarly to the present state-of-the-art method.
Conclusion
Occipitocervical fusion can yield excellent results regarding clinical improvement and long-term stability with a high fusion rate. Simple reconstruction plates, though more demanding surgically, achieve similar results. Preserving a neutral patient’s position for fixation avoids postoperative dysphagia and may help prevent adjacent segment disease development.
References
Lopez AJ, Scheer JK, Leibl KE, Smith ZA, Dlouhy BJ, Dahdaleh NS (2015) Anatomy and biomechanics of the craniovertebral junction. Neurosurg Focus 38(4):E2. https://doi.org/10.3171/2015.1.FOCUS14807
Lee DJ, Ahmadpour A, Ament JD, Goodarzi A, Panchal RR (2016) when is occipitocervical fusion necessary for upper cervical injuries? Semin Spine Surg. https://doi.org/10.1053/j.semss
Joaquim AF, Osorio JA, Riew KD (2020) Occipitocervical fixation: general considerations and surgical technique. Glob Spine J 10(5):647–656. https://doi.org/10.1177/2192568219877878
Zileli M, Akıntürk N (2022) Complications of occipitocervical fixation: retrospective review of 128 patients with 5-year mean follow-up. Eur Spine J 31:311–326. https://doi.org/10.1007/s00586-021-07037-2
Ebraheim NA, Klausner T, Xu R, Yeasting RA (1998) Safe lateral-mass screw lengths in the Roy-Camille and Magerl techniques. An anatomic study. Spine (Phila Pa 1976) 23:1739–1742
Shousha M, Mosafer A, Boehm H (2014) Infection rate after transoral approach for the upper cervical spine. Spine (Phila Pa 1976) 39(19):1578–1583. https://doi.org/10.1097/BRS.0000000000000475
Chamnan R, Chantarasirirat K, Paholpak P et al (2020) Occipitocervical measurements: correlation and consistency between multi-positional magnetic resonance imaging and dynamic radiographs. Eur Spine J 29:2795–2803. https://doi.org/10.1007/s00586-020-06415-6
Riel RU, Lee MC, Kirkpatrick JS (2010) Measurement of a posterior occipitocervical fusion angle. J Spinal Disord Tech 23(1):27–29. https://doi.org/10.1097/bsd.0b013e318198164b
Winegar CD, Lawrence JP, Friel BC et al (2010) A systematic review of occipital cervical fusion: techniques and outcomes. J Neurosurg Spine 13(1):5–16. https://doi.org/10.3171/2010.3
Ashafai NS, Visocchi M, Wąsik N (2019) Occipitocervical fusion: an updated review. Acta Neurochir Suppl 125:247–252. https://doi.org/10.1007/978-3-319-62515-7_35
Vender JR, Rekito AJ, Harrison SJ, McDonnell DE (2004) The evolution of posterior cervical and occipitocervical fusion and instrumentation. Neurosurg Focus 16(1):E9
Nockels RP, Shaffrey CI, Kanter AS, Azeem S, York JE (2007) Occipitocervical fusion with rigid internal fixation: long-term follow-up data in 69 patients. J Neurosurg Spine 7(2):117–123. https://doi.org/10.3171/SPI-07/08/117
Martinez-Del-Campo E, Turner JD, Kalb S et al (2016) Occipitocervical fixation: a single surgeon’s experience with 120 patients. Neurosurgery 79(4):549–560. https://doi.org/10.1227/NEU.0000000000001340
Upadhyaya M, Jain S, Kire N, Merchant Z, Kundnani V, Patel A (2019) Surgical, clinical, and radiological outcomes of occipitocervical fusion using the plate–screw–rod system with allograft in craniocervical instability. J Craniovert Jun Spine 10:216–223
Bhatia R, Desouza RM, Bull J, Casey ATH (2013) Rigid occipitocervical fixation: indications, outcomes, and complications in the modern era. J Neurosurg Spine 18(4):333–339. https://doi.org/10.3171/2013.1.spine12645
Pan J, Huang D, Hao D et al (2014) Occipitocervical fusion: Fix to C2 or C3? Clin Neurol Neurosurg 127:134–139. https://doi.org/10.1016/j.clineuro.2014.10.013
Finn MA, Fassett DR, McCall TD, Clark R, Dailey AT, Brodke DS (2008) The cervical end of an occipitocervical fusion: a biomechanical evaluation of 3 constructs. Lab Investig J Neurosurg Spine 9(3):296–300
Sawin PD, Traynelis VC, Menezes AH (1998) A comparative analysis of fusion rates and donor-site morbidity for autogeneic rib and iliac crest bone grafts in posterior cervical fusions. J Neurosurg 88:255–265
Henderson FC Sr, Henderson FC Jr, Wilson WA IV, Mark AS, Koby M (2017) Utility of the clivo-axial angle in assessing brainstem deformity: pilot study and literature review. Neurosurg Review 41(1):149–163. https://doi.org/10.1007/s10143-017-0830-3
Izeki M, Neo M, Takemoto M et al (2014) The O-C2 angle established at occipito-cervical fusion dictates the patient’s destiny in terms of postoperative dyspnea and/or dysphagia. Eur Spine J 23:328–336. https://doi.org/10.1007/s00586-013-2963-6
Wang L-N, Bo-wen Hu, Song Y-M et al (2019) Predictive abilities of O-C2a and O-EAa for the development of postoperative dysphagia in patients undergoing occipitocervical fusion. Spine J. https://doi.org/10.1016/j.spinee.2019.11.013
Meng Y, Tingkui Wu, Liu Z et al (2018) the impact of the difference in O-C2 angle in the development of dysphagia after occipitocervical fusion: a simulation study in normal volunteers combined with a case-control study. Spine J. https://doi.org/10.1016/j.spinee.2018.01.005
Maulucci CM, Ghobrial GM, Sharan AD et al (2014) Correlation of posterior occipitocervical angle and surgical outcomes for occipitocervical fusion. Evid Based Spine Care J 5(2):163–165. https://doi.org/10.1055/s-0034-1386756
Fu KM, Smith JS, Polly DW Jr et al (2011) Scoliosis Research Society Morbidity and Mortality Committee. Correlation of higher preoperative American Society of Anesthesiology grade and increased morbidity and mortality rates in patients undergoing spine surgery. J Neurosurg Spine 14(4):470–474. https://doi.org/10.3171/2010.12
Funding
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB). There was no financial support to perform this work from any company or institute.
Author information
Authors and Affiliations
Contributions
MAI designed the study, collected the data, carried out the statistical analysis, wrote and revised the manuscript, and reviewed the literature. HB designed the study, collected the data and critically reviewed the manuscript. HAEG and AA designed the study and revised the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
There are no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ismail, M.A., Boehm, H., El Ghait, H.A. et al. Surgical treatment of craniocervical instability: comparison of two constructs regarding clinical and radiological outcomes of 100 patients. Eur Spine J 32, 3511–3521 (2023). https://doi.org/10.1007/s00586-023-07795-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-023-07795-1