
Abstract
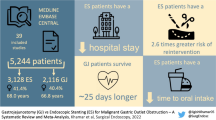
Whether nasogastric or nasojejunal decompression (ND) prevents anastomotic leakage, hastens the return of bowel function, and shortens hospital stay after gastrectomy for gastric cancer has long been controversial. We evaluated the necessity of routine ND after radical gastrectomy for gastric cancer with a systematic review and meta-analysis. We searched literature published prior to January 2014 in PubMed, Embase, Cochrane Library, Web of Science, and BIOSIS Previews for relevant randomized controlled trials (RCTs). Only prospective RCTs comparing individuals with and without ND after gastrectomy for gastric cancer were included. Outcome measures included time to first flatus, time to starting oral diet, anastomotic leakage, pulmonary complications, wound dehiscence, length of hospital stay, morbidity, and mortality. Cochrane Collaboration RevMan 5.2 software was used for the meta-analysis. Eight RCT studies fulfilled our inclusion criteria. Of the 1,141 patients in those RCTs, 570 received nasogastric or nasojejunal decompression and 571 did not. Anastomotic leakage, pulmonary complications, wound dehiscence, morbidity, and mortality were comparable between the groups. Stratified by the type of gastrectomy or gastrojejunostomy, no significant differences in above mentioned outcomes were observed in subgroup analyses. The no ND group displayed a significantly shorter time to oral diet (weighted mean difference [WMD] = 0.45, 95 % confidence interval [CI] = 0.29 to 0.61, p < 0.001) and a marginally shorter end of hospital stay (WMD = 0.48, 95 % CI = −0.01 to 0.98, p = 0.05). The ND group significantly shortened time to first flatus (WMD = −0.7, 95 % CI = −1.13 to −0.27, p = 0.001), especially with Roux-en-Y reconstruction (WMD = −1.0, 95 % CI = −1.52 to −0.48, p = 0.0002) and prolonged time to starting oral diet (WMD = 0.52, 95 % CI = 0.13 to 0.90, p = 0.009) in the patients with subtotal gastrectomy. Routine ND appears to be unnecessary after gastrectomy for gastric cancer, irrespective of the extent of resection, and the type of digestive reconstruction.





Similar content being viewed by others


References
Pacelli F, Rosa F, Marrelli D, Morgagni P, Framarini M, Cristadoro L, Pedrazzani C, Casadei R, Cozzaglio L, Covino M, Donini A, Roviello F, de Manzoni G, Doglietto GB. Naso-gastric or naso-jejunal decompression after partial distal gastrectomy for gastric cancer. Final results of a multicenter prospective randomized trial. Gastric Cancer : Official Journal of the International Gastric Cancer Association and the Japanese Gastric Cancer Association 2013 [doi: 10.1007/s10120-013-0319-x]
Yang Z, Zheng Q, Wang Z. Meta-analysis of the need for nasogastric or nasojejunal decompression after gastrectomy for gastric cancer. The British Journal of Surgery 2008; 95(7): 809–816 [doi: 10.1002/bjs.6198]
Li C, Mei JW, Yan M, Chen MM, Yao XX, Yang QM, Zhou R, Zhu ZG. Nasogastric decompression for radical gastrectomy for gastric cancer: a prospective randomized controlled study. Digestive Surgery 2011; 28(3): 167–172 [doi: 10.1159/000323744]
Tavassoli A, Rajabi MT, Abdollahi A, Bagheri R, Noorshafiee S. Efficacy and necessity of nasojejunal tube after gastrectomy. International Journal of Surgery 2011; 9(3): 233–236 [doi: 10.1016/j.ijsu.2010.11.017]
Cheatham ML, Chapman WC, Key SP, Sawyers JL. A meta-analysis of selective versus routine nasogastric decompression after elective laparotomy. Ann Surg 1995; 221(5): 469–476; discussion 476–468.
Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ (Clinical research ed) 2011; 343: d5928 [doi: 10.1136/bmj.d5928]
Sutton AJ, Abrams KR, Jones DR, Jones DR, Sheldon TA, Song F. Methods for meta-analysis in medical research: J. Wiley, 2000
Wu CC, Hwang C, Liu T. There is no need for nasogastric decompression after partial gastrectomy with extensive lymphadenectomy. Eur J Surg 1994; 160(6–7): 369–373.
Hak YC, Ho SB, Kon HW, Kil PW. Nasogastric decompression is not necessary in operations for gastric cancer prospective randomised trial. Eur J Surg 2002; 168(7): 379–383
Lee JH, Hyung WJ, Noh SH. Comparison of gastric cancer surgery with versus without nasogastric decompression. Yonsei Med J 2002; 43(4): 451–456
Doglietto GB, Papa V, Tortorelli AP, Bossola M, Covino M, Pacelli F, Group ITGS. Nasojejunal tube placement after total gastrectomy a multicenter prospective randomized trial. Arch Surg 2004; 139(12): 1309–1313; discussion 1313
Hsu SD, Yu JC, Chen TW, Chou SJ, Hsieh HF, Chan DC. Role of Nasogastric Tube Insertion after Gastrectomy. Chirurgische Gastroenterologie 2007; 23(3): 303–306 [doi: 10.1159/000105624]
Katai H. Function-preserving surgery for gastric cancer. International Journal of Clinical Oncology 2006; 11(5): 357–366
Hölscher AH, Vallböhmer D, Brabender J. The prevention and management of perioperative complications. Best Practice & Research Clinical Gastroenterology 2006; 20(5): 907–923
McAlister FA, Bertsch K, Man J, Bradley J, Jacka M. Incidence of and risk factors for pulmonary complications after nonthoracic surgery. American Journal of Respiratory and Critical Care Medicine 2005; 171(5): 514–517
Mattei P, Rombeau JL. Review of the pathophysiology and management of postoperative ileus. World Journal of Surgery 2006; 30(8): 1382–1391
Suehiro T, Matsumata T, Shikada Y, Sugimachi K. Accelerated rehabilitation with early postoperative oral feeding following gastrectomy. Hepato-Gastroenterology 2003; 51(60): 1852–1855
Hur H, Kim SG, Shim JH, Song KY, Kim W, Park CH, Jeon HM. Effect of early oral feeding after gastric cancer surgery: a result of randomized clinical trial. Surgery 2011; 149(4): 561–568
Balk EM, Bonis PA, Moskowitz H, Schmid CH, Ioannidis JP, Wang C, Lau J. Correlation of quality measures with estimates of treatment effect in meta-analyses of randomized controlled trials. Jama 2002; 287(22): 2973–2982
Acknowledgments
This work was supported by The National Key Technology R&D Program (no.2013BAI05B00), the Major Program of Science and Technology Program of Guangzhou (no.201300000087), Research Fund of Public welfare in Health Industry of Health (No.201402015), Ministry of Health of PR China, and the program of the national key clinical medical specialty
Conflict of Interest
None declared.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Da Wang and Tingting Li contributed equally to this work.
Hao Liu and Guoxin Li also contributed equally and should be considered as co-corresponding author.
Rights and permissions
About this article

Cite this article
Wang, D., Li, T., Yu, J. et al. Is Nasogastric or Nasojejunal Decompression Necessary Following Gastrectomy for Gastric Cancer? A Systematic Review and Meta-Analysis of Randomised Controlled Trials. J Gastrointest Surg 19, 195–204 (2015). https://doi.org/10.1007/s11605-014-2648-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-014-2648-4