
Abstract
Background
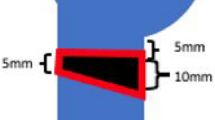
The management of the subcapital fracture of the fifth metacarpal bone, the boxer's fracture, is still a matter of debate. Besides the question of which rate of angulation is acceptable before a reduction becomes necessary, recommendations for further treatment of this fracture vary as well. Therefore, the aim of our study was to compare randomly and prospectively the results of an immobilization treatment for 3 weeks with cast with a functional treatment, all with accepted angulations up to 70°.
Patients and methods
Between June 1997 and June 1998, 40 patients were randomly allocated either to treatment with an ulnar gutter plaster cast for a period of 3 weeks followed by mobilization, or a pressure bandage for 1 week and immediate mobilization within limits imposed by pain. All patients were monitored at the outpatient clinic 6 and 12 weeks after the fracture. Clinical outcome was measured by the range of motion (ROM) of the fifth metacarpal phalangeal (MCP) joint, and by interviewing the patients about their satisfaction, pain perception, return to work and hobby, and need for physiotherapy.
Results
A total of 35 patients with a mean age of 29 years (range 15–84) completed the required follow-up program. The mean angulation of the fracture was 39° (range 15–70°). Between the two groups, no statistical differences were scored with respect to ROM, satisfaction, pain perception, return to work and hobby, and need for physiotherapy. According to a sample size calculation (power 90%, alpha 0.05, to detect 5° difference in ROM), 12 patients needed to be included in each group to reach significance.
Conclusions
A pressure bandage for 1 week, followed by immediate mobilization, is a sufficient alternative treatment for a boxer's fracture, if it is not angulated greater than 70° and not rotated. This treatment resulted in satisfied patients who perceived no more pain and had a good ROM of the fifth MCP joint. Reduction of angulated fractures of less than 70° seems not of value, with respect to ROM of the fifth MCP joint.
Similar content being viewed by others


References
Ali A, Hamman J, Mass DP (1999)The biomechanical effects of angulated boxer's fractures. J Hand Surg 24A:835–44
Birndorf MS, Daley R, Greenwald DP (1997) Metacarpal fracture angulation decreases flexor mechanical efficiency in human hands. Plast Reconstr Surg 99:1079–83
Braakman M, Oderwald EE, Haentjens HHJ (1998) Functional taping of fractures of the 5th metacarpal results in a quicker recovery. Injury 29:5–9
Breddam M, Hansen TB (1995) Subcapital fractures of the fourth and fifth metacarpals treated without splinting and reposition. Scand J Plast Reconstr Hand Surg 29:269–70
Calder JDF, O'Leary S, Evans SC (2000) Antegrade intramedullary fixation of displaced fifth metacarpal fractures. Injury, Int J Care Injured 31:47–50
Ford DJ, Ali MS, Steel WM (1989) Fractures of the fifth metacarpal neck: is reduction or immobilisation necessary? J Hand Surg 14B:165–7
Freeland AE, Geissler WB, Weiss A-PC (2001) Operative treatment of common displaced and unstable fractures of the hand. J Bone Joint Surg Am 83:928–945
Holst-Nielsen F (1976) Subcapital fractures of the four ulnar metacarpal bones. The Hand 8:290–3
Hunter JM, Cowen NJ (1970) Fifth metacarpal fractures in a compensation clinic population. J Bone Joint Surg 52A:1159–65
Konradsen L, Nielsen PT, Albrecht-Beste E (1990) Functional treatment of metacarpal fractures. Acta Orthop Scand 61:531–4
Kuokkanen HOM, Mulari-Keränen SK, Niskanen RO, Haapala JK, Korkala OL (1999) Treatment of subcapital fractures of the fifth metacarpal bone: a prospective randomised comparison between functional treatment and reposition and splinting. Scand J Plast Reconstr Hand Surg 33:315–7
Lowdon IMR (1986) Fractures of the metacarpal neck of the little finger. Injury 17:189–92
McKerrell J, Bowen V, Johnston G, Zondervan J (1987) Boxer's fractures-conservative or operative management? J Trauma 27:486–90
Porter ML, Hodgkinson JP, Hirst P, Wharton MR, Cunliffe M (1988) The boxer's fracture: a prospective study of functional recovery. Arch Emerg Med 5:212–15
Sørensen JS, Freund KG, Kejlå G (1993) Functional fracture bracing in metacarpal fractures: the Galvestone metacarpal brace versus a plaster-of-Paris bandage in a prospective study. J Hand Ther 6:263–5
Theeuwen GAJM, Lemmens JAM, van Niekerk JLM (1991) Conservative treatment of boxer's fracture: a retrospective analysis. Injury 22:394–6
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Muller, M.G.S., Poolman, R.W., van Hoogstraten, M.J. et al. Immediate mobilization gives good results in boxer's fractures with volar angulation up to 70 degrees: a prospective randomized trial comparing immediate mobilization with cast immobilization. Arch Orthop Trauma Surg 123, 534–537 (2003). https://doi.org/10.1007/s00402-003-0580-2
Received:
Revised:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-003-0580-2