
Abstract
Breast cancer is a reality for 5000 women in Switzerland every year and, when these women are in a committed relationship, represents a critical event for their partners as well. For this reason, there is now a consensus in the literature to consider breast cancer as an event involving couples as much as women alone. Research should also take into account women and partners and should be extended to couples as a unit. Up to now, it has been difficult to draw a synthesis from the data available in the body of writings on the impact of cancer on couples, as methodologies have been diverse and vary between studies. Thus, the goal of this chapter is first of all to present the advantages and limitations of the two main methods of assessment that are used in the domain of couple relationships: questionnaires and observation. The necessity to combine the different methods is then discussed. At last, comments will be illustrated with a project conducted in Switzerland funded by the Swiss National Science Foundation that formed part of the National Centre of Competence in Research (NCCR) “LIVES – Overcoming Vulnerability: Life Course Perspectives” and which examined couples facing breast cancer using a mixed method approach.
The original version of this chapter was revised. An erratum to this chapter can be found at https://doi.org/10.1007/978-3-319-24157-9_11
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
- Overcoming Vulnerability
- National Center Of Competence In Research (NCCR)
- Coupling Relationship
- Dyadic Coping Inventory
- Healthy Partner
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Breast cancer is a reality for 5000 women in Switzerland every year (Ligue Suisse contre le Cancer 2005). This form of cancer is the most prevalent one among women (one woman out of eight will present a breast cancer) and represents the principal cause of mortality among women under 60. Consequences of the disease are not restricted to somatic health; facing diagnosis and medical treatment represents a source of severe stress with a possible impact on social and emotional functioning (Manne et al. 2004). Women have to cope with somatic symptoms (pains, loss of appetite, nausea, tiredness, for example) and emotional consequences (anxiety, depression, anger, helplessness, for example), difficulties related to their body image and sexual identity, and with the uncertainty about the prognosis as well as their marital and familial future (Zimmermann and Heinrichs 2008). Breast cancer may thus be considered as a critical life event. Moreover, it is associated with chronic strain (worries, long-term treatment) and daily hassles: daily life has to be partly reorganized to allow the women to follow their medical treatment, so that couple, family and work relationships are affected.
When women are married or in a committed relationship, breast cancer represents a critical event for their partners as well. Some of them report high level of physical and psychological distress, which can be even higher than the level of distress reported by women. Partners worry because they do not know whether the women will survive the disease. Moreover, they fear the consequences of their partners dying from the illness, such as loneliness (Kayser and Scott 2008; Northouse 1989). In addition, breast cancer specifically affects the couple relationship as it concerns a body part intimately related to sexual activity. For these reasons, there is now a consensus in the literature to consider breast cancer as an event involving couples as much as women alone.
1.1 The Couple Relationship as the Primary Resource of Social Support
Implications for the couple relationship can be seen from the woman’s perspective. One way to cope with the stress related to the illness is indeed to receive support from significant others, especially from the partner (Ell et al. 1989; Manne et al. 2004; Pistrang and Barker 1995). Social support plays an important role in one’s life at two inter-related levels (Cutrona 1996; Weiss 1974). First, at a general level, it allows the fulfillment of interpersonal needs in everyday life. In this perspective, social support is an ongoing resource that increases well-being and acts as a resiliency factor that lowers the probability that daily life events will be perceived as stressors by the individual. Second, at a more specific level, social support refers to the assistance that an individual receives during times of adversity when she has to face and cope with a critical event. In this perspective, social support is conceptualized as a moderator factor which influences the link between a critical event and an individual’s health. In case of a somatic illness like cancer, support is sought especially from the partner (Ell et al. 1989; Manne et al. 2004; Pistrang and Barker 1995). Three types of supportive social interactions have been traditionally distinguished: emotional, instrumental and informational. The first one is of primary importance in stress situations: it refers to reassurance and love needs that a person will have when facing a challenging situation. In the case of a breast cancer, this is usually the first need women report that they expect from their partner. The second one refers to pragmatic help, like money or assistance in the realization of daily tasks. Women expect this kind of help both from their partners (daily shopping, household chores) and from the larger social circle or even from institutions (having money for the medical treatment). The latter refers to advice or information which is mainly expected from medical staff. Women’s satisfaction with the social support they receive from their partners is an important predictor of the enhancement of their mood and quality of life (Giese-Davis et al. 2000; Helgeson and Cohen 1996). Moreover, women’s perception of her partner as highly supportive predicts a better adjustment to the stress of the illness as it plays a buffering role against comorbid disorders such as depression or anxiety (Manne et al. 1999), and helps to maintain a good quality of life which is in turn predictive of better outcomes (e.g. more chances to get back into work after treatment) (Northouse et al. 2002; Schulz and Schwarzer 2004).
On their side, partners are in the difficult situation in which they have to manage a “double agenda”: on the one hand, they have to cope with their own stress and on the other hand they have to be supportive to their wife (Zimmermann et al. 2007). When they face the distress of their wife, they report feeling helpless and often not knowing how to provide an adequate support (Zimmermann and Heinrichs 2006). Some of them lack the necessary resources, as they may be overwhelmed by the stress and consequently display inadequate social support: for example, emotional withdrawal, criticism, minimization of the effects of the disease, lack of empathy, avoidance of discussion related to cancer (Pistrang and Barker 1995; Wortman and Dunkel-Schetter 1987). Most of the time, partners do not receive support from the medical staff because attention is primarily given to the woman; existing psychosocial interventions are also mainly addressed to the woman, or to the couple as an “entity” but rarely to the partner him(her)self – when it is the case, it is most often to enhance their skills to help their wives (see for example Manne and Ostroff 2008). Data are indeed scarce about the way partners manage their own stress.
The importance of the help partners give to each other when facing an aversive event has been underscored by theoretical and empirical data about stress and coping. Bodenmann (2005) has coined the term “dyadic coping” to put the emphasis on the way partners communicate their needs to one another and how they respond to the others’ needs. Dyadic coping is supposed to be implemented when individual coping is not efficient to regulate emotions associated with a stress situation; this is in essence a reciprocal process, which means that the help one partner may provide to the other depends to a certain extent on the help she or he will receive. A comprehensive study should then take into account not only the woman needs, but also the partners’ needs, how both get connected and what are the reciprocal behaviors they use to communicate their needs and their support to each other.
However, social support is not only a matter of what someone “does” for someone else, but also a matter of what the recipient of the help will perceive as such. The literature in the domain of social support has shown that there is a difference between the received social support (the “objective” social support) and the perceived social support (the “subjective” social support). Perception of social support depends on several factors such as personality or psychological states; depression may for example make a person unable to perceive the help she receives as her vision of the world is negative, by definition. On the contrary, an “optimistic” person may over-evaluate the help she receives (Cutrona 1996; Cutrona and Suhr 1992; Schwarzer and Leppin 1989).
1.2 Methodological Challenges
Studying social support in couples implies several methodological challenges. In order to have a comprehensive picture of the couple facing a stressful event, it is necessary to draw on the one hand on “objective” data, i.e. what the person receives, and on the other hand on “subjective” data, i.e. the perception the person has about received support. Getting objective data has two implications: first, several sources of information have to be solicited; second, at least one of these sources has to be an “external informant”, that means a third person who evaluates the relationship between the partners. To date, social support in the domain of women breast cancer has been measured mainly by self-reported questionnaires completed by the women and, much more rarely, by their partners – the behavior of their partners is thus most often reported by the women themselves. Second, while a lot of attention has been given to the effect of the different types of social support (emotional, instrumental, informational) and to the effect of individual variables like coping strategies in women on adjustment to the stress of the illness, much less is known about the mechanisms though which social support is communicated and perceived in couples. It is difficult to draw a synthesis from the data available in the literature, as methodologies have been diverse and vary between studies. For example, Gerits (2000) found contradictory findings between studies using different assessment methods in the domain of breast cancer. He reported that studies using questionnaires did not find a link between coping strategies in women and disease outcomes, while studies measuring these variables by interviewing the women did find significant links between these variables.
2 Objectives of the Chapter
The goal of this chapter is to present the advantages and limitations of the two main methods of assessment that are used in the domain of couple relationships: questionnaires and observation. The necessity to combine the different methods is discussed. Comments will be illustrated with a project conducted in Switzerland funded by the Swiss National Science Foundation that formed part of the National Centre of Competence in Research (NCCR) “LIVES – Overcoming Vulnerability: Life Course Perspectives”. This project examined couples facing breast cancer using a mixed method approach. Indeed the studies reported above have shown that women do not cope alone with their illness, but within their marital relationship, and that mutual social support between partners has an impact on the patient’s as well as partner’s adjustment (Kayser 2005). It is of primary importance to gain and refine knowledge about the way each partner copes with the disease and the social support they provide one another, in order to help them to avoid inadequate adjustment to the illness and to identify variables which may be used to set up psychosocial and psychological interventions. Although it is known that interventions addressed to the patients or couples facilitate social support within the interactional relationship, several questions are left unanswered (Kayser 2005), such as: What kind of interventions should be delivered? What is the more relevant between an individual (woman and partner separately) or a couple-based intervention in a given situation? At what point during the illness and treatment would the intervention be most helpful for each partner?
3 Considerations About the Different Assessment Methods
The two main methods of questionnaires and observation have both advantages and limitations that we present below.
3.1 Questionnaires
Questionnaires make it possible to obtain self-reported data (a person assesses his/her own thoughts, emotions, behaviors, relations to other people) or hetero-reported data (a person evaluates another person’s thoughts, emotions, behaviors, relations to other people). Hetero-reported data can be obtained by participants of a study (for example: husbands evaluate their wife’s behaviors) or by external judges (for example: questionnaires are filled in by researchers or practitioners) (Favez 2010).
3.1.1 Advantages of Questionnaires
Questionnaires offer the advantages to be quickly completed and easy to use. Furthermore, they make it possible to assess thoughts, emotions, behaviors and relations through different temporal perspectives: a woman could then assess her couple relationship as it was in the past, as it is in the present and how she expects (or hopes) it to be in the future (Favez 2010). Questionnaires mainly make it possible to assess the subjective point of view of the person; as far as social support is concerned, they make it possible thus to assess the perceived support, which is of utmost importance as several studies have pointed out the more important role of perceived social support compared to the received social support by people facing cancer (Uchino 2004).
Furthermore, in the domain of marital relationships, Hahlweg et al. (2000) noted that partners provide additional pieces of information about their relationships’ history and their manner of interacting with each other when they fill in the questionnaires. They have the opportunity to report data which are to a certain extent representative of the “objective” reality of the relationship. Accordingly, Kenny and Acitelli (2001) assumed that motive (willingness to have a good perception of the partner), opportunity (spouses have a lot of occasions to observe their partner) and information (possibility to share with the partner intimate feelings) should lead to accurate data about the partner and the relationship.
3.1.2 Disadvantages of Questionnaires
Questionnaires present however some disadvantages and limitations, one being the possible influence of social desirability on the one hand, or of a lenience effect when assessing the relationship on the other hand. In the domain of couple marital interactions, Murray et al. (1996) explained this phenomenon by talking about a strong idealization effect. According to the theory of Sillars (1985), some individuals could have a biased perception of the social support provided by their partner in order to protect their marital relationship. Indeed, tactfully interpreting the personality or the behaviors of the partner could, in some situations, avoid harming the relationship. Sillars (1985) noted that the familiarity between the partners (impression of knowing the partner), the behavioral interdependence (ways of communicating and interacting between partners that take place over time) and the propensity of the couple relationship to generate strong positive and negative emotions (which could lead to erroneous inferences about the partner’s actions and intentions) could also be a source of biased perception of the partner’s social support. More globally, and not restricted to positive evaluations, answers may be biased by a halo effect. In marital studies, Nye (1988) showed this effect in satisfied partners who attribute a great number of positive traits to their partner and a negative halo effect in unhappily married couples where each partners attribute a lot of negative traits to each other. This effect has also been described as a sentiment override: in short, there is a kind of global judgment about the relationship which causes partners to see the different variables pertaining to the relationship with the same affective valence. Finally, answers to a questionnaire on relationships are also influenced by attribution bias – which is close to the halo effect (Bradbury and Fincham 1990; Jacobson et al. 1985). For example, an inadequate behavior of one partner (a criticism, an accusation, contempt, etc.) is interpreted by the other partner in a happily married couple as an unstable and situational behavior, and an adequate behavior is perceived as stable and internal to the partner. In contrast, in an unhappily married couple, an inadequate behavior is seen as stable and internal to the partner and an adequate one is perceived as unstable and dependent of the situation.
Another limitation lies not in questionnaires themselves, but in the use of a research methodology relying only on questionnaires. There are indeed often high correlations between different questionnaires completed by the same person, when these questionnaires are addressing close concepts. For example, in the domain of marital interactions, high correlations are systematically found between social support perceived and provided by the partners and marital satisfaction (Bodenmann 2000). While these correlations may refer to genuine associations between different variables, they may also stem from an artifact that Gottman has named the “GLOP problem” (Gottman 1998). It refers to the fact that an association between two variables assessed by the same person may be explained by a third “hidden” variable; to continue with the above example, a low marital satisfaction and a low perception of the support provided by the partner may both be the result of a depressed mood in the informant. This artifact is all the more evident when couple relationships are assessed. In this case, the between-informants agreement is significantly lower than within-informants agreement (Rhoades and Stocker 2006). This means that the real degree of similarity between both partners tends to be lower than the degree of similarity reported individually by each partner. For example, a woman facing cancer could give an account of a high level of emotional support provided to and received from her partner, whereas her partner reports that both he and his partner provided one another with a low level of emotional support. In this example, one partner reports a high degree of emotional support in the couple and the other one a low level. The between-informants agreement is thus low. However, the within-reporter agreement is high because each partner perceives a same level of emotional support by him/herself and the partner.
In short, it is thus important to note that researchers have emphasized that questionnaires make it possible to collect subjective data (the informant’s representation) and to a certain extent “objective” data, but they are also subject to biases so that additional methodology is warranted when the researcher is interested in getting an accurate picture of interactional variables. Direct observation of behavior is the usual alternative to questionnaires in studies on interactions.
3.2 Observational Data
Observational data allow the collection of “here and now” information (Favez 2010). This collection can be naturalistic or standardized. Naturalistic observational data are obtained in the participants’ natural environment (at home, for example). Standardized observational data are obtained in a laboratory situation with a task given to the participants. In most cases, technical equipment is used to make a video or audio recording of the behaviors (verbal and/or nonverbal). Trained coders visualize and listen then to the video- or audiotaped sequences and code them using standard coding tools.
3.2.1 Advantages of Observational Data
Observational data allow homogeneity between trained coders using a standardized coding grid, which may be consider as an index of “objectivity”. For example, in the domain of marital interactions, in order to evaluate emotional social support provided by partners, coders firstly have to define and conceptualize the emotional social support (What is it? What are the behavioral indicators of emotional social support? How is emotional social support expressed?). Researchers then have to define the measuring unit: do they want to observe behaviors, for example, a look from a partner to the other one (molecular units) or a chain or group of behaviors that form a construct, for example, consolation (molar units) (Favez 2010). Researchers are then trained to code. This homogeneity cannot be obtained when asking both partners to individually evaluate their own couple relationship.
Moreover, observational data make it possible to take into account interactional sequences – that is, how the couple is functioning in moment-to-moment interactions. For example, in the domain of marital interactions, Margolin and Wampold (1981) showed that distressed partners tend more often to show a “negative reciprocity” than nondistressed couples, i.e. a negative action by one partner (a criticism, for example) is followed by a negative reaction by the other partner and so on. On the other hand, nondistressed couples show a tendency for a partner to react positively (with humor, for example) to a negative action of the other; this is absent in distressed couples, and has been labeled as “negative reactivity”. In a similar vein, observational data has highlighted some communication patterns such as the demand-withdraw pattern (Christensen and Schenk 1991). This pattern is characterized in marital relationships by the motivation of one partner (usually the wife) to discuss some issues and to solve problems, and by the efforts of the other partner (usually the husband) to avoid the discussion and to withdraw from the interaction.
Furthermore, observational data make it possible to analyze whether the answer provided by one partner is optimally matched with the needs and demands of the other one (Cutrona and Russell 1990). For example, a woman facing cancer is afraid of the disease and feels the need to share these concerns with her partner, to be heard by him, to be reassured by being taken in his arms and so on. This woman needs some emotional social support from her partner. The partner responds to her demand by suggesting to phone to her doctor in order to have some information about the disease. He gives her instrumental social support. Although the support provided by the partner is theoretically positive, it is not adapted to the specific woman's need at this very moment; consequently it is evaluated by the patient as inadequate and ineffective.
Finally, observational data allow the detection of possible incongruences between messages emitted by different communication channels. Nonverbal and paraverbal communication play an important role in the way social support between partners is perceived. If one partner gives positive verbal social support to the other one (“I will be with you in order to face the cancer”), but pronounces this sentence, for example, with anger (paraverbal) or without looking at his partner (nonverbal), the woman will perceive the social support as negative.
3.2.2 Hesitations and Arguments for the Use of Observational Data in the Domain of Couple Interactions
Several questions regarding observational methods have been under debate, especially concerning laboratory observation. The first one is about representativeness of the data: is it possible to get information about how the couple does in “real” life when they are asked to interact in an artificial setting with cameras around them? Studies show that couples indeed behave differently in laboratories and at home without the presence of an observer. When they are under observation, partners are kinder to each other than when they are at home alone and they engage in far shorter chains of negativity (Gottman 1979), but if high negative emotions are present between them they tend nevertheless to show up after a while. Gottman (1994) demonstrated that couples could simulate adequate communication during maximum the first 2 min of an interaction and then they fall in their typical communication patterns. Vincent et al. (1979) ultimately asked the couples to try either to fake good or fake bad in the lab during 10 min. Both groups of couples were unable to fake their nonverbal behaviors. Nonverbal behavior may be a better discriminator of distressed and nondistressed groups than verbal behavior alone. Heyman (2001) summarized that, even if interactions of distressed couples observed in a laboratory are not as negative as interactions filmed at home, some “differences in affect, behavior, physiology, and interactional patterns and processes” could be revealed. In general, observational data may generate “false negatives” (some couples may be able to “hide” their negative feelings), so it is possible that partners interact in a more adequate way in the laboratory than they do at home and researchers might overlook conflicts in the marital interactions. By contrast, “false positives” are very unlikely to be found (when negative emotions are displayed in the laboratory, they are representative of the objective state of the relation). All in all, this tends to show that observational data collected in a laboratory can be representative of everyday interactions, especially for couples with a high level of conflict and negative emotions.
Another question concerns the possible selection bias as there might be a difference between people who agree to be filmed and observed in the lab and people who do not. Data are scarce in this domain. In one research, Krokoff et al. (1988) did not find differences between couples who volunteered to participate in the videotaped sequences and couples who were randomly assigned to participate in these sequences.
Finally, there might be concerns about the consequences for people of participating in laboratory observations, especially in procedures in which couples are asked to talk about conflict issues, with the possible risk that the negative emotions elicited in the laboratory may spread into their everyday life. Here also, data are scarce; in one research, Fichten and Wright (1983) did not find any negative effects for couples participating in observational studies. Indeed these authors videotaped couples’ interactions in a laboratory. Six months later, the level of marital satisfaction reported by the couples was the same as the level reported at the time of the observation. Moreover, almost half of these couples reported an improvement of their marital satisfaction due to participating in the study. As far as couples facing cancer are concerned, we hypothesized that taking part in a situation of observation could also have benefits for both partners. Indeed being in a lab could facilitate talking about the disease between partners and mobilize individual resources of both partners and couples’ resources.
3.2.3 Disadvantages of Observational Data
Hahlweg and collaborators (2000) remind us that the collection of observational data in the domain of marital interactions is “costly and time consuming, particularly for microanalytic coding systems that require the accurate classification of small units of behavior” (p. 61). These authors describe the typical process in order to obtain valid data. The couples have first to come to the laboratory and be videotaped during a discussion. Several external observers have to be trained in order to code the interactions with a standard grid. These coders are regularly supervised and the inter-rater validity has repeatedly to be probed. In consequence, observational data requires important resources.
4 The Necessity to Mix the Methods
So, what is the best methodology in studying social support in couples? Should we choose between the two? The first thing to consider is the extent to which information brought by these methods is redundant or complementary. In the domain of marital interactions, moderate correlations are found between questionnaires and observational data. For example, Hahlweg et al. (2000) computed associations between conflict patterns reported by partners – self-reported data based on the Communication Patterns Questionnaire (CPQ; Heavey et al. 1996) – and conflict patterns rated by external observers – observational data that relied on the Coding System for Marital/Family Interaction (KPI; Hahlweg et al. 1984) – in a nonreferred sample group. They only found moderate correlations between the results of the two instruments. In general, there are consistently low to moderate associations between questionnaires and observation, even when the instruments are designed to assess the same psychological construct.
Based on the fact that questionnaires provide access to the representations of each partner and that observational data allow the observation of verbal, nonverbal and paraverbal interactions between both partners, it is now relatively well accepted that the information is complementary and that the best strategy is to use both when possible. This is all the more relevant as the results obtained by these methods may highlight discrepancies which are clinically informative. For example in studies examining social support among couples facing breast cancer, the healthy partner may seem very supportive during the video sequences, but appears rather contemptuous in the data collected by questionnaires. These discrepancies may be due to the healthy partner’s personality (for example: a passive-aggressive personality), or to the healthy partner’s willingness to preserve the other partner and the couple interaction and not show his partner any discouragement. In contrast, the healthy partner may report good evaluations of his own social support in questionnaires, but appear to be inadequate during the audio- or videotaped interactions. This phenomenon could appear when the healthy partner tries to answer in a socially desirable way (it is easier to guess the expected answers by filling in questionnaires that by participating in a videotaped interaction) or when the healthy partner is not aware of his behavior.
This low to moderate association may also be due to stereotypes. For example, Neff and Karney (2005) highlight the fact that in studies relying on self-reported data both spouses tended to report a better social support provided by the women than by the men. In contrast to this, gender differences were not reported in studies using observational data.
5 The Study “Women Facing Breast Cancer” of the LIVES NCCR
In order to overcome the artifacts produced by the use of different assessment methods, the study “Women facing cancer” uses a mixed-method approach as mentioned above. We present now the details of this study.
5.1 Method
5.1.1 Sample
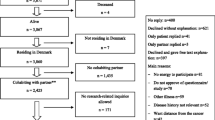
Eighty-nine women with breast cancer were recruited at the Breast Centre of the University Hospital of Lausanne (Switzerland). Sixty were in a relationship (their partners also participated in the study) and 29 were single. The mean age for women in relationships was 54.70 (SD = 12.55) and 55.59 (SD = 12.66) for single women; partners were on average 56.21 years old (SD = 14.75). 60 % of the women in relationship were married. 65.5 % of single women were divorced or separated, 17.2 % were widows, and 17.2 % were single (i.e. never married).
5.1.2 Procedure
Women were informed of the study by the breast nurse during their hospitalization (1–2 weeks after the diagnosis). Criteria for study inclusion were as follows: (a) the patient had a diagnosis of breast cancer; (b) the patient had had breast cancer surgery; (c) the patient and partner were 18 years of age or older; (d) the patient and partner were French speaking. Eighty-nine women accepted to participate (58 %) and 65 women refused (42 %). The principal reasons for refusal were the following: no desire to be filmed (32 %), a lot of stress and a lack of energy (26 %), no desire to talk about these difficult moments (29 %), and various other reasons (13 %). Comparisons were made between study participants and nonparticipants. Results indicated no significant differences in terms of age, t(152) = 0.05, ns nor in terms of relationship status (in couple or single), χ2(1, 154) = 0.01, ns. Women and their partners were received around 2 weeks after the surgery for an interview with the breast nurse, a situation of observation and to fill in questionnaires (T1). Follow ups were planned to take place 3 months (T2), 12 months (T3) and 24 months (T4) after the surgery.
5.1.3 Questionnaires
Questionnaires were used in order to assess several individual and relational variables by both partners, such as general distress (Brief Symptoms Inventory-18; Derogatis 2001), marital satisfaction (Relationship Assessment Scale; Hendrick 1988) or social support in couple interactions (Dyadic Coping Inventory; Bodenmann 2008). These questionnaires were paper self-completion questionnaires. The study also contained hetero-reported data such as the evaluation by both partners of the other one’s social support (Dyadic Coping Inventory, Bodenmann 2008) or cancer- related communication (Cancer-related Communication Problems within Couples Scale, Kornblith et al. 2006). Questionnaires were constituted of Likert-scales. Each partner individually filled in the questionnaire at home and returned it by mail to the Breast Center using the prepaid envelope. Finally, questionnaires about medical information, such as diagnosis, complications, and treatment were administered by the breast nurse.
One of the questionnaires, the Family Attitude Scale (FAS; Kavanagh et al. 1997; French version Vandeleur et al. 2013), aimed at assessing “expressed emotions”. This is one of the constructs that has been studied through observations and self-reports and thus it may illustrate the complementary information brought by these two methods. Expressed emotions refer to the degree of criticism and hostility and emotional over-involvement in a family or a marital relationship (Brown and Rutter 1966). High Expressed Emotion (HEE) is defined when one partner makes a lot of negative comments about the other one and the couple relationship and Low Expressed Emotion (LEE) describes a low rate of such comments. Expressed emotions are known to be a significant predictor of negative psychological outcomes (Butzlaff and Hooley 1998; Lister 2011), high level of partner caregiver burden (Möller-Leimkühler and Jandl 2011) and relationship dissatisfaction (Kronmüller et al. 2011) across several diseases. The FAS is a 30-item questionnaire assessing the informant’s expressed emotions through self-reported attitudes and behaviors towards another person – in our case, the partner. Items are rated on Likert scales from 4 (every day) to 0 (never), except for positive attitudes and behaviors which are reverse scored. The total score has a range of 0–120, with higher scores reflecting high expressed emotions. Examples of questions are: “I find myself saying nasty or sarcastic things to him/her”, “He/she is easy to get along with”, “I am sick of having to look after him/her”. In our study, women obtained a mean score of 21.4 (SD = 14.6; median = 19; range = 1–76); partners got a mean score of 14.6 (SD = 9.2; median = 14; range = 0–35).
5.2 Observational Data
Two kinds of observational data were collected by the breast nurse in the lab of the Breast Centre of the University Hospital of Lausanne. Firstly, a semi-standardized interview aimed at collecting information from both partners about the way they reacted to the diagnosis, the sense they gave to the illness, how they informed (if they have) their families and friends, how they have been managing the illness, how the relationship has been affected at an emotional as well at a sexual level, how they have been supporting each other and where they could find support outside their relationship, how they see their future. The partners were invited to answer freely to these questions. The interview was videotaped. Two researchers coded the verbal, paraverbal and nonverbal contents of the interview with standardized coding grids for social support or for diagnosis integration. Inter-rater reliability was assessed in order to warrant the validity of the data.
Secondly, each partner was invited to complete a standardized task aimed at evaluating “live” expressed emotion: the Five Minute Speech Sample (FMSS; Magana et al. 1986). This task consists in a monologue by each partner who is asked to talk about his/her partner and their couple relationship during 5 min. The speech is audiotaped and the verbal and paraverbal content is coded for expressed emotions with a standardized coding grid provided by the authors (Magana et al. 1986). An expert in this coding system trained three coders. In order to establish interobserver reliability, the coders rated 15 videotapes (that means 30 FMSS-sequences) independently. Cohen’s kappa coefficients were then computed. For the different coded categories (e.g.: critics, quality of the relationship, etc.), the coefficients were higher than 0.80 between each coder and the expert and higher than 0.80 among the coders.
5.3 Observed and Self-Reported Expressed Emotions; A Case Example
The woman is 70 and the man 74 years old. The partners have known each other for 52 years and have been married for 51 years. They have two children of 51 and 48 years old. They filled in the questionnaires and participated in the FMSS 2 weeks after the surgery (6 weeks after the woman received a diagnosis of breast cancer).
The woman obtained a score of 40 on the FAS. This score is high compared to the mean score of the sample (larger than one standard deviation above the mean). For example, she gave high scores to items such as “He makes me feel drained” and “He ignores my advice”. In the FMSS, this woman made mainly positive comments about her husband (“He is just and right”, “He is gentle and kind, he is very sensitive”) and her happiness to be in a marital relationship with him (“We are always on the same wavelength”, “I am happy [with him]”, “I am lucky [with him]”, “I can count on him”, “We are well together”, “I will never change [my partner]”).
The man obtained a score of 21 at the FAS. This score is average with regard to the sample of the current study (within one standard deviation above the mean). He displayed zero score on some items like: “She is really hard to take”, “I feel disappointed with her”. By contrast, in the FMSS, he displayed a very high expressed emotions pattern with several criticisms toward his partner; the monologue began with the sentence: “She was a girl I knew among others. I was taken by surprise, so my father told me that I made a mistake that I will pay to the bitter end. I didn’t know her. I quickly saw that I could manipulate her, that I could rule her with a rod of iron.” The husband gave next some criticisms: “She is quite impulsive. Her brother says she is unreliable. She sometimes deserves ….[silent, sigh], she freaks out.”
This example illustrates the necessity to assess this construct with several methods as the results are not the same depending on the method that was used: according to the questionnaire, the woman was high on expressed emotion while the man was low; according to the situation of observation, the woman was low on expressed emotions and the man was high. This certainly refers to a certain degree of ambivalence in their relationship; the mixed-method approach allowed us to note that both partners are ambivalent while a single method would have led us to conclude that one partner only is high on emotion and thus “responsible” for the negativity in the relation. Moreover, we would not have identified the same partner as the “negative one” depending on the chosen method. The mixed method also allows a more complex and comprehensive evaluation of a situation. In fact, each method measures a different aspect of this situation and grasps its nuances and subtleties.
6 Conclusion
A mixed-method approach is crucial in order to study couple interactions in general and interactions in couples facing cancer in particular. It makes it possible to combine data representative of the “subjective reality” of the partners (i.e. the representations they have of the relationship) and of the “objective reality” (how they actually act when they talk about each other or when they interact together). Unfortunately, observation is often overlooked in research mainly because of its cost and the difficulty to operationalize psychological constructs in behavioral indexes (Weiss and Heyman 2004). Gottman (1994) has nevertheless made a plea for observation, arguing that observational data have a special place for two reasons:
-
1.
Partners are not aware of the different patterns of communication and behaviors that usually occur in their couple interaction. It is also difficult for them to accurately report behavioral interactions.
-
2.
Self-reported data assess perceptions, in other words the subjective reality of an individual. Observational data allow researchers to avoid the confusion between perceptions and reality.
Even if observational data require time and energy (i) to obtain videotaped sequences, (ii) to elaborate a coding system and (iii) to code the sequences, this chapter shows that this effort is worthwhile.
References
Bodenmann, G. (2000). Stress und Coping bei Paaren. Göttingen: Hogrefe.
Bodenmann, G. (2005). Dyadic coping and its significance for marital functioning. In T. A. Revenson, K. Kayser, & G. Bodenmann (Eds.), Couples coping with stress: Emerging perspectives on dyadic coping (pp. 33–50). Washington, DC: American Psychological Association.
Bodenmann, G. (2008). Dyadisches Coping Inventar (DCI). Test manual. Bern: Huber.
Bradbury, T. N., & Fincham, F. D. (1990). Attributions in marriage: Review and critique. Psychological Bulletin, 107, 3–33.
Brown, G., & Rutter, M. (1966). The measurement of family activities and relationships. A methodological study. Human Relations, 19(3), 241–263.
Butzlaff, R. L., & Hooley, J. M. (1998). Expressed emotion and psychiatric relapse. Archives of General Psychiatry, 55, 547–552.
Christensen, A., & Schenk, J. L. (1991). Communication, conflict, and psychological distance in nondistressed, clinic, and divorcing couples. Journal of Consulting and Clinical Psychology, 59, 458–463.
Cutrona, C. E. (1996). Social support in couples. Thousand Oaks: Sage.
Cutrona, C. E., & Russell, D. W. (1990). Type of social support and specific stress: Toward a theory of optimal matching. In B. R. Sarason, I. G. Sarason, & G. R. Gregory (Eds.), Social support: An interactional view (pp. 319–366). Oxford: Wiley.
Cutrona, C. E., & Suhr, J. A. (1992). Controllability of stressful events and satisfaction with spouse support behaviors. Communication Research, 19, 154–176.
Derogatis, L. R. (2001). Brief Symptom Inventory (BSI)-18. Administration, scoring and procédures manual. Minneapolis: NCS Pearson, Inc.
Ell, K., Nishimoto, R., Morway, T., Mantell, J., & Hamovitch, M. (1989). A longitudinal analysis of psychological adaptation among survivors of cancer. Cancer, 63, 406–413.
Favez, N. (2010). L’examen clinique de la famille. Modèles et instruments d’évaluation. Wavre: Mardaga.
Fichten, C. S., & Wright, J. (1983). Problem-solving skills in happy and distressed couples: Effects of videotape and verbal feedback. Journal of Clinical Psychology, 39, 340–352.
Gerits, P. (2000). Life events, coping and breast cancer: State of the art. Biomedecine and Parmacotherapy, 54, 229–233.
Giese-Davis, J., Hermanson, K., Koopman, C., Weibel, D., & Spiegel, D. (2000). Quality of couples’ relationship and adjustment to metastatic breast cancer. Journal of Family Psychology, 14, 251–266.
Gottman, J. M. (1979). Marital interaction: Experimental investigations. New York: Academic.
Gottman, J. M. (1994). What predicts divorce: The relationship between marital processes and marital outcomes. Hillsdale: Lawrence Erlbaum Associates, Inc.
Gottman, J. M. (1998). Psychology and the study of marital processes. Annual Review of Psychology, 49, 169–197.
Hahlweg, K., Reisner, L., Kohli, G., Vollmer, M., Schindler, L., & Revenstorf, D. (1984). Development and validity of a new system to analyze interpersonal communication: Kategoriensystem für partnerschaftliche Interaktion KPI. In K. Hahlweg & N. S. Jacobson (Eds.), Marital interaction: Analysis and modification (pp. 182–198). New York: Guilford Press.
Hahlweg, K., Kaiser, A., Christensen, A., Fehm-Wolfsdorf, G., & Groth, T. (2000). Self-report and observational assessment of couples’ conflict: The concordance between the communication patterns questionnaire and the KPI observation system. Journal of Marriage and Family, 62, 61–67.
Heavey, C. L., Larson, B. M., Zumtobel, D. C., & Christensen, A. (1996). The communication patterns questionnaire: The reliability and validity of a constructive communication subscale. Journal of Marriage and Family, 58, 796–800.
Helgeson, V., & Cohen, S. (1996). Social support and adjustment to cancer: Reconciling descriptive, correlational and intervention research. Health Psychology, 15(2), 135–148.
Hendrick, S. S. (1988). A generic measure of relationship satisfaction. Journal of Marriage and the Family, 50, 93–98.
Heyman, R. E. (2001). Observation of couple conflicts: Clinical assessment applications, stubborn truths and shaky foundations. Psychological Assessment, 13, 5–35.
Jacobson, N. S., McDonald, D. W., Follette, W. C., & Berley, R. A. (1985). Attributional processes in distressed and nondistressed married couples. Cognitive Therapy Research, 9, 35–50.
Kavanagh, D.J., O’Halloran, P., Manicavasagar, V., Clark, D., Piatkowska, O., Tennant, C., Rosen, A. (1997). The family attitude scale: Reliability and validity of a new scale for measuring the emotional climate of families. Psychiatry Research, 70, 185–195.
Kayser, K. (2005). Enhancing dyadic coping during a time of crisis: A theory-based intervention with breast cancer patients and their partners. In T. A. Revenson, K. Kayser, & G. Bodenmann (Eds.), Couples coping with stress: Emerging perspectives on dyadic coping (pp. 33–50). Washington, DC: American Psychological Association.
Kayser, K., & Scott, J. (2008). Helping couples cope with women’s cancers. An evidence-based approach for practitioners. New York: Springer.
Kenny, D. A., & Acitelli, L. K. (2001). Accuracy and bias in the perception of the partner in a close relationship. Journal of Personality and Social Psychology, 80, 439–448.
Kornblith, A. B., Regan, M. M., Youngmee, K., Greer, G., Parker, B., Bennett, S., & Winer, E. (2006). Cancer-related communication between female patients and male partners scale: A pilot study. Psycho-Oncology, 15, 780–794.
Krokoff, L. J., Gottman, J. M., & Roy, A. K. (1988). Blue-collar marital interaction and a companionate philosophy of marriage. Journal of Personal and Social Relationships, 5, 201–222.
Kronmüller, K.-T., Backenstrass, M., Victor, D., Postelnicu, I., Schenkenbach, C., Joest, K., Fiedler, P., & Mundt, C. (2011). Quality of marital relationship and depression: Results of a 10-year prospective follow-up study. Journal of Affective Disorders, 128, 64–71.
Ligue Suisse contre le Cancer. (2005). Le dépistage du cancer du sein. Berne: Ligue suisse contre le cancer du sein.
Lister, Z. D. (2011). Diabetes and the couple dyad: Expressed emotion, diabetes control and management. Dissertation Abstracts International, A: The Humanities and Social Sciences, 71, 3438.
Magana, A., Goldstein, M., Karno, M., Miklowitz, D., Jenkins, J., & Falloon, I. (1986). A brief method for assessing expressed emotions in relatives of psychiatric patients. Psychiatry Research, 17, 203–212.
Manne, S. L., & Ostroff, J. S. (2008). Coping with breast cancer. A couples-focused group intervention. Oxford: University Press.
Manne, S. L., Alferi, T., Taylor, K. L., & Dougherty, J. (1999). Spousal negative responses to cancer patients: The role of social restriction, spouse mood and relationship satisfaction. Journal of Consulting and Clinical Psychology, 67, 352–361.
Manne, S. L., Ostroff, J., Sherman, M., Heyman, R. E., Ross, S., & Fox, K. (2004). Couples’ support-related communication, psychological distress, and relationship satisfaction among women with early stage breast cancer. Journal of Consulting and Clinical Psychology, 72, 660–670.
Margolin, G., & Wampold, B. E. (1981). Sequential analysis of conflict and accord in distressed and nondistressed marital partners. Journal of Consulting and Clinical Psychology, 49, 554–567.
Möller-Leimkühler, A. M., & Jandl, M. (2011). Expressed and perceived emotion over time: Does the patients’ view matter for the caregivers’ burden? European Archives of Psychiatry and Clinical Neuroscience, 261, 349–355.
Murray, S. L., Holmes, J. G., & Griffin, D. W. (1996). The benefits of positive illusions: Idealization and construction of satisfaction in close relationships. Journal of Personality and Social Psychology, 70, 79–98.
Neff, L. A., & Karney, B. R. (2005). Gender differences in social support: A question of skill or responsiveness? Journal of Personality and Social Psychology, 88, 79–90.
Northouse, L. L. (1989). The impact of breast cancer on patients and husbands. Cancer Nursing, 12, 276–284.
Northouse, L. L., Mood, D., Kershaw, T., Schafenacker, A., Mellon, S., Walker, J., Galvin, E., & Decker, V. (2002). Quality of life of women with recurrent breast and their family members. Journal of Clinical Oncology, 20, 4050–4064.
Nye, F. (1988). Fifty years of family research 1937–1987. Journal of Marriage and Family, 50, 305–316.
Pistrang, N., & Barker, C. (1995). The partner relationship in psychological response to breast cancer. Social Science and Medicine, 40, 789–797.
Rhoades, G. K., & Stocker, C. M. (2006). Can spouses provide knowledge of each other’s communication patterns? A study of self-reports, spouses’ reports, and observational coding. Family Process, 45, 499–511.
Schulz, U., & Schwarzer, R. (2004). Long-term effects of spousal support on coping with cancer after surgery. Journal of Social and Clinical Psychology, 23, 716–732.
Schwarzer, R., & Leppin, A. (1989). Sozialer Rückhalt und Gesundheit: Eine Meta-Analyse. Göttingen: Hogrefe.
Sillars, A. L. (1985). Interpersonal perceptions in relationships. In W. Ickes (Ed.), Compatible and incompatible relationships (pp. 277–305). New York: Springer-Verlag.
Uchino, B. N. (2004). Social support and physical health: Understanding the health consequences of our relationships. New Haven: Yale University Press.
Vandeleur, C., Kavanagh, D. J., Favez, N., Castelao, E., & Preisig, M. (2013). French version of the Family Attitude Scale: Psychometric properties and relation of attitudes to the respondent's psychiatric status. Psychiatry Research, 210, 641–646.
Vincent, J. P., Friedman, L. C., Nugent, J., & Messerly, L. (1979). Demand characteristics in observations of marital interaction. Journal of Consulting and Clinical Psychology, 47, 557–566.
Weiss, R. (1974). The provisions of social relationships. In Z. Rubin (Ed.), Doing unto other (pp. 17–26). Englewood Cliffs: Prentice-Hall.
Weiss, R., & Heyman, R. (2004). Couples observational research: An impertinent, critical overview. In P. Kerig & D. Baucom (Eds.), Couple observational coding systems (pp. 11–25). Mahwah: Lawrence Erlbaum.
Wortman, C. B., & Dunkel-Schetter, C. (1987). Conceptual and methodological issues in the study of social support. In A. Baum & J. E. Singer (Eds.), Handbook of psychology and health(Vol. 5, pp. 63–108). Hillsdale: Lawrence Erlbaum.
Zimmermann, T., & Heinrichs, N. (2006). Psychosoziale Interventionen für Frauen mit Krebserkrankungen der Genitalorgane. Verhaltenstherapie & Verhaltensmedizin, 27(2), 125–141.
Zimmermann, T., & Heinrichs, N. (2008). Seite an Seite. Eine gynäkologische Krebserkrankung in der Partnerschaft gemeinsam bewältigen: Ein Ratgeber für Paare. Göttingen: Hogrefe-Verlag.
Zimmermann, T., Heinrichs, N., & Baucom, D. H. (2007). Does one size fit all? Moderators in psychosocial interventions for breast cancer patients. A meta-analysis. Annals of Behavioral Medicine, 34(3), 225–239.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution-NonCommercial 2.5 International License (http://creativecommons.org/licenses/by-nc/2.5/), which permits any noncommercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made. The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2016 The Author(s)
About this chapter
Cite this chapter
Charvoz, L., Favez, N., Cairo Notari, S., Panes-Ruedin, B., Delaloye, JF. (2016). A Survey of Couples Facing Breast Cancer in Women. In: Oris, M., Roberts, C., Joye, D., Ernst Stähli, M. (eds) Surveying Human Vulnerabilities across the Life Course. Life Course Research and Social Policies, vol 3. Springer, Cham. https://doi.org/10.1007/978-3-319-24157-9_5
Download citation
DOI: https://doi.org/10.1007/978-3-319-24157-9_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-24155-5
Online ISBN: 978-3-319-24157-9
eBook Packages: Social SciencesSocial Sciences (R0)