
Abstract
Background
Elevated arterial–central venous carbon dioxide partial pressure difference (AVCO2) may be an important marker to predict tissue and organ hypoperfusion in adults. We analyzed the hemodynamic data of infants with congenital heart disease who underwent corrective repair with cardiopulmonary bypass (CPB) to identify whether AVCO2 has clinical significance in early postoperative tissue hypoperfusion, occurrence of complications, and clinical outcomes.
Methods
Infants with clinical conditions of hypoperfusion, without volume responsiveness and with ineffective initial treatment, within 3 h of cardiac surgery were enrolled in this study. A pulse contour cardiac output catheter was used to monitor the cardiac index (CI). Eight measurements of arterial blood gas and central venous blood gas were taken within 42 h after surgery. Clinical data of all patients were recorded.
Results
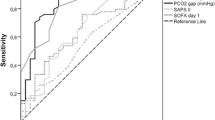
A total of 69 children were enrolled in this study. Arteriovenous oxygen difference, AVCO2, lactic acid level, and vasoactive inotropic score in the hypoperfusion group (oxygen supply/oxygen consumption ratio [DO2/VO2] of ≤ 2) were significantly higher than those in the non-hypoperfusion group (DO2/VO2 > 2), while the CI in the hypoperfusion group was significantly lower than that in the non-hypoperfusion group. The cutoff value of AVCO2 to predict DO2/VO2 ≤ 2 was 12.3 within 42 h of surgery with area under the curve of 0.84. High AVCO2 is more likely to be associated with some complications and prolonged mechanical ventilation and length of stay in the intensive care unit.
Conclusion
Elevated AVCO2 within 42 h of CPB in infants is associated with tissue and organ hypoperfusion and incidence of complications. Persistent or repeated increase in AVCO2 indicates poor prognosis.


Similar content being viewed by others


References
Mallat J, Pepy F, Lemyze M, Gasan G, Vangrunderbeeck N, Tronchon L, Vallet B, Thevenin D (2014) Central venous-to-arterial carbon dioxide partial pressure difference in early resuscitation from septic shock: a prospective observational study. Eur J Anaesthesiol 31:371–380
Mahutte CK, Jaffe MB, Sassoon CS, Wong DH (1991) Cardiac output from carbon dioxide production and arterial and venous oximetry. Crit Care Med 19:1270–1277
Pittman RN (2016) The Regulation of Tissue Oxygenation, 2nd edn. Morgan & Claypool Life Sciences, San Rafael, CA, pp 23–36
Silbert BI, Litton E, Ho KM (2015) Central venous-to-arterial carbon dioxide gradient as a marker of occult tissue hypoperfusion after major surgery. Anaesth Intensive Care 43:628–634
Robin E, Futier E, Pires O, Fleyfel M, Tavernier B, Lebuffe G, Vallet B (2015) Central venous-to-arterial carbon dioxide difference as a prognostic tool in high-risk surgical patients. Crit Care 19:227
Vincent JV, De Backer D (2013) Circulatory shock. N Engl J Med 369:1726–1734
Lim HS (2016) Cardiogenic Shock: Failure of oxygen delivery and oxygen utilization. Clin Cardiol 39:477–483
Cain SM, Curtis SE (1991) Experimental models of pathologic oxygen supply dependency. Crit Care Med 19:603–612
Cuschieri J, Rivers EP, Donnino MW, Katilius M, Jacobsen G, Nguyen HB, Pamukov N, Horst HM (2005) Central venous–arterial carbon dioxide difference as an indicator of cardiac index. Intensive Care Med 31:818–822
Ospina-Tascón GA, Bautista-Rincón DF, Umaña M, Tafur JD, Gutiérrez A, García AF, Bermúdez W, Granados M, Arango-Dávila C, Hernández G (2013) Persistently high venous-to-arterial carbon dioxide differences during early resuscitationare associated with poor outcomes in septic shock. Crit Care 17:R294
Scheeren TWL, Wicke JN, Teboul J-L (2018) Understanding the carbon dioxide gaps. Curr Opin Crit Care 24:181–189
van Beest PA, Lont MC, Holman ND (2013) Central venous–arterial pCO2 difference as a tool in resuscitation of sevptic patients. Intensive Care Med 39:1034–1039
Du W, Liu DW, Wang XT, Long Y, Chai WZ, Zhou X, Rui X (2013) Combining central venous-to-arterial partial pressure of carbon dioxide difference and central venous oxygen saturation to guide resuscitation in septic shock. J Crit Care 28:1110.e1-1110.e5
Takami Y, Masumoto H (2005) Mixed venous-arterial CO2 tension gradient after cardiopulmonary bypass. Asian Cardiovasc Thorac Annals 13:255–260
Guinot PG, Badoux L, Bernard E, Abou-Arab O, Lorne E, Dupont H (2017) Central venous-to-arterial carbon dioxide partial pressure difference in patients undergoing cardiac surgery is not related to postoperative outcomes. J Cardiothorac Vasc Anesth 31:1190–1196
Rhodes LA, Erwin WC, Borasino S, Cleveland DC, Alten JA (2017) Central venous to arterial CO2 difference after cardiac surgery in infants and neonates. Pediatr Crit Care Med 18:228–233
Akamatsu T, Inata Y, Tachibana K, Hatachi T, Takeuchi M (2017) Elevated central venous to arterial CO2 difference is not associated with poor clinical outcomes after cardiac surgery with cardiopulmonary bypass in children. Pediatr Crit Care Med 18:859–862
Funding
The Biomedical and Engineering (Science) Interdisciplinary Study Fund of Shanghai Jiaotong University. No: YG2019QNA04.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Gong, X., Zhu, L., Liu, Y. et al. Elevated Arterial–Central Venous Carbon Dioxide Partial Pressure Difference Indicates Poor Prognosis in the Early Postoperative Period of Open Heart Surgery in Infants with Congenital Heart Disease. Pediatr Cardiol 42, 1601–1606 (2021). https://doi.org/10.1007/s00246-021-02646-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-021-02646-6