
Abstract
Stature estimation is one of the most basic and important methods of personal identification. The long bones of the limbs provide the most accurate stature estimation, with the femur being one of the most useful. In all the previously reported methods of stature estimation using computed tomography (CT) images of the femur, laborious manual measurement was necessary. A semi-automatic bone measuring method can simplify this process, so we firstly reported a stature estimation process using semi-automatic bone measurement software equipped with artificial intelligence. Multiple measurements of femurs of adult Japanese cadavers were performed using automatic three-dimensional reconstructed CT images of femurs. After manually setting four points on the femur, an automatic measurement was acquired. The relationships between stature and five femoral measurements, with acceptable intraobserver and interobserver errors, were analyzed with single regression analysis using the standard error of the estimate (SEE) and the coefficient of determination (R2). The maximum length of the femur (MLF) provided the lowest SEE and the highest R2; the SEE and R2 in all cadavers, males and females, respectively, were 3.913 cm (R2 = 0.842), 3.664 cm (R2 = 0.705), and 3.456 cm (R2 = 0.686) for MLF on the right femur, and 3.837 cm (R2 = 0.848), 3.667 cm (R2 = 0.705), and 3.384 cm (R2 = 0.699) for MLF on the left femur. These results were non-inferior to those of previous reports regarding stature estimation using the MLF. Stature estimation with this simple and time-saving method would be useful in forensic medical practice.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Stature estimation is one of the most important and basic methods for individual identification as well as for sex and age estimation [1,2,3,4,5,6,7,8,9,10]. Recent forensic anthropology reports have described sex, weight, and age estimation using computed tomographic (CT) images of bones [11,12,13,14,15,16,17,18,19,20,21,22]. Regarding stature estimation, the long bones of the limbs provide the most accurate stature estimation over a wide age range in studies conducted on different races. Among them, the femur is reported as one of the most useful for stature estimation [4, 10, 23,24,25,26,27,28,29,30].
Conventionally, the femur is measured using an osteometric board, which is placed on a horizontal plane [31,32,33,34,35]. In recent reports, the femur was measured using X-ray photography [36,37,38]. Some reports have provided stature estimation using CT images of the femur [39,40,41,42,43,44], and researchers in these studies manually measured the femur on CT images for estimation. However, manual measurement requires a certain level of technical proficiency and can be affected by the performance of the measurer. Thus, using a simpler measurement method than the manual method may provide benefits such as reduction of time and effort required for measurement and prevention of unintentional measurement errors. Herein, we created three-dimensional (3D) reconstructed images from postmortem CT images and measured the femur using a semi-automatic measurement software, with the aim of providing new stature estimation formulae based on these semi-automatic measurements.
Materials and methods
This study included 300 cadavers of known sex and age over 18 that underwent whole-body postmortem CT imaging and subsequent forensic autopsy at the forensic medicine departments at Chiba University and the University of Tokyo in Japan between October 2016 and October 2020. Cadavers with severe decomposition, burn injuries, congenital malformations, postoperative changes, missing parts, femoral fractures, severe deformation of the vertebral bodies, and severe trauma to the head, neck, trunk, or lower limbs were excluded because such conditions have possible effects on the condition of the femur or stature. We included the cadavers of 150 males (10–20 years, n = 1; 21–30 years, n = 21; 31–40 years, n = 19; 41–50 years, n = 37; 51–60 years, n = 38; 61–70 years, n = 20; 71–80 years, n = 12; 81–90 years, n = 2) and 150 females (10–20 years, n = 13; 21–30 years, n = 12; 31–40 years, n = 28; 41–50 years, n = 24; 51–60 years, n = 21; 61–70 years, n = 18; 71–80 years, n = 20; 81–90 years, n = 14). Cadaver stature was measured in the supine position before autopsy using a measuring tape or a ruler. The adjusted stature (AS) was calculated by subtracting 2.0 cm from the measured stature to obtain an estimate of the living stature according to previous studies [45,46,47,48].
At Chiba University, postmortem CT was performed using a 64-row detector CT system (Supria Grande; Fujifilm Healthcare Corporation, Tokyo, Japan), and the scanning protocol was as follows: tube voltage, 120 kV; tube current, 250 mA; scan time, 0.75 s; collimation, 0.625 mm. The slice thickness, reconstruction interval, and field of view during image reconstruction were 1.0, 0.725, and 500 mm, respectively. At the University of Tokyo, postmortem CT was performed using a 16-row detector CT system (ECLOS; Fujifilm Healthcare Corporation), and the scanning protocol was as follows: tube voltage, 120 kV; tube current, 200 mA; scan time, 1 s; collimation, 1.25 mm. The slice thickness, reconstruction interval, and field of view during image reconstruction were 1.25, 1.25, and 500 mm, respectively.
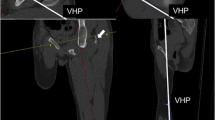
Image data were processed on a workstation (Synapse Vincent; Fujifilm Medical), and a semi-automatic application was used to measure the femur. Just after launching, this application automatically recognizes the femur and displays it as a reconstructed 3D image. If it contains other structures, such as calcified blood vessels or cartilage, manual adjustments are necessary. After confirmation that the reconstruction is appropriate, the bone surface information is automatically extracted with a single click. By manually marking the four points—the center of the femoral head, intercondylar notch (ICN), medial epicondyle, and lateral epicondyle—on the model (Fig. 1), 41 measurements are automatically calculated and displayed (Table 1). The time required from manual marking to displaying the results was approximately 40 s. Using the results of each cadaver, the average values of the right and left femurs were also calculated (Fig. 2).

Four points where manual marking are necessary (each picture shows one point in the horizontal, coronal, and sagittal planes and the three-dimensional reconstruction of the computed tomography images). a Center of the femoral head: the central point of the femoral head. b Intercondylar notch: posterior 1/4 point on the midline of the recess located between the medial and lateral condyles on the bottom surface of the lower end of the femur. c Medial epicondyle: the most medial point of the medial condyle. d Lateral epicondyle: the most lateral point of the lateral condyle

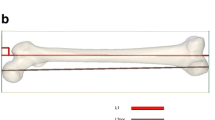
Five measurements with acceptable intraobserver and interobserver errors. a Maximum length of the femur (MLF). b Lateral anterior–posterior length (LAP). c Cross-section medial–lateral width (C-ML). d C-lateral anterior–posterior length (C-LAP). e C-medial anterior–posterior length (C-MAP)
First, to select measurements with acceptable intraobserver and interobserver errors, 20 cadavers were randomly selected. To evaluate the intraobserver error, a single researcher measured the femurs twice with an interval of ≥ 1 day for each cadaver. To evaluate the interobserver error, another researcher measured the femurs, and the result was then compared with the first result from the first researcher. The intraobserver and interobserver errors were assessed with the technical error of measurement (TEM), relative technical error of measurement (rTEM), and coefficient of reliability (R) [49, 50]. The acceptance range for rTEM was set at < 1.5% for intraobserver error and < 2.0% for interobserver error [51].
Second, the sexual differences in age, AS, and acceptable measurement were evaluated. If these values followed a normal distribution, Student’s t-test was used. If the values did not follow a normal distribution, the Wilcoxon rank sum test was used instead [52, 53]. The absolute z values of skewness and kurtosis were used to assess normal distribution [54].
Lastly, the relationship between AS and each measurement for all 300 cadavers was assessed using single regression analysis with the statistical values of the coefficient of determination (R2) and the standard error of the estimate (SEE). In this analysis, all manual markings were performed by a single researcher. A residual plot was created with the predicted stature calculated with the obtained regression equation, and the difference between the predicted stature and AS and the existence of heteroscedasticity was examined [55].
Statistical significance was set at P < 0.05 to reject the null hypothesis that there was no significant difference in statistical values between males and females and that the regression coefficient was 0. Statistical analysis was performed using Excel 2010 (Microsoft Corporation, Redmond, WA, USA).
Results
The 41 measurements were classified into groups 1 and 2 based on the results of intraobserver and interobserver errors (Table 2), and the TEM, rTEM, and R values for each measurement of both the right and left femurs are shown in Table 3. Group 1 included measurements with rTEM values < 1.5% for intraobserver error and < 2.0% for interobserver error on both the right and left sides. Group 2 included the other measurements whose rTEM values for intraobserver or interobserver errors were larger than the acceptable range. Group 1 comprised five measurements: maximum length of the femur (MLF), lateral anterior–posterior length (LAP), cross-section medial–lateral width (C-ML), C-lateral anterior–posterior length (C-LAP), and C-medial anterior–posterior length (C-MAP), for which R values were > 0.9. Group 2 was classified into groups 2–1 and 2–2 according to measurement type. Group 2–1 included measurements for angles and curvature radii, and group 2–2 included measurements for length.
The descriptive statistics for age, AS, and five group 1 measurements are presented in Table 4. Age, AS, MLF, LAP, C-LAP and C-MAP followed a normal distribution, while only C-ML did not follow a normal distribution. There was no significant difference in mean age between the sexes (P = 0.482). The mean values of AS and of each measurement were significantly greater in men than in women (C-ML, P < 0.01; AS, MLF, LAP, C-LAP, and C-MAP, P < 0.001).
Table 5 describes the result of the single linear regression analysis for estimating AS using five group 1 measurements for all cadavers, regardless of sex. Tables 6 and 7 show the results for males and females, respectively. Significant positive correlations were observed between the AS and each measurement. MLF had the strongest correlation and the lowest SEE for all cadavers, while LAP had the second strongest correlation and lowest SEE. Figures 3, 4, and 5 show the residual plots for the five measurements.

Residual distribution for all samples regardless of sex with the five measurements. a1: Right MLF (maximum length of the femur): a2: left MLF, a3: average MLF; b1: right LAP (lateral anterior–posterior length): b2: left LAP, b3: average LAP; c1: right C-ML (cross-section medial–lateral width): c2: left C-ML, c3: average C-ML; d1: right C-LAP (C-lateral anterior–posterior length): d2: left C-LAP, d3: average C-LAP; e1: right C-MAP (C-medial anterior–posterior length), e2: Left C-MAP, e3: average C-MAP. AS, adjusted stature, PS, predicted stature calculated with the obtained regression equation

Residual distribution for male samples with the five measurements. a1: right MLF (maximum length of the femur): a2: left MLF, a3: average MLF; b1: right LAP (lateral anterior–posterior length): b2: left LAP, b3: average LAP; c1: right C-ML (cross-section medial–lateral width): c2: left C-ML, c3: Average C-ML; d1: right C-LAP (C-lateral anterior–posterior length): d2: left C-LAP, d3: average C-LAP; e1: right C-MAP (C-medial anterior–posterior length): e2: left C-MAP, e3: average C-MAP. AS, adjusted stature, PS: predicted stature calculated with the obtained regression equation

Residual distribution for female samples with the five measurements. a1: right MLF (maximum length of the femur): a2: left MLF, a3: average MLF; b1: right LAP (lateral anterior–posterior length): b2: left LAP, b3: average LAP; c1: right C-ML (cross-section medial–lateral width): c2: left C-ML, c3: average C-ML; d1: right C-LAP (C-lateral anterior–posterior length): d2: left C-LAP, d3: average C-LAP; e1: right C-MAP (C-medial anterior–posterior length): e2: left C-MAP, e3: average C-MAP. AS, adjusted stature; PS, predicted stature calculated with the obtained regression equation
Discussion
In this study, we obtained stature estimation formulae based on a 3D model reconstructed from CT images using semi-automatic measurement software. This is the first report that obtained stature estimation formulae from measurements in 3D CT-reconstructed images using semi-automatic measurement software. In the present study, artificial intelligence (AI) was used for recognition of the femur, extraction of bone surface information, and semi-automatic measurement. AI has been applied in multiple fields of medical research. In the field of diagnostic imaging, it has been shown to reduce not only time for analysis but also interreader variability or false-positive markings [56,57,58,59]. Furthermore, AI has been shown to improve adenoma detection rates and reduce examination time in colonoscopy [60], thus reducing waiting time for outpatients [61] and the time interval between CT angiography at a primary stroke center to door-in at a comprehensive stroke center [62]. In the present study, the advantages of using a semi-automatic measurement software were the following: it is a simple measurement method; the time required for measurement is short (approximately 1 min); multiple measurements can be obtained with a single method.
Previously, some stature estimation methods with a single linear regression analysis from MLF measured using radiographic images were reported (Table 8). In two previous reports that presented intraobserver and interobserver errors [40, 44], the rTEM values for intraobserver errors were 0.108–0.277 and those for interobserver errors were 0.192–0.289. In this report, the rTEM values for intraobserver errors were 0.034–0.035 and those for interobserver errors were 0.018–0.019, which were lower than in these two reports. It is possible that these errors were reduced using semi-automatic measurement software.
Compared with previous reports [37, 40, 42, 44] of Japanese cadavers, the results of R2 and SEE in this study were either better or at least not inferior; therefore, the stature estimation formulae determined in this study could be useful in forensic medical practice. Compared with previous reports providing stature estimations using CT images of Japanese femurs [40, 42, 44], the present study observed the lowest SEE in males, whereas the SEE in females was the second lowest after Chiba et al. [44], and the difference was < 0.2 cm. In their report, MLF was manually measured by reproducing the conventional anthropological measurement method using a CT arbitrary cross-section reconstruction image. Although it may be highly applicable to conventional bone measurements, their measurement method is complicated and time consuming, taking approximately 140 s for measuring MLF, and approximately 440 s for measuring the 5 measurements needed for single side written in the research [44]. In contrast, the semi-automatic measurement method examined in this study is much simpler and faster. It took approximately 40 s from manual marking to displaying 41 measurements, and approximately 280 s from launching this application to displaying all the results. This time period includes measurements of both sides of the femur and includes the time required for 3D model reconstruction. Since the semi-automatic measurement method reduced the measurement error and shortened the measurement time, it is expected that if a fully automatic measuring method is developed, it will be possible to measure with smaller errors and shorter measurement time than the results of this study currently show.
Hasegawa et al. [37] showed lower SEE values in females than those observed in this study (difference, > 0.3 cm), and their report showed the best results in terms of SEE in Japanese subjects, as shown in Table 8 [37, 40, 42, 44]. However, the SEE in males was slightly higher than that observed in males in this study. In addition, the difference in SEE between males and females was 0.74 and 0.83, which was greater than difference in this study (0.003 and 0.072). Hasegawa et al. [37] provided stature estimation formulae using an X-ray photograph of a living human. The difference between this report and theirs might be because their patients were alive, the radiation imaging device was different, and the number of female samples was higher than that of the male samples in their study.
Comparison of the present study with those of Zhang et al. [63] and Lee et al. [39] is complicated because the subjects are different, but our results were superior to those of Zhang et al. [63] and slightly inferior to those of Lee et al. [39]. Zhang et al. [63] studied a smaller number of cadavers than this study; therefore, the difference might be due to the sample size. Meanwhile, Lee et al. [39] had more cadavers with age of 41–60 years (65.8% for men and 45.1% for women) than our report (50.0% for men and 30.0% for women). They might have obtained better results of stature estimation formulae than this study, whose age groups of cadavers were scattered because their stature estimation formulae were adapted to the age groups that comprised most of their cadavers. The difference in age composition ratio, CT equipment, or image reconstruction software may have affected the results.
Many reports have shown that MLF is useful for stature estimation, consistent with our finding that stature estimation with MLF showed the best performance. However, it is impossible to measure MLF if only part of the femur remains. In this study, stature estimation using LAP showed the second lowest SEE. This suggests that LAP would be useful for stature estimation if the MLF cannot be measured, for example, if only the lower part of the femur remains. Although some reports provided stature estimation formulae using measurements of the lower part of the femur [29, 44, 64, 65], no report has suggested that LAP is useful for stature estimation. The high values of SEE for LAP and the three measurements, C-ML, C-LAP, and C-MAP, were not negligible. However, of all the studies that performed stature estimation using the measurements of the lateral side of the femur, only Chiba et al. [44] calculated SEE. They reported that the SEEs calculated from femoral epicondylar breadth (linear distance between projection points of the most medial and lateral epicondyles projected vertically to the horizontal) was 5.620–6.300. Compared to their study, SEEs calculated from LAP showed better results, and SEEs calculated from other measurements were not inferior. Since there are few comparison targets, further research on stature estimation using the measurements of the distal part of the femur is desirable in future studies.
Among the 41 measurements that were semi-automatically measured in the present study, group 2 measurements had large intraobserver and interobserver errors outside the permissible range. Descriptive statistics for the measurements corresponding to group 2 are shown in Online Resource 1. There are several possible reasons for the higher measurement errors in group 2 measurements. Group 2–1 measurements were based on information from the edge of the reconstructed 3D CT model. Therefore, the slight difference in construction due to the manual removal of calcified blood vessels and cartilage might have resulted in a large error. Group 2–2 measurements, except MAP, had smaller values than those of group 1, as shown in Table 4 and Online Resource 1. Therefore, the error caused by manual operation might have had a significant influence on these measurements. MAP had similar values to those of group 1 measurements, but it also had higher measurement errors. Unlike C-ML, C-LAP, and C-MAP, MAP is measured without creating a cross section at the lower part of the femur. The deformation of the knee joint, including the distal end of the femur, might have occurred in most of the cadavers in this study because primary knee osteoarthritis often occurs in people over 50 years old [66, 67]. This change may have made it difficult for the AI software to have identified them. In some cadavers, the software used in this study mistakenly recognized the knee cartilage and patella as part of the femur when it identified the femur, and the structure other than the femur had to be manually removed. This manual operation might have caused higher measurement errors. In addition, MAP had a larger measurement error than LAP, which was also measured without creating a cross section. This may be because osteoarthritis occurs more frequently on the medial side than on the lateral side [64].
The residual plots indicated that the two measurements, MLF and LAP, were good models for calculating regression equations. The other three measurements were difficult to adopt for the regression equations, because of the large outliers and a small range of predicted values, especially in the residual plots using single-sex. This may be attributed to the small range of the three measurements.
This study has several limitations. The measurements useful in other reports, such as the femoral diaphysis length, physiological length, or bicondylar length [13, 29, 65, 68, 69], were not measured because the semi-automatic measurement application was not configured to measure them. Furthermore, the application was developed by Fujifilm, including measurements selection. The femurs measured in this study were collected only from cadavers with soft tissue, so further studies examining the difference between digital and analog measurements are warranted. Femur deformation due to aging was not considered. In this research, the stature of the cadavers was recalculated in AS, and the estimation formulae were assessed, but since the actual stature was measured only once, intra- and inter-observer errors were not evaluated for the stature. Age-stratified analysis was not performed because of the insufficient sample size in this study. In addition, this study was performed using images captured with two types of CT equipment. Further studies comparing and examining images acquired with different CT devices are warranted.
Conclusion
This study provided the first stature estimation formulae based on a 3D CT model of modern Japanese femurs using a simple and rapid semi-automatic measurement software. For stature estimation with this method, MLF was the best, and LAP was the second-best measurement using 41 total measurements. These formulae can be useful in forensic investigations.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Code availability
Code sharing not applicable to this article as no codes were generated or analyzed during the current study.
References
Pearson K (1899) IV. Mathematical contributions to the theory of evolution.—V. On the reconstruction of the stature of prehistoric races. Phil Trans R Soc Lond A 192:169–244. https://doi.org/10.1098/rsta.1899.0004
Breitinger E (1937) Zur Berechnung der Körperhöhe aus den langen Gliedmaßenknochen. Anthropol Anz 14:249–274
Trotter M, Gleser GC (1951) The effect of ageing on stature. Am J Phys Anthropol 9:311–324. https://doi.org/10.1002/ajpa.1330090307
Trotter M, Gleser GC (1952) Estimation of stature from long bones of American Whites and Negroes. Am J Phys Anthropol 10:463–514. https://doi.org/10.1002/ajpa.1330100407
Olivier G, Aaron C, Fully G, Tissier G (1978) New estimations of stature and cranial capacity in modern man. J Hum Evol 7:513–518. https://doi.org/10.1016/S0047-2484(78)80020-7
Zeybek G, Ergur I, Demiroglu Z (2008) Stature and gender estimation using foot measurements. Forensic Sci Int 181:54.e1-54.e5. https://doi.org/10.1016/j.forsciint.2008.08.003
Duyar I, Pelin C (2003) Body height estimation based on tibia length in different stature groups. Am J Phys Anthropol 122:23–27. https://doi.org/10.1002/ajpa.10257
Mullins RA, Albanese J (2018) Estimating biological characteristics with virtual laser data. J Forensic Sci 63:815–823. https://doi.org/10.1111/1556-4029.13621
Asadujjaman M, Al Noman SN, Molla MBA (2020) Stature estimation from foot anthropometric measurements in Bangladeshi population. Ir J Med Sci 189:365–372. https://doi.org/10.1007/s11845-019-02048-x
Mahakkanukrauh P, Khanpetch P, Prasitwattanseree S, Vichairat K, Troy Case DT (2011) Stature estimation from long bone lengths in a Thai population. Forensic Sci Int 210:279.e1-279.e7. https://doi.org/10.1016/j.forsciint.2011.04.025
Zhang K, Luo YZ, Fan F, Zheng JQ, Yang M, Li T, Pang T, Zhang J, Deng ZH (2015) Stature estimation from sternum length using computed tomography-volume rendering technique images of western Chinese. J Forensic Leg Med 35:40–44. https://doi.org/10.1016/j.jflm.2015.07.003
Giurazza F, Del Vescovo R, Schena E, Cazzato RL, D’Agostino F, Grasso RF, Silvestri S, Zobel BB (2013) Stature estimation from scapular measurements by CT scan evaluation in an Italian population. Leg Med (Tokyo) 15:202–208. https://doi.org/10.1016/j.legalmed.2013.01.002
Giurazza F, Del Vescovo R, Schena E, Battisti S, Cazzato RL, Grasso FR, Silvestri S, Denaro V, Zobel BB (2012) Determination of stature from skeletal and skull measurements by CT scan evaluation. Forensic Sci Int 222:398.e1-398.e9. https://doi.org/10.1016/j.forsciint.2012.06.008
Villa C, Hansen MN, Buckberry J, Cattaneo C, Lynnerup N (2013) Forensic age estimation based on the trabecular bone changes of the pelvic bone using post-mortem CT. Forensic Sci Int 233:393–402. https://doi.org/10.1016/j.forsciint.2013.10.020
Lorkiewicz-Muszyńska D, Przystańska A, Kociemba W, Sroka A, Rewekant A, Żaba C, Paprzycki W (2013) Body mass estimation in modern population using anthropometric measurements from computed tomography. Forensic Sci Int 231:405.e1-405.e6. https://doi.org/10.1016/j.forsciint.2013.05.017
Chiba F, Makino Y, Motomura A, Inokuchi G, Torimitsu S, Ishii N, Sakuma A, Nagasawa S, Saitoh H, Yajima D, Hayakawa M, Odo Y, Suzuki Y, Iwase H (2013) Age estimation by multidetector CT images of the sagittal suture. Int J Legal Med 127:1005–1011. https://doi.org/10.1007/s00414-013-0883-y
Torimitsu S, Makino Y, Saitoh H, Ishii N, Yajima D, Inokuchi G, Motomura A, Chiba F, Yamaguchi R, Hoshioka Y, Iwase H (2018) Determination of sex on the basis of hyoid bone measurements in a Japanese population using multidetector computed tomography. Int J Legal Med 132:907–914. https://doi.org/10.1007/s00414-017-1728-x
Torimitsu S, Makino Y, Saitoh H, Sakuma A, Ishii N, Yajima D, Inokuchi G, Motomura A, Chiba F, Yamaguchi R, Hashimoto M, Hoshioka Y, Iwase H (2016) Sexual determination based on multidetector computed tomographic measurements of the second cervical vertebra in a contemporary Japanese population. Forensic Sci Int 266:588.e1-588.e6. https://doi.org/10.1016/j.forsciint.2016.04.010
Torimitsu S, Makino Y, Saitoh H, Sakuma A, Ishii N, Yajima D, Inokuchi G, Motomura A, Chiba F, Yamaguchi R, Hashimoto M, Hoshioka Y, Iwase H (2017) Stature estimation in a contemporary Japanese population based on clavicular measurements using multidetector computed tomography. Forensic Sci Int 275:316.e1-316.e6. https://doi.org/10.1016/j.forsciint.2017.02.037
Torimitsu S, Makino Y, Saitoh H, Sakuma A, Ishii N, Inokuchi G, Motomura A, Chiba F, Hoshioka Y, Iwase H (2015) Estimation of sex in Japanese cadavers based on sternal measurements using multidetector computed tomography. Leg Med (Tokyo) 17:226–231. https://doi.org/10.1016/j.legalmed.2015.01.003
Torimitsu S, Makino Y, Saitoh H, Sakuma A, Ishii N, Hayakawa M, Inokuchi G, Motomura A, Chiba F, Hoshioka Y, Iwase H (2015) Stature estimation in Japanese cadavers based on the second cervical vertebra measured using multidetector computed tomography. Leg Med (Tokyo) 17:145–149. https://doi.org/10.1016/j.legalmed.2014.11.003
Chiba F, Makino Y, Motomura A, Inokuchi G, Torimitsu S, Ishii N, Kubo Y, Abe H, Sakuma A, Nagasawa S, Saitoh H, Yajima D, Hayakawa M, Miura M, Iwase H (2014) Age estimation by quantitative features of pubic symphysis using multidetector computed tomography. Int J Legal Med 128:667–673. https://doi.org/10.1007/s00414-014-1010-4
Jeong Y, Jantz LM (2016) Developing Korean-specific equations of stature estimation. Forensic Sci Int 260:105.e1-105.e11. https://doi.org/10.1016/j.forsciint.2015.12.048
Trotter M, Gleser GC (1958) A re-evaluation of estimation of stature based on measurements of stature taken during life and of long bones after death. Am J Phys Anthropol 16:79–123. https://doi.org/10.1002/ajpa.1330160106
Auerbach BM, Ruff CB (2010) Stature estimation formulae for indigenous North American populations. Am J Phys Anthropol 141:190–207. https://doi.org/10.1002/ajpa.21131
Monum T, Prasitwattanseree S, Das S, Siriphimolwat P, Mahakkanukrauh P (2017) Sex estimation by femur in modern Thai population. Clin Ter 168:e203–e207. https://doi.org/10.7417/T.2017.2007
Ruff C (2007) Body size prediction from juvenile skeletal remains. Am J Phys Anthropol 133:698–716. https://doi.org/10.1002/ajpa.20568
Feldesman MR (1992) Femur/stature ratio and estimates of stature in children. Am J Phys Anthropol 87:447–459. https://doi.org/10.1002/ajpa.1330870406
Brits DM, Bidmos MA, Manger PR (2017) Stature estimation from the femur and tibia in Black South African sub-adults. Forensic Sci Int 270:277.e1-277.e10. https://doi.org/10.1016/j.forsciint.2016.10.013
Sládek V, Macháček J, Ruff CB, Schuplerová E, Přichystalová R, Hora M (2015) Population-specific stature estimation from long bones in the early medieval Pohansko (Czech Republic). Am J Phys Anthropol 158:312–324. https://doi.org/10.1002/ajpa.22787
Wilson RJ, Herrmann NP, Jantz LM (2010) Evaluation of stature estimation from the database for forensic anthropology. J Forensic Sci 55:684–689. https://doi.org/10.1111/j.1556-4029.2010.01343.x
Dayal MR, Steyn M, Kuykendall KL (2008) Stature estimation from bones of South African whites. Afr J Sci 104:124–128
Andou M (1923) Nihonjin (seijin) no shishikotsu no keisoku ni oite. Kokka Igaku Zasshi 434:101–120 (in Japanese)
Fujii A (1960) On the relation of long bone length of limbs to stature. Juntendoudaigaku Taiikugakubu Kiyo 3:49–61 (in Japanese with English abstract)
White TD, Black MT, Folkens PA (2011) Human osteology, 3rd edn. Academic Press, New York
Sağir M (2006) Estimation stature from X-rays of metacarpals in the Turkish population. Anthropol Anz 64:377–388. https://doi.org/10.1127/anthranz/64/2006/377(inTurkish,withEnglishabstract)
Hasegawa I, Uenishi K, Fukunaga T, Kimura R, Osawa M (2009) Stature estimation formulae from radiographically determined limb bone length in a modern Japanese population. Leg Med (Tokyo) 11:260–266. https://doi.org/10.1016/j.legalmed.2009.07.004
Cui JH, Luo YZ, Chang YF, Peng Z, Deng LP, Zhang K, Deng ZH (2019) Stature estimation of Sichuan Han females based on X-ray photography of total lower limbs. Fa Yi Xue Za Zhi 35:11–16. https://doi.org/10.12116/j.issn.1004-5619.2019.01.003 (in Chinese, with English abstract)
Lee S, Gong HH, Hyun JY, Koo HN, Lee HY, Chung NE, Choi YS, Yang KM, Ha Choi BH (2017) Estimation of stature from femur length measured using computed tomography after the analysis of three-dimensional characteristics of femur bone in Korean cadavers. Int J Legal Med 131:1355–1362. https://doi.org/10.1007/s00414-017-1556-z
Hishmat AM, Michiue T, Sogawa N, Oritani S, Ishikawa T, Fawzy IA, Hashem MA, Maeda H (2015) Virtual CT morphometry of lower limb long bones for estimation of the sex and stature using postmortem Japanese adult data in forensic identification. Int J Legal Med 129:1173–1182. https://doi.org/10.1007/s00414-015-1228-9
Imai N, Funayama K, Suzuki H, Tsuchiya K, Nozaki A, Minato I, Miyasaka D, Endo N (2020) Stature estimation formulae based on bony pelvic dimensions and femoral length. Homo 71:111–119. https://doi.org/10.1127/homo/2020/1116
Nishio H (2013) Stature estimation based on the lengths of the long bones of the extremities according to post-mortem computed tomography. Res Pract Forensic Med 56:223–235
Zech WD, Näf M, Siegmund F, Jackowski C, Lösch S (2016) Body height estimation from post-mortem CT femoral F1 measurements in a contemporary Swiss population. Leg Med (Tokyo) 19:61–66. https://doi.org/10.1016/j.legalmed.2016.02.004
Chiba F, Makino Y, Torimitsu S, Motomura A, Inokuchi G, Ishii N, Hoshioka Y, Abe H, Yamaguchi R, Sakuma A, Nagasawa S, Saito H, Yajima D, Fukui Y, Iwase H (2018) Stature estimation based on femoral measurements in the modern Japanese population: a cadaveric study using multidetector computed tomography. Int J Legal Med 132:1485–1491. https://doi.org/10.1007/s00414-018-1834-4
De Mendonça MC (2000) Estimation of height from the length of long bones in a Portuguese adult population. Am J Phys Anthropol 112:39–48. https://doi.org/10.1002/(SICI)1096-8644(200005)112:1%3c39::AID-AJPA5%3e3.0.CO;2-#
Meadows L, Jantz RL (1992) Estimation of stature from metacarpal lengths. J Forensic Sci 37:147–154. https://doi.org/10.1520/JFS13222J
Telkka A (1950) On the prediction of human stature from the long bones. Acta Anat (Basel) 9:103–117. https://doi.org/10.1159/000140434
Radoinova D, Tenekedjiev K, Yordanov Y (2002) Stature estimation from long bone lengths in Bulgarians. Homo 52:221–232. https://doi.org/10.1078/0018-442x-00030
Arroyo M, Freire M, Ansotegui L, Rocandio AM (2010) Intraobserver error associated with anthropometric measurements made by dietitians. Nutr Hosp 25:1053–1056. https://doi.org/10.3305/nh.2010.25.6.4854
Mueller WH, Malina RM (1987) Relative reliability of circumferences and skinfolds as measures of body fat distribution. Am J Phys Anthropol 72:437–439. https://doi.org/10.1002/ajpa.1330720404
Jamaiyah H, Geeta A, Safiza MN, Khor GL, Wong NF, Kee CC, Rahmah R, Ahmad AZ, Suzana S, Chen WS, Rajaah M, Adam B (2010) Reliability, technical error of measurements and validity of length and weight measurements for children under two years old in Malaysia. Med J Malaysia 65 Supplement A:131–137
Wright DB, Herrington JA (2011) Problematic standard errors and confidence intervals for skewness and kurtosis. Behav Res Methods 43:8–17. https://doi.org/10.3758/s13428-010-0044-x
McGee M (2018) Case for omitting tied observations in the two-sample t-test and the Wilcoxon-Mann-Whitney test. PLoS ONE 13:e0200837. https://doi.org/10.1371/journal.pone.0200837
Kim HY (2013) Statistical notes for clinical researchers: assessing normal distribution (2) using skewness and kurtosis. Restor Dent Endod 38:52–54. https://doi.org/10.5395/rde.2013.38.1.52
Bilić-Zulle Lidija (2011) Comparison of methods: passing and Bablok regression. Biochem Med (Zagreb) 21(1):49–52. https://doi.org/10.11613/bm.2011.010
Leiner T, Rueckert D, Suinesiaputra A, Baeßler B, Nezafat R, Išgum I, Young AA (2019) Machine learning in cardiovascular magnetic resonance: basic concepts and applications. J Cardiovasc Magn Reson 21:61. https://doi.org/10.1186/s12968-019-0575-y
Rueckel J, Reidler P, Fink N, Sperl J, Geyer T, Fabritius MP, Ricke J, Ingrisch M, Sabel BO (2021) Artificial intelligence assistance improves reporting efficiency of thoracic aortic aneurysm CT follow-up. Eur J Radiol 134:109424. https://doi.org/10.1016/j.ejrad.2020.109424
Mayo RC, Kent D, Sen LC, Kapoor M, Leung JWT, Watanabe AT (2019) Reduction of false-positive markings on mammograms: a retrospective comparison study using an artificial intelligence-based CAD. J Digit Imaging 32:618–624. https://doi.org/10.1007/s10278-018-0168-6
Leite AF, Van Gerven AV, Willems H, Beznik T, Lahoud P, Gaêta-Araujo H, Vranckx M, Jacobs R (2021) Artificial intelligence-driven novel tool for tooth detection and segmentation on panoramic radiographs. Clin Oral Investig 25:2257–2267. https://doi.org/10.1007/s00784-020-03544-6
Sinagra E, Badalamenti M, Maida M, Spadaccini M, Maselli R, Rossi F, Conoscenti G, Raimondo D, Pallio S, Repici A, Anderloni A (2020) Use of artificial intelligence in improving adenoma detection rate during colonoscopy: might both endoscopists and pathologists be further helped. World J Gastroenterol 26:5911–5918. https://doi.org/10.3748/wjg.v26.i39.5911
Li X, Tian D, Li W, Dong B, Wang H, Yuan J, Li B, Shi L, Lin X, Zhao L, Liu S (2021) Artificial intelligence-assisted reduction in patients’ waiting time for outpatient process: a retrospective cohort study. BMC Health Serv Res 21:237. https://doi.org/10.1186/s12913-021-06248-z
Hassan AE, Ringheanu VM, Rabah RR, Preston L, Tekle WG, Qureshi AI (2020) Early experience utilizing artificial intelligence shows significant reduction in transfer times and length of stay in a hub and spoke model. Interv Neuroradiol 26:615–622. https://doi.org/10.1177/1591019920953055
Zhang Q, Paz AR, Banner J, Jørkov MLS, Villa C (2020) Stature estimation from postmortem CT femoral maximum length in contemporary Danish population. J Forensic Sci 65:930–938. https://doi.org/10.1111/1556-4029.14254
Miyasaka T, Saito M, Kurosaka D, Ikeda R, Yamanaka S, Marumo K (2020) Impact of posterior femoral condylar cartilage and posterior intercondylar distance on rotation of femoral component in total knee arthroplasty. BMC Musculoskelet Disord 21:498. https://doi.org/10.1186/s12891-020-03537-2
Menéndez Garmendia AM, Sánchez-Mejorada G, Gómez-Valdés JA (2018) Stature estimation formulae for Mexican contemporary population: a sample based study of long bones. J Forensic Leg Med 54:87–90. https://doi.org/10.1016/j.jflm.2017.12.019
Garstang SV, Stitik TP (2006) Osteoarthritis: epidemiology, risk factors, and pathophysiology. Am J Phys Med Rehabil 85 (11) Supplement: S2-S11; quiz S12. https://doi.org/10.1097/01.phm.0000245568.69434.1a
Mine K, Nakayama T, Milanese S, Grimmer K (2017) The effectiveness of braces and orthoses for patients with knee osteoarthritis: a systematic review of Japanese-language randomised controlled trials. Prosthet Orthot Int 41:115–126. https://doi.org/10.1177/0309364616640926
Bidmos MA (2008) Estimation of stature using fragmentary femora in indigenous South Africans. Int J Legal Med 122:293–299. https://doi.org/10.1007/s00414-007-0206-2
Anzellini A, Toyne JM (2020) Estimating the stature of ancient high-altitude Andean populations from skeletal remains of the Chachapoya of Peru. Am J Phys Anthropol 171:539–549. https://doi.org/10.1002/ajpa.23977
Zhang Y, Wang X, Shao Y, Xia Q (2018) The orientation of the surgical epicondylar axis varies in varus and non-varus knees in the coronal plane. Knee Surg Sports Traumatol Arthrosc 26:2580–2586. https://doi.org/10.1007/s00167-016-4386-5
Berger RA, Rubash HE, Seel MJ, Thompson WH, Crossett LS (1993) Determining the rotational alignment of the femoral component in total knee arthroplasty using the epicondylar axis. Clin Orthop Relat Res 286:40–47. https://doi.org/10.1097/00003086-199301000-00008
Author information
Authors and Affiliations
Contributions
All authors contributed to the conception and design of the study. Material preparation, data collection, and analysis were performed by Kei Kira and Fumiko Chiba. The first draft of the manuscript was written by Kei Kira, and all authors commented on the previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
The experimental protocol was approved by the Ethical Review Board of Chiba University (2987) and the University of Tokyo (10835–1).
Consent to participate
This study provided sufficient protection of the privacy of the patients and their families as per the Japanese Protection Guideline of Personal Information on Research Publication in Legal Medicine, and the requirements of informed consent from the next of kin was waived by the Ethical Review Board.
Consent for publication
This study provided sufficient protection of the privacy of the patients and their families as per the Japanese Protection Guideline of Personal Information on Research Publication in Legal Medicine, and the requirements of informed consent from the next of kin was waived by the Ethical Review Board.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kira, K., Chiba, F., Makino, Y. et al. Stature estimation by semi-automatic measurements of 3D CT images of the femur. Int J Legal Med 137, 359–377 (2023). https://doi.org/10.1007/s00414-022-02921-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-022-02921-y