
Abstract
Background
In patients who have undergone thyroidectomy and central compartment neck dissection (CCND) for papillary thyroid cancer (PTC), visualization of enlarged lymph nodes may lead to more extensive CCND. This study sought to determine the effect of patient age and the presence of thyroiditis on the number of malignant and total lymph nodes resected in patients who underwent CCND for PTC.
Methods
This retrospective review examined a prospective database of patients who underwent total thyroidectomy and CCND for PTC between April 2009 and June 2013 and had thyroiditis on the final pathology. The patients were categorized into age groups by decade (18–29, 30–39, 40–49, 50–59, and ≥60 years) and compared with a control group of patients matched by age, gender, and tumor size.
Results
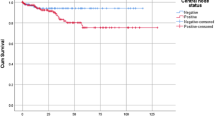
Of 74 patients with thyroiditis, 64 (87 %) were women. The median age of the patients was 47.5 years (range 18.2–72.0 years). The patients with thyroiditis had more lymph nodes resected than those without thyroiditis (median 11 vs 7; p < 0.01). However, these patients had fewer malignant lymph nodes (median 0 vs 1.5; p = 0.06), resulting in a lower lymph node ratio (0 vs 0.18; p = 0.02) for the entire cohort, but particularly for the youngest (18–29 years) and oldest (≥60 years) age groups.
Conclusions
Patients with thyroiditis and PTC who underwent CCND had more lymph nodes resected but a had lower proportion of metastatic lymph nodes than those without thyroiditis. Given the relatively low yield of malignant cervical lymphadenopathy, a more judicious approach to CCND might be considered, particularly for the youngest and oldest patients with PTC and thyroiditis.
Similar content being viewed by others


References
Noguchi S, Noguchi A, Murakami N. Papillary carcinoma of the thyroid I: developing pattern of metastasis. Cancer. 1970;26:1053–60.
Gimm G, Rath FW, Dralle H. Pattern of lymph node metastases in papillary thyroid carcinoma. Br J Surg. 1998;85:252–4.
Takada H, Kikumori T, Imai T, Sawaki M, Shibata A, Kiuchi T. Patterns of lymph node metastases in papillary thyroid carcinoma: results from consecutive bilateral cervical lymph node dissection. World J Surg. 2011;35:1560–6.
Carty SE, Cooper DS, Doherty GM, et al. Consensus statement on the terminology and classification of central neck dissection for thyroid cancer. Thyroid. 2009;19:1153–8.
Cooper DS, Doherty GM, Haugen BR, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167–214.
Giordano D, Valcavi R, Thompson GB, Pedroni C, Renna L, Gradoni P, Barbieri V. Complications of central neck dissection in patients with papillary thyroid carcinoma: results of a study on 1087 patients and review of the literature. Thyroid. 2012;22:911–7.
Kouvaraki MA, Lee JE, Shapiro SE, Sherman SI, Evans DB. Preventable reoperations for persistent and recurrent papillary thyroid carcinoma. Surgery. 2004;136:1183–91.
McLeod DSA, Sawka AM, Cooper DS. Controversies in primary treatment of low-risk papillary thyroid cancer. Lancet. 2013;381:1046–57.
Wang TS, Cheung K, Farrokhyar F, Roman SA, Sosa JA. A meta-analysis of the effect of prophylactic central compartment neck dissection on locoregional recurrence rates in patients with papillary thyroid cancer. Ann Surg Oncol. 2013;20:3477–83.
Wang TS, Evans DB, Fareau GG, Carroll T, Yen TW. Effect of prophylactic central compartment neck dissection on serum thyroglobulin and recommendations for adjuvant radioactive iodine in patients with differentiated thyroid cancer. Ann Surg Oncol. 2012;19:4217–22.
Pearce EN, Farwell AP, Braverman LE. Thyroiditis. N Engl J Med. 2003;348:2646–55.
Paksoy N, Yazal K. Cervical lymphadenopathy associated with Hashimoto’s thyroiditis. Acta Cytol. 2009;53:491–6.
Brancato D, Citarrella R, Richiusa P, Amato MC, Vetro C, Galluzzp CG. Neck lymph nodes in chronic autoimmune thyroiditis: the sonographic pattern. Thyroid. 2013;23:173–7.
Jara SM, Carson KA, Pai SI, et al. The relationship between chronic lymphocytic thyroiditis and central neck lymph node metastasis in North American patients with papillary thyroid carcinoma. Surgery. 2013;154:1272–82.
Kim SS, Lee BJ, Lee JC, et al. Coexistence of Hashimoto’s thyroiditis with papillary thyroid carcinoma: the influence of lymph node metastases. Head Neck. 2011;33:1272–7.
Schneider DF, Chen H, Sippel RS. Impact of lymph node ratio on survival in papillary thyroid cancer. Ann Surg Oncol. 2013;20:1906–11.
Paulson LM, Shindo ML, Schuff KG. Role of chronic lymphocytic thyroiditis in central node metastasis of papillary thyroid carcinoma. Otolaryngol Head Neck Surg. 2012;147:444–9.
Zhang L, Li H, Ji QH, et al. The clinical features of papillary thyroid cancer in Hashimoto’s thyroiditis patients from an area with a high prevalence of Hashimoto’s disease. BMC Cancer. 2012;12:610–7.
Ahn D, Seo HJ, Park JH, et al. Clinical relationship between Hashimoto’s thyroiditis and papillary thyroid cancer. Acta Oncol. 2011;50:1228–34.
Acknowledgment
The authors thank Dr. Jason Glenn for his assistance with statistical analysis.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Lai, V., Yen, T.W.F., Rose, B.T. et al. The Effect of Thyroiditis on the Yield of Central Compartment Lymph Nodes in Patients with Papillary Thyroid Cancer. Ann Surg Oncol 22, 4181–4186 (2015). https://doi.org/10.1245/s10434-015-4551-y
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-015-4551-y