Abstract
Possibilities for action depend on the fit between the body and the environment. Perceiving what actions are possible is challenging, because the body and the environment are always changing. How do people adapt to changes in body size and compression? In Experiment 1, we tested pregnant women monthly over the course of pregnancy to determine whether they adapted to changing possibilities for squeezing through doorways. As women gained belly girth and weight, previously passable doorways were no longer passable, but women’s decisions to attempt passage tracked their changing abilities. Moreover, their accuracy was equivalent to that of nonpregnant adults. In Experiment 2, nonpregnant adults wore a “pregnancy pack” that instantly increased the size of their bellies, and they judged whether doorways were passable. Accuracy in the “pregnant” participants was only marginally worse than that of actual pregnant women, suggesting that participants adapted to the prosthesis during the test session. In Experiment 3, participants wore the pregnancy pack and gauged passability before and after attempting passage. The judgments were grossly inaccurate prior to receiving feedback. These findings indicate that experience facilitates perceptual–motor recalibration for certain types of actions.
Similar content being viewed by others


Over the course of pregnancy, women’s bodies undergo dramatic changes. These changes include the obvious gains in body mass: The typical weight gain during pregnancy is 12–16 kg (US Institute of Medicine, 1990), and some women enlarge by 20 kg or more (Bracero & Byrne, 1998). Weight gain is slow in the first trimester, becomes rapid in the second trimester, and tapers off slightly in the third trimester (Carmichael, Abrams, & Selvin, 1997). Of course, the additional body mass is not evenly distributed: Women’s abdomens increase by 31 % of their original size in order to accommodate the growing fetus (Jensen, Doucet, & Treitz, 1996). The change in body proportions causes an anterior shift in the center of mass, as women’s large bellies pull them forward (Fries & Hellebrandt, 1943). But these changes are not permanent. During delivery, mothers immediately shed much of the acquired mass in the form of 3.4 kg of newborn infant and 0.6 kg of placenta, eventually losing a total of 10 kg of their pregnant body mass by 6 months postpartum (Soltani & Fraser, 2000).
Physical changes to the body have functional consequences for motor abilities. The forward shift of the center of mass destabilizes the body. While trying to stand still, pregnant women sway more than nonpregnant women (Butler, Colon, Druzin, & Rose, 2006). Moreover, pregnant women lean backward—by as much as 28º—to compensate for their large bellies (Whitcome, Shapiro, & Lieberman, 2007). Balance in pregnant women is precarious, and the risk of falling increases (Dunning et al., 2003). Changes in body size and proportions also affect gait. Some pregnant women adopt a “waddling gait” by widening their base of support to keep balance (Bird, Menz, & Hyde, 1999). Most, however, maintain an outwardly normal gait pattern (Wu et al., 2004), but to do so places additional strain on their hip and ankle muscles (Foti, Davids, & Bagley, 2000). After delivery, balance and locomotion return to normal as women’s bodies begin reverting to their original size and shape.
Perceiving changing possibilities for action
The relation between pregnant women’s changing bodies and abilities typifies a general issue in perception and action: Possibilities for action reflect the fit between body and environment—what Gibson (1979) termed “affordances.” When the body changes relative to the environment, affordances also change (Adolph, 2008). Affordances change across the lifespan. From infancy to old age, motor abilities depend on body size and morphology. For example, a small child can easily slip through a narrow doorway that is impassable for a large adult; the adult can touch a high shelf that is out of reach for the child. But not all changes are developmental or permanent; bodies change over shorter time scales as well. Nutrition, activity, illness, and other such factors can cause fluctuations in the size and shape of the body that have consequences for action.
The problem for the perceptual system is to perceive affordances accurately, given the large range of potential bodies that one might have and of environmental challenges that one might face. Which actions are possible, and which are not? To perceive affordances accurately, perceptual information must be calibrated to action possibilities (Bingham & Pagano, 1998; Mark, 1987; Mark, Baillet, Craver, Douglas, & Fox, 1990; Warren, 1984; Warren & Whang, 1987; Withagen & Michaels, 2005). For example, perceptual information about the size of an opening must be scaled to one’s actual ability to fit through the opening. A fixed solution linking visual information to action possibilities will fail over time, because what you can do today might be different from what you can do tomorrow. To select and modify actions adaptively, perception of affordances must be flexibly adapted to changes in the body and the environment (Adolph, 2008). Recalibration is needed to align perception and action. Here we asked about the role of motor experience in recalibrating to changing affordances over the course of pregnancy. Do pregnant women take changes in their growing bodies into account when perceiving affordances for action?
Despite a burgeoning literature reporting changes in body size, gait, and balance over pregnancy (e.g., Butler et al., 2006; Soltani & Fraser, 2000; Wu et al., 2004), no empirical work has tested whether pregnant women adapt to changing possibilities for action. There is reason to expect that affordance perception may be hindered during pregnancy: With such rapid changes to their bodies, pregnant women’s judgments may be based on their original, prepregnancy body dimensions, or perception may lag behind their growing bodies. Anecdotally, pregnant women report bumping into furniture or burning their bellies while ironing. Popular guides, such as What to Expect When You’re Expecting (Murkoff & Mazel, 2008), warn women about the dangers of pregnancy-induced clumsiness. But is clumsiness the same as failing to perceive affordances? Although pregnant women are more susceptible to balance errors (Butler et al., 2006; Dunning et al., 2003), perceiving the fit between the body and the environment may be an entirely different matter.
Judging possibilities for fitting through openings is a common paradigm for assessing the perception of affordances (Franchak, Celano, & Adolph, 2012; Franchak, van der Zalm, & Adolph, 2010; Higuchi, Cinelli, Greig, & Patla, 2006; Higuchi et al., 2011; Stefanucci & Geuss, 2010; Wagman & Taylor, 2005; Warren & Whang, 1987). Adults report accurately whether they can squeeze through openings within 2 cm of their actual abilities (Franchak et al., 2010), and evidence of body scaling is apparent across the lifespan, from infancy (Franchak & Adolph, 2012) to old age (Comalli, Franchak, Char, & Adolph, 2013). Adults can adapt to experimentally induced changes to their bodies: They adapt their decisions to their new body dimensions for fitting under barriers when wearing platform shoes or large helmets (Stefanucci & Geuss, 2010), reaching through openings while wearing bulky gloves (Ishak, Adolph, & Lin, 2008), or walking through horizontal openings while wearing shoulder pads (Higuchi et al., 2011). Pregnant women might adapt to changing affordances as accurately as adults whose bodies were altered experimentally, but affordance perception has not been studied with regard to real, physical growth.
The role of motor experience in perceptual–motor recalibration
If pregnant women successfully adapt to changing affordances, what process might account for their recalibration? Previous work suggests that affordance perception depends on intrinsic information (e.g., information about the observer’s body) and, moreover, that experience moving the body is critical for perceptual–motor recalibration (Mark, 1987; Mark et al., 1990; Stoffregen, Yang, & Bardy, 2005; Warren, 1984; Warren & Whang, 1987; Yu, Bardy, & Stoffregen, 2011). For example, intrinsic information about the body’s height, such as that provided by eye height and postural sway, allows observers to make accurate decisions about what openings are possible to walk through (Warren & Whang, 1987), what barriers are possible to fit under (Stoffregen, Yang, Giveans, Flanagan, & Bardy, 2009; Yu et al., 2011), and what risers are possible to step on and sit on (Mark, 1987; Mark et al., 1990; Stoffregen et al., 2005; Warren, 1984). When wearing platform shoes that increase standing height, experience moving the body facilitates recalibration (Mark, 1987; Mark et al., 1990): Observers cannot accurately judge their new abilities when movement is restricted (e.g., standing still with their backs against a wall), but the swaying movements of the body while standing in place facilitates recalibration of affordance perception. Similarly, novice wheelchair users cannot accurately judge what barriers are possible to roll under if head movement is restricted, but can accurately judge affordances when head movements are not restricted (Yu et al., 2011).
For these height-scaled actions, specific practice performing the target action does not improve recalibration beyond the improvements gained through general experience with the body in motion. Presumably, the body’s postural sway during normal movement generates sufficient visual information (via optic flow) to inform on changes to height, facilitating recalibration of height-scaled affordances. However, if the critical information for affordances is not available in vision, perceptual–motor recalibration may require experience performing the specific action. For example, observers may not be able to perceive affordances involving friction and rigidity through vision because friction and rigidity are emergent properties—they depend on the relation between two surfaces. When walking on a surface, the slipperiness of the surface depends on the surface characteristics with respect to the characteristics of the walker’s shoe (Adolph & Joh, 2009). Visual information about the surface, such as shine, does not provide information about affordances for walking on slippery ground (Joh, Adolph, Campbell, & Eppler, 2006). Similarly, rigidity depends on the compliance of two surfaces and the amount of applied force. It seems unlikely that there is visual information specifying the compliance of a surface given a yet-to-be applied force. In lieu of visual information, haptic experience pressing against the surface can inform as to its rigidity (Adolph & Joh, 2009; Joh & Adolph, 2006).
Affordances for squeezing through openings depend in part on the rigidity of the body—how much the torso can compress. (Comalli et al., 2013; Ishak et al., 2008). Young adults’ torsos can compress by 3 to 4 cm, and compressed body size predicts what doorways are possible to squeeze through. Indeed, practice performing the specific action facilitates perception of affordances for squeezing through doorways, even when body dimensions have not been altered. For example, participants who completed 20 practice trials squeezing through doorways were slightly more accurate than participants who judged passability without practice (Franchak et al., 2010). However, the benefit of practice may be even greater when the body has changed. We predicted that specific practice would facilitate recalibration to altered body size and compression in the task of squeezing through openings.
We tested this prediction in three experiments. We chose the affordance of squeezing sideways through doorways so as to contrast with prior work that investigated recalibration to changes in height-scaled affordances: Adaptation to changes involving torso width and compression has not been previously reported. In Experiment 1, we tracked pregnant women longitudinally to determine whether everyday experience is sufficient to facilitate recalibration to changing affordances for squeezing through doorways. In Experiment 2, we manipulated participants’ body dimensions with a pregnancy prosthesis to test whether they could recalibrate to a sudden change in body size and compression. Finally, in Experiment 3 we tested whether specific experience squeezing through doorways was necessary for recalibrating to altered body dimensions.
Experiment 1: Pregnant women
We tracked women’s changing body dimensions and corresponding changes in affordances for squeezing through doorways over the course of pregnancy and following delivery. At each monthly session, we determined an affordance threshold for each woman—the opening size that she could squeeze through on 50 % of trials. If measured accurately, changes in affordance thresholds over pregnancy should track changes in relevant body dimensions. We also determined a decision threshold for each woman, indicating the smallest opening that she judged possible to squeeze through. If pregnant women’s perception of affordances failed to update to account for changes in the body, decision errors—the discrepancy between affordance and decision thresholds—should increase as women’s bodies grow farther from their original size. However, if women adapt to changes in their bodies, errors should not increase, and decision thresholds should closely match affordance thresholds.
Method
Participants and design
A group of 11 women participated, who were 25 to 42 years of age at the first test session (M = 32.7 years). All of the women had normal or corrected-to-normal vision. Women were recruited through word of mouth and received a photo album documenting their pregnancies as a souvenir. One additional woman was recruited but could not participate after her second session for medical reasons; her data are excluded from the analyses.
Ten women visited the lab once a month over the course of their pregnancies and for a final session after giving birth. Each woman completed four to eight test sessions, depending on when they were recruited relative to their delivery dates (Table 1). Once enrolled in the study, no participant missed a test session. One woman completed 20 weekly test sessions from her 4th month of pregnancy until delivery, and two sessions at 1 and 4 weeks postpartum.
Apparatus
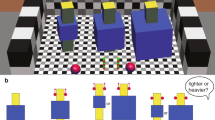
Doorways of varying width were presented by using an adjustable, wooden apparatus constructed on a large platform that measured 490 cm long × 98 cm wide × 64 cm high (Fig. 1). A stationary wall (122 cm long × 173 cm high) was attached to the side of the platform, and a moving wall (114 cm wide × 191 cm high) was attached to the other side of the platform, perpendicular to the stationary wall and positioned 304 cm from the start of the walkway. The moving wall adjusted in 0.2-cm increments, creating doorways that varied from 0 to 74 cm in width. Participants began each trial behind a starting line 250 cm from the moving wall.

Adjustable apparatus to create doorways of varying width. Pregnant women walked along a raised walkway toward doorways and turned their bodies to squeeze through
A measurement camera recorded calibration markings, helping the experimenter to adjust the doorway accurately. In addition, two cameras recorded women’s movements during the trial: a panning side camera captured the approach to the opening, and a fixed overhead camera focused on the participant moving through the opening. All three camera views were mixed into a single frame and digitally captured by a computer using a video capture card (Winfast).
Procedure
In each session, women completed M = 67.5 trials of walking through doorways, followed by measurements of their body dimensions. Each walking trial began with the woman standing on the starting line facing away from the doorway while the experimenter adjusted the apparatus. After hearing a verbal cue, the woman turned to face the opening and made her decision: Women were instructed to attempt to walk through the doorway if they believed that they could fit through without getting stuck, but to refuse to attempt if they did not. They could abort their attempt at any point during the approach, which counted as a refusal. Women spontaneously turned and walked through in a sideways orientation on all but the largest doorways, and on the narrowest doorways, walking was momentarily interrupted as they squeezed through.
The experimenter scored each trial as a successful attempt (S = walked through without becoming wedged), failed attempt (F = body became wedged in the opening), or refusal (R = woman did not enter the doorway). The experimenter entered the result of each trial into a customized MATLAB program that fit an affordance function (based on the rate of successes to failures) and a decision function (based on the rate of attempts to refusals) to the woman’s data. The program suggested a doorway width for each trial to facilitate the curve fit for each function: Sessions began with a binary search for thresholds for the first ten trials, followed by randomized trials presented within a three-SD range of the current estimate of each threshold (see Franchak et al., 2010, for details).
The affordance and decision functions (Fig. 2) were modeled as Gaussian cumulative probability density functions using maximum likelihood estimates of the mu (threshold) and sigma (standard deviation) parameters (for details, see Franchak & Adolph, 2013). The affordance function characterized women’s ability to fit through doorways on the basis of their success rate at each doorway size [S / (S + F)]. The decision function characterized their perception of whether they could fit through doorways on the basis of their attempt rate at each doorway size [(S + F) / (S + F + R)]. The discrepancy between the decision threshold and the affordance threshold provided a measure of decision error (dashed line in Fig. 2). The sigma parameter of the decision function characterized sensitivity to affordances by measuring the variability of participants’ responses.

Example affordance and decision functions for one participant’s session. Gray squares show success rates, and white circles show attempt rates at each doorway size. Symbol size denotes the number of trials; the smallest symbols = one trial, and the largest symbols = five trials. The affordance function (gray curve) was fit to the success rate, and the decision function (black curve) was fit to the attempt rate. Decision error (dashed line) was calculated as the difference between the 50 % points of the two functions
At the end of the session, weight was recorded on a digital scale, and stomach circumference was measured at the navel with a tape measure. For safety reasons, we did not measure compression body dimensions in pregnant women. Sessions lasted about 1 h.
Data processing
A primary coder rescored the outcome of each trial using a computerized video-coding system, Datavyu (www.datavyu.org). A second, reliability coder scored 25 % of the trials. The two coders agreed on M = 96.2 % of the trials (κ = .945); disagreements between the coders were resolved by discussion.
The affordance and decision functions were refit to the hand-coded data, and the resulting parameters were used in the analyses. A parametric bootstrap with 1,000 Monte Carlo iterations provided 95 % confidence intervals for the estimates of the affordance and decision function parameters (Wichmann & Hill, 2001). The margin of error for the curve fits was less than a centimeter: The affordance threshold estimates averaged 26.70 ± 0.58 cm, and the decision threshold estimates averaged 25.58 ± 0.59 cm.
Results and discussion
Because women completed test sessions at different points in their pregnancies, we calculated the number of weeks of gestation at each test session relative to each woman’s due date (40 weeks). Table 1 shows the number of weeks of gestation for the first session of each participant and the number of test sessions completed.
Developmental trajectories for body dimensions, abilities, and decisions were analyzed using linear generalized estimating equations (GEE) that modeled a group trajectory based on the trajectories of each individual. Similar to a univariate linear regression, GEE models estimate linear change in a dependent measure from a continuous predictor. Each GEE model used an autoregressive correlation matrix to reflect individual change: Every measurement depended on a participant’s measurement at the previous session. In addition, to examine individual differences in developmental trajectories, we also calculated linear regressions for each woman; individual Bs and R 2s are shown in Table 2.
Developmental change in bodies and affordances
Figures 3a and b show a continual increase in weight and stomach circumference for each woman from the first session until delivery. A GEE model predicting weight on the basis of weeks of gestation showed that women gained B = 0.46 kg/week (Wald’s χ 2 = 193.1, p < .001), consistent with the rate of weight gain (0.4 to 0.5 kg/week) reported in the medical literature (Abrams, Carmichael, & Selvin, 1995; Carmichael et al., 1997). However, individual linear regressions showed variability in growth rates: The rate of weight gain ranged from a modest B = 0.14 kg/week to a rapid 0.67 kg/week; weeks’ gestation accounted for R 2s ≥ 88 % of the variance in weight gain (Table 2). Similarly, stomach circumference increased at a rate of B = 0.91 cm/week, on the basis of a GEE model with weeks’ gestation as the predictor (Wald’s χ 2 = 136.7, p < .001). Like weight gain, increase in stomach circumference also varied widely, ranging from B = 0.14 cm/week to 1.33 cm/week. Weeks gestation accounted for R 2s ≥ 63 % of variation in stomach circumference. Thus, at each monthly session, women found themselves about 1.8 kg heavier, with an extra 3.6 cm of belly girth.

Scatterplots showing changes for each pregnant woman over pregnancy and in the postpartum session. a weight, b stomach circumference, c affordance threshold, and d decision threshold. Each woman’s data are denoted by a different symbol type. Solid black lines show the generalized estimating equation model fits
The changes in women’s bodies were mirrored by changes in their ability to fit through doorways. Affordance thresholds increased by B = 0.39 cm/week, as confirmed by a GEE model with weeks’ gestation as the predictor (Wald’s χ 2 = 68.0, p < .001, Fig. 3c). On the basis of that rate, each monthly session incurred roughly 1.6 cm of increased affordance threshold, totaling 9.6 cm over the 2nd and 3rd trimesters of pregnancy. As Table 2 shows, this rate varied from B = 0.17 to B = 0.63 cm/week between women, with weeks’ gestation accounting for R 2s ≥ 72 % of the variation in affordance thresholds.
After giving birth, women’s bodies change drastically. However, because participants were (understandably) not eager to visit the lab in the days immediately following delivery, the final test sessions took place M = 5.5 weeks postpartum (see Table 1 for the individual test intervals). Furthermore, the test session preceding birth occurred M = 3.1 weeks before delivery, so we cannot report the full extent of women’s growth leading up to delivery. Although we are unable to describe the exact trajectories of body size between the pre- and postpartum sessions, it is clear that a tremendous amount of weight and torso size was lost by 4–5 weeks after delivery: On average, women had lost M = 8.25 kg (SD = 1.97 kg) and M = 16.21 cm (SD = 4.76 cm) of stomach circumference (Figs. 3a–b). Changes in body dimensions accompanied changes in abilities: Affordance thresholds decreased by M = 7.18 cm (SD = 2.33 cm) from the pre- to the postpartum session (Fig. 3c).
Adapting decisions to changing affordances
Did women update their decisions to changing affordances for passage? If women’s judgments were calibrated to their original, nonpregnant body dimensions, we would expect decision thresholds to change at a slower rate than affordance thresholds—decisions would fail to keep pace with rapid changes in abilities. However, Fig. 3d shows that women’s perceptions of action possibilities changed at a rate that matched their changing abilities, indicating that they adapted their decisions to changing affordances. A GEE model with weeks’ gestation predicting decision threshold revealed that decisions increased at a rate of B = 0.37 cm/week (Wald’s χ 2 = 66.5, p < .001) Individual linear regressions showed that decision threshold rates of change varied from B = 0.23 to 0.68 cm/week between women, with weeks’ gestation accounting for R 2s ≥ 57 % of variation in decision thresholds (Table 2). A paired-samples t test on the individual regression coefficients indicated that decisions changed at a greater rate than affordances, t(10) = –2.77, p = .02.
Accuracy of decisions
Pregnant women’s decisions adapted to affordances, but were their decisions accurate? Decisions may have changed at the same rate as affordances while lagging one to two months behind, resulting in poor accuracy. We calculated decision error by subtracting the decision threshold from the affordance threshold: Positive values would indicate overestimation by attempting impossibly small doorways, whereas negative values would indicate underestimation by refusing to walk through possible openings. Signed decision errors averaged M = 0.59 cm (SD = 2.05 cm) during pregnancy and M = –0.01 cm (SD = 2.04 cm) postpartum. Across the pre- and postpartum sessions, 55.5 % of sessions showed positive errors, and 45.0 % had negative errors. Because positive and negatives errors cancel out when averaging signed errors, we calculated absolute error in order to examine the magnitude of errors, regardless of error direction; absolute errors averaged only M = 1.63 cm (SD = 1.36 cm) during pregnancy, and M = 1.62 cm (SD = 1.15 cm) in the postpartum sessions.
We tested for changes in signed decision error and absolute error over pregnancy (excluding the postpartum sessions) with GEE models using weeks of gestation as a predictor. Signed error showed a small but significant decrease, B = –0.06 cm/week (Wald’s χ 2 = 4.83, p = .027), indicating that women became somewhat more likely to make errors of underestimation. However, absolute error did not show significant change, B = –0.03 cm/week (Wald’s χ 2 = 2.94, p = .086). Thus, although women refused to attempt possible doorways more often over the weeks of gestation, the trend was not strong enough to significantly impact on absolute error. The lack of a change in absolute error indicates that women maintained a constant error of 1.6 cm throughout their pregnancies—roughly the same as the monthly increase in their affordance thresholds.
How should we consider a decision error of 1.6 cm? Because we recruited women who were already pregnant, we could not compare accuracy during pregnancy to accuracy prepregnancy. However, comparisons with previous work indicated that pregnant women were highly accurate. Nonpregnant, college-aged adults erred by M = 1.62 cm in a similar task (Franchak et al., 2010, action-first condition) and did not differ significantly from the pregnant women in the present study, t(21) = 0.30, p = .764, suggesting that pregnant women’s perceptions of affordances fully adapted to changes in functional body dimensions.
Variability of decisions
Aside from the effects of scaling and accuracy, we considered the possibility that decisions became more variable as bodies became larger. That is, even if the decision thresholds matched affordance thresholds, women might have responded inconsistently over a larger range of aperture widths. Across sessions, the decision functions varied by a mean sigma (standard deviation) of 1.02 cm (SD = 0.73 cm), about twice as much as the affordances varied, M = 0.52 cm (SD = 0.63 cm). However, decision variability did not increase over pregnancy, showing a marginal decrease of B = –0.23 cm/week in a GEE model with weeks’ gestation as the predictor (Wald’s χ 2 = 3.05, p = .081). Like accuracy, pregnant women’s decision variability was comparable to that of nonpregnant adults in previous research, M = 1.11 cm (Franchak et al., 2010).
Experiment 2: “Pregnant” people
Experiment 1 demonstrated that pregnant women recalibrated to changing affordances for squeezing through doorways over the course of pregnancy and following delivery. How did they achieve this impressive feat? Pregnant women had a week’s or a month’s worth of experience between each session to adapt to changes in their bodies. Was this prolonged experience necessary for recalibration, or might women have recalibrated more rapidly? We addressed the issue of prolonged experience in Experiment 2 by asking whether adults could cope with a sudden, dramatic change in body size. Nonpregnant adults wore a “pregnancy pack” that increased the size of their abdomens, and they completed the same task as in Experiment 1. We compared the accuracy of participants wearing the pregnancy pack to that of “no-pack” participants whose bodies had not been experimentally altered. If prolonged experience is required to recalibrate to changes in body size and compression, “pregnancy pack” participants should not recalibrate during the test session.
Method
Participants and design
A group of 48 men and women 18–24 years of age (M = 19.9 years) participated. They were recruited from the psychology department’s subject pool and received course credit for participation. Half were assigned to the “pregnancy pack” condition, and the other half were assigned to the “no-pack” condition, with sex split evenly between conditions.
Apparatus
Participants assigned to the pregnancy pack condition wore a custom-made prosthesis that increased the size of their bellies (Fig. 4). The pregnancy pack consisted of a dome-shaped piece of foam measuring 28 cm in diameter and protruding 15 cm from the body. The foam belly was hollowed out and filled with dry beans to increase the rigidity of the prosthesis, ensuring that, although the belly would compress by a few centimeters, participants could not completely deform it by pressing against the doorway. The belly weighed 2.5 kg. It was secured to a Velcro belt that fit around the waist, and shoulder straps helped to keep the prosthesis in place. Although the prosthesis simulated some aspects of pregnancy (gains to torso size shifting the center of mass), the manipulation was not designed to fully mimic the biomechanical changes incurred by pregnant women (e.g., overall body mass, gait, and balance). The doorway apparatus and cameras were the same as in Experiment 1.

Procedure
The trial procedure was identical to that of Experiment 1: Participants in both conditions completed M = 54.5 trials of squeezing through doorways. Participants were instructed to attempt to fit through with their bodies turned sideways. Affordance and decision functions were fit to the success and attempt data. Participants in the pregnancy pack condition put on the prosthesis right before the first trial and were not given time to acclimate to the prosthesis before testing. After the test trials, participants removed the prosthesis and completed an additional 15 trials to estimate their affordance function without the pregnancy pack, in order to determine the size of the manipulation.
Data processing
As in Experiment 1, a primary coder rescored the outcome of each trial, and a reliability coder scored 25 % of the trials. The two coders agreed on M = 95.1 % of trials (κ = .922); disagreements between coders were resolved by discussion. Preliminary analyses did not reveal any differences between male and female participants, so subsequent analyses omit sex as a factor.
As before, we used a parametric bootstrap with 1,000 Monte Carlo iterations to provide 95 % confidence intervals for the mu parameters of the affordance and decision functions. The affordance threshold estimates averaged M = 24.32 ± 0.54 cm, and the decision threshold estimates averaged M = 23.37 ± 0.59 cm.
Results and discussion
Affordances for squeezing through doorways
Comparing affordance thresholds with and without the prosthesis for participants in the pregnancy pack condition showed that wearing the pack increased thresholds by M = 10.48 cm (SD = 2.67 cm). As can be seen in Fig. 5, thresholds in the pregnancy pack condition averaged M = 30.15 cm (SD = 4.14 cm). Pregnancy pack thresholds overlapped with the upper range of pregnant women’s thresholds. Just as pregnancy affected each woman differently, depending on her starting size, the same pregnancy pack resulted in a range of thresholds, depending on the participants’ original size.

Decision thresholds (white circles) relative to affordance thresholds (black squares) for each participant in Experiments 2 and 3, ordered from the smallest to the largest affordance thresholds. Decision errors are shown by the dashed lines. For participants in Experiment 3, pretest decision thresholds and pretest decision errors are shown by gray circles and gray lines, respectively
Without the prosthesis, thresholds averaged M = 19.68 cm (SD = 2.67 cm) for participants who had previously participated in the pregnancy pack condition, which was comparable to the affordance thresholds of participants in the no-pack condition (M = 18.26 cm, SD = 2.18 cm). Thresholds in the no-pack condition were similar to the lower range of pregnant women’s thresholds.
Accuracy of decisions
Figure 5 shows the decision threshold relative to the affordance threshold for each participant. We calculated signed error and absolute error as in Experiment 1. Participants wearing the pregnancy pack tended to underestimate affordances by refusing to attempt possible openings: The signed decision errors averaged M = –0.87 cm (SD = 3.59 cm). Although participants without the prosthesis overestimated affordances by attempting too-small openings (M = 0.49 cm, SD = 2.03), the signed decision errors did not differ between conditions, t(46) = 1.62, p = .11. However, wearing the pregnancy pack caused a marginal increase in absolute error: Wearing the pregnancy pack induced errors of M = 2.72 cm (SD = 2.24 cm), whereas participants without the prosthesis erred by only M = 1.63 cm (SD = 1.27 cm), t(46) = –1.96, p = .056. Of note, pregnant women’s 1.6-cm absolute error was comparable to that of participants not wearing the prosthesis, providing further evidence that they adapted to changes in their bodies. However, we were surprised that participants wearing the prosthesis only erred by 1.1 cm more than participants without the prosthesis, despite a 10.5-cm increase in body size.
We considered the possibility that pregnancy pack participants adapted to the prosthesis during the test session. Participants wearing the pregnancy pack may have initially made large errors but used feedback to correct their decisions over the course of the session. Indeed, the largest single errors of participants wearing the pregnancy pack (M = 5.72 cm, SD = 3.92 cm) were of greater magnitude than those in the no-pack group (M = 3.50 cm, SD = 2.65 cm), t(46) = –2.31, p = .025. Moreover, participants wearing the prosthesis made their largest errors earlier in the session (trial number M = 17.03, SD = 13.44) than did participants in the no-pack group (trial number M = 27.03, SD = 18.16), t(46) = 2.298, p = .026. Error feedback in the first trials of the session most likely facilitated learning about their new body dimensions and helped to prevent errors on subsequent trials.
Variability of decisions
Finally, we tested whether the sudden change to body dimensions incurred an increase in decision variability: Greater uncertainty about body dimensions might result in less consistent motor decisions. The sigma parameters of decision functions in the pregnancy pack condition (M = 1.80 cm, SD = 1.15 cm) were slightly larger than those of participants in the no-pack condition, (M = 1.37 cm, SD = 1.04 cm); however, the difference failed to reach significance, t(46) = –1.34, p = .19. Like decision error, decision variability was comparable between no-pack participants and actual pregnant women.
Experiment 3: The role of feedback in recalibration
Experiment 2 showed that “pregnant” participants were slightly less accurate than those whose bodies were not changed. But participants wearing the pregnancy pack made larger errors early in the session, suggesting that feedback from attempting to squeeze through openings improved judgments on subsequent trials. Because we used a randomized trial protocol and participants could decide whether to attempt each doorway size, individual participants received different amounts of feedback. We addressed this difference in Experiment 3 by separating perceptual judgments from motor feedback: Participants wore the pregnancy pack and made yes/no judgments while standing at the starting line. Then they walked through various doorways. Assessing judgment accuracy before and after specific practice squeezing through doorways allowed us to examine the role of feedback in recalibration. Judgment accuracy prior to feedback should be worse if specific practice is required in order to recalibrate perception of affordances for squeezing through doorways—which is of special interest because information about body compression requires the surfaces (belly and doorway) to press against each other.
Method
Participants and apparatus
A group of 12 men and women 18–22 years of age (M = 20.6 years) participated. They were recruited from the psychology department’s subject pool and received course credit for participation. The doorway apparatus and pregnancy pack were the same as in Experiment 2.
Procedure
Participants put on the pregnancy pack and then completed three blocks of trials in the following order: 30 pretest judgment trials, 20 walking experience trials, and 30 posttest judgment trials. In contrast to Experiments 1 and 2, participants made verbal judgments while standing at the starting line—they said “yes” if they thought they could squeeze through the opening, and “no” if they did not think that they could squeeze through in a sideways orientation. During judgment trials, participants did not attempt to walk through the opening but were permitted to move as much as they wanted while staying behind the starting line. Participants did not receive feedback about whether they could fit through doorways until the block of walking experience trials. During the walking experience trials, participants were asked to attempt to squeeze through doorways of varying sizes, regardless of whether they believed they could fit. Thus, each participant received 20 trials of feedback about whether passage was possible.
We fit a psychometric function to each block of trials. A pretest decision function and a posttest decision function were fit to the proportions of “yes” responses in the pretest and posttest judgment blocks, respectively, using the same fitting procedure as in Experiments 1 and 2. An affordance function was fit to the proportion of successes in the walking experience block. For each block of trials, trial order was determined using the same protocol as in Experiments 1 and 2.
At the end of the session, we measured participants’ sagittal body size while wearing the pregnancy pack by having them stand in the doorway with their backs against the stationary wall and closing the doorway until it came in contact with the prosthesis. Then we measured compressed sagittal body size by pressing the doorway against the prosthesis until it would no longer yield to pressure or the participant signaled discomfort.
Data processing
Because participants provided verbal responses rather than motor responses (as in Exps. 1 and 2), offline video coding was unnecessary. As before, a parametric bootstrap with 1,000 Monte Carlo iterations provided 95 % confidence intervals for the mu parameters of each function. The affordance threshold estimates averaged M = 27.91 ± 0.26 cm, the pretest decision threshold estimates averaged M = 38.16 ± 0.88 cm, and the posttest decision threshold estimates averaged M = 28.34 ± 0.47 cm.
Results and discussion
Affordances for squeezing through doorways
As is shown in Fig. 5, participants’ affordance thresholds while wearing the prosthesis were large, M = 27.91 cm (SD = 2.14 cm), similar to those of participants wearing the pregnancy pack in Experiment 2 (M = 30.15 cm). To verify that participants’ compressed body dimensions matched the affordance thresholds more closely than their static body dimensions, we calculated the difference between the affordance thresholds and each body measurement. As expected, the compressed body dimensions closely matched the affordance thresholds, deviating by only M = 0.64 cm (SD = 1.52 cm), whereas static body dimensions deviated by a greater amount (M = 7.69 cm, SD = 1.34 cm), t(11) = 19.62, p < .001.
Accuracy of decisions
We calculated the signed error and absolute error for the pretest and posttest decision thresholds in order to compare accuracy before and after specific practice squeezing through doorways. Figure 5 shows each participant’s pretest and posttest decision thresholds relative to their affordance thresholds. In the pretest, participants grossly misjudged affordances by overcompensating for the added girth of the prosthesis. Every participant underestimated affordances by saying “no” to doorways that were possible to navigate: Their signed error averaged M = –10.25 cm (SD = 6.61 cm), and the absolute error averaged M = 10.25 cm (SD = 6.61 cm). However, 20 feedback trials with practice squeezing through doorways reduced errors dramatically: Posttest signed errors averaged M = –0.43 cm (SD = 2.89 cm), and posttest absolute errors averaged M = 2.40 cm (SD = 1.50 cm). Paired t tests confirmed significant decreases in the signed errors, t(11) = 5.27, p < .001, and absolute errors, t(11) = 4.00, p = .002.
Variability of decisions
Finally, we compared the variability of decisions before and after practice squeezing through openings. Decision variability was significantly greater in the pretest (M = 1.55 cm, SD = 0.73) than in the posttest (M = 0.65 cm, SD = 0.44 cm), t(11) = 3.07, p = .011, suggesting that motor experience decreased participants’ uncertainty about affordances.
General discussion
In the present experiments, we examined recalibration of perception of affordances for squeezing through doorways. We contrasted participants’ recalibration in response to two changes to the body: real growth during pregnancy and simulated growth in the lab. In Experiment 1, pregnant women fully adapted to changes in their abilities to squeeze through doorways and made errors comparable to nonpregnant adults. As their bellies increased in size, so did their judgments of what doorways were possible to squeeze through in a sideways position. But pregnant women grew gradually and had the benefit of everyday experience to learn about their changing bodies. In Experiment 2, we sped up the process. Wearing the pregnancy pack simulated 9 months of belly growth in 1 min; thus, participants did not have the benefit of prolonged experience. Although errors were higher, relative to participants who did not wear the prosthesis, participants wearing the pregnancy pack were fairly accurate, despite a large change to their body dimensions. Experiment 3 showed that judgments when wearing the pregnancy pack were erroneous prior to experience squeezing through openings, but that action experience facilitated perceptual–motor recalibration.
Action experience and recalibration
Consistent with prior work on height-scaled affordances (Mark, 1987; Mark et al., 1990; Stoffregen et al., 2005; Warren, 1984; Warren & Whang, 1987; Yu et al., 2011), the present study shows that motor experience is crucial to the process of recalibration. Observers need to move in order to adapt. However, the role of movement—indirect experience from postural sway versus direct practice performing the action—depends on the perceptual information for affordances. Whereas optic flow generated by postural sway can provide information about body height, body compression cannot be perceived solely through vision. Thus, although standing in place is sufficient for recalibrating to changes in height, it is not sufficient for recalibrating to changes involving torso size and compression. Only after practice squeezing through openings did participants recalibrate to changing affordances; judgments prior to motor experience grossly missed the mark. Moreover, in prior work we demonstrated that even participants whose bodies have not been altered benefit from specific practice (Franchak et al., 2010), suggesting that the role of experience in affordance perception may extend beyond the process of recalibration.
Indeed, studies of other affordances have shown that experience improves perceptual judgments. Other emergent properties, like friction, also pose challenges for perceiving affordances (Joh et al., 2006; Joh, Adolph, Narayanan, & Dietz, 2007). Adults inaccurately judged whether they could stand on sloping surfaces covered in slippery vinyl. However, experience improved the judgments: Rubbing the feet on the surface of support provided information about friction, and subsequent decisions were accurate. Similarly, judgments about how far participants could propel their bodies by leaping were inaccurate prior to experience but matched their actual abilities following leaping experience (Cole, Chan, & Adolph, 2013). By measuring the underlying properties that determine a particular affordance, we may gain insight into how experience aids the observer in perceiving that affordance.
Although we concluded that specific experience was important for learning about affordances for squeezing through openings, the present experiments did not clearly distinguish which aspect of experience was critical. One possibility is that attempting to fit through the opening provided feedback about success and failure, and this feedback helped participants to hone their subsequent judgments. A second possibility is that by attempting to fit through openings, participants experienced the degree to which they could compress their bodies, given the amount of force applied. If so, simply pressing their bellies against any rigid surface might provide the requisite experience, which could perhaps be similar to how rubbing the feet against a flat surface provides information about affordances for standing on a slope covered with the same material (Joh et al., 2007). In future work, restricting participants’ vision while they squeeze through doorways might help us discern whether the present findings are due to motor experience alone or whether recalibration depends on perceptual–motor information.
The randomized trial design that we used did not allow for trial-by-trial analyses of recalibration. Future work should examine the time course of adaptation in order to determine whether participants adapt quickly after one or two trials of squeezing through, or whether numerous feedback trials are needed to fully recalibrate. Indeed, recalibration may follow different time courses, depending on the affordance. For example, prior work has shown that even after 8 days of practice, novice wheelchair users fail to fully recalibrate the spatial requirements of a wheelchair when judging what doorways are possible to wheel through (Higuchi, Takada, Matsuura, & Imanaka, 2004). In addition, we did not measure participants’ speed of approach or the distance from the doorway at which participants aborted their attempts. Variations in walking speed affect affordances for passage (Higuchi et al., 2011; Warren & Whang, 1987), and walking speed and viewing distance also affect the acquisition of visual information (Fath & Fajen, 2011; Higuchi et al., 2006; Wilmut & Barnett, 2010). Future work should use motion tracking to investigate how the observers’ walking dynamics affect visual information and whether modulations in walking speed and distance relate to observers’ motor decisions.
Perceptual–motor adaptation during pregnancy
We began this article by citing examples of how pregnancy poses challenges for keeping balance. If pregnant women recalibrate to changing affordances, why are falls common? Failing to perceive affordances leads to motor errors, but the converse is not necessarily true—not every motor error is the result of an error in perceiving affordances. If pregnant women’s falls are the result of poor motor decisions (i.e., deciding to descend too-steep slopes), we might attribute those falls to a failure of perception. More likely, higher rates of falling during pregnancy are not due to poor motor decisions, but rather are the result of noise in the motor system: Increased postural sway makes simply standing in one place a riskier venture. If pregnant women fall while walking on flat ground, we should not blame the perception of affordances.
Bumping into furniture and other spatial errors are a separate issue from balance. We found that pregnant women accurately perceived the space needed to accommodate their growing bodies. How might we explain these other errors that have been reported in pregnancy? Whereas pregnant women’s rate of falling has been rigorously documented (Dunning et al., 2003), the increased rate of spatial errors is only anecdotal. One possibility is that spatial errors do not increase in frequency but change in attribution. Pregnant women may bump into things just as often as nonpregnant adults, but when they do, they attribute the error to being pregnant. Indeed, with popular guides and websites warning women about pregnancy-induced clumsiness, bumping into furniture with a large belly may be more salient than it would be for a nonpregnant adult making a similar error.
The present study is the first to report perceptual recalibration in response to actual growth, as opposed to experimentally induced manipulations to body size. How do these findings generalize to other physical changes that are sustained over the lifespan? The all-too-common experience of weight gain likely operates similarly to pregnancy—experience might be necessary to facilitate recalibration to changes in body size and compression. So, too, would the less frequent experience of weight loss. But other changes might not require experience for calibration. Recalibration to changes in height from birth through puberty might be served by optic flow and postural sway to the extent that eye height sufficiently specifies affordances.
Conclusion
Finally, we stress that any change to the body must be considered with respect to a task and an environment. Pregnancy—like any change to the body—alters some affordances but not others. Gains in torso size will change affordances for squeezing through openings, but not for walking under barriers. In this sense, perceptual recalibration must be both flexible and specific. We must be able to adapt the perception of affordances to take relevant changes into account, sparing perception of affordances that are unaffected. The nature of the task, and not just the change in the body, are crucial for understanding the process of recalibration. Some tasks have clear relations to body dimensions and visual information. For these tasks, recalibration might occur without the need for practice. But tasks that rely on emergent properties like compression or friction complicate recalibration and may require learning from specific experience (Adolph & Joh, 2009). Indeed, some affordances that were previously considered as body-scaled might in fact be action-scaled—that is, determined by the dynamics of the body in motion (Fath & Fajen, 2011; Franchak & Adolph, 2013; Franchak et al., 2012; Warren, 1984). If so, experience may play a larger role in perceptual–motor recalibration than has previously been thought.
References
Abrams, B., Carmichael, S., & Selvin, S. (1995). Factors associated with the pattern of maternal weight gain during pregnancy. Obstetrics and Gynecology, 86, 170–176.
Adolph, K. E. (2008). The growing body in action: What infant locomotion tells us about perceptually guided action. In R. Klatzy, M. Behrmann, & B. MacWhinney (Eds.), Embodiment, ego-space, and action (pp. 275–321). Mahwah, NJ: Erlbaum.
Adolph, K. E., & Joh, A. S. (2009). Multiple learning mechanisms in the development of action. In A. Woodward & A. Needham (Eds.), Learning and the infant mind (pp. 172–207). New York, NY: Oxford University Press.
Bingham, G. P., & Pagano, C. C. (1998). The necessity of a perception–action approach to definite distance perception: Monocular distance perception to guide reaching. Journal of Experimental Psychology: Human Perception and Performance, 24, 145–168.
Bird, A. R., Menz, H. B., & Hyde, C. C. (1999). The effect of pregnancy on footprint parameters. A prospective investigation. Journal of the American Podiatric Medical Association, 89, 405–409.
Bracero, L. A., & Byrne, D. W. (1998). Optimal maternal weight gain during singleton pregnancy. Gynecologic and Obstetric Investigation, 46, 9–16.
Butler, E. E., Colon, I., Druzin, M. L., & Rose, J. (2006). Postural equilibrium during pregnancy: Decreased stability with and increased reliance on visual cues. American Journal of Obstetrics and Gynecology, 195, 1104–1108.
Carmichael, S., Abrams, B., & Selvin, S. (1997). The pattern of maternal weight gain in women with good pregnancy outcomes. American Journal of Public Health, 87, 1984–1988.
Cole, W. G., Chan, G. L. Y., & Adolph, K. E. (2013). Perceiving affordances for different motor skills. Experimental Brain Research, 225, 309–319.
Comalli, D. M., Franchak, J. M., Char, A., & Adolph, K. E. (2013). Ledge and wedge: Younger and older adults’ perception of action possibilities. Experimental Brain Research, 228, 183–192. doi:10.1007/s00221-013-3550-0
Dunning, K., LeMasters, G., Levin, L., Bhattacharya, A., Alterman, T., & Lordo, K. (2003). Falls in workers during pregnancy: Risk factors, job hazards, and high risk occupations. American Journal of Industrial Medicine, 44, 664–672.
Fath, A. J., & Fajen, B. R. (2011). Static and dynamic visual information about the size and passability of an aperture. Perception, 40, 887–904.
Foti, T., Davids, J. R., & Bagley, A. (2000). A biomechanical analysis of gait during pregnancy. Journal of Bone and Joint Surgery, 82, 625–632.
Franchak, J. M., & Adolph, K. E. (2012). What infants know and what they do: Perceiving possibilities for walking through openings. Developmental Psychology, 48, 1254–1261.
Franchak, J. M., & Adolph, K. E. (2013). Affordances for action as probabilstic functions: Implications for development, perception, and decision-making. Ecological Psychology, (in press).
Franchak, J. M., Celano, E. C., & Adolph, K. E. (2012). Perception of passage through openings cannot be explained geometric body dimensions alone. Experimental Brain Research, 223, 301–310.
Franchak, J. M., van der Zalm, D., & Adolph, K. E. (2010). Learning by doing: Action performance facilitates affordance perception. Vision Research, 50, 2758–2765.
Fries, E. C., & Hellebrandt, F. A. (1943). The influence of pregnancy on the location of the center of gravity, postural stability, and body alignment. American Journal of Obstetrics and Gynecology, 46, 374–380.
Gibson, J. J. (1979). The ecological approach to visual perception. Boston, MA: Houghton Mifflin.
Higuchi, T., Cinelli, M. E., Greig, M. A., & Patla, A. E. (2006). Locomotion through apertures when wider space for locomotion is necessary: Adaptation to artificially altered bodily states. Experimental Brain Research, 175, 50–59.
Higuchi, T., Murai, G., Kijima, A., Seya, Y., Wagman, J. B., & Imanaka, K. (2011). Athletic experience influences shoulder rotations when running through apertures. Human Movement Science, 30, 534–549.
Higuchi, T., Takada, H., Matsuura, Y., & Imanaka, K. (2004). Visual estimation of spatial requirements for locomotion in novice wheelchair users. Journal of Experimental Psychology: Applied, 10, 55–66.
Ishak, S., Adolph, K. E., & Lin, G. C. (2008). Perceiving affordances for fitting through apertures. Journal of Experimental Psychology: Human Perception and Performance, 34, 1501–1514. doi:10.1037/a0011393
Jensen, R. K., Doucet, S., & Treitz, T. (1996). Changes in segment mass and mass distribution during pregnancy. Journal of Biomechanics, 29, 251–256.
Joh, A. S., & Adolph, K. E. (2006). Learning from falling. Child Development, 77, 89–102.
Joh, A. S., Adolph, K. E., Campbell, M. R., & Eppler, M. A. (2006). Why walkers slip: Shine is not a reliable cue for slippery ground. Perception & Psychophysics, 68, 339–352. doi:10.3758/BF03193681
Joh, A. S., Adolph, K. E., Narayanan, P. J., & Dietz, V. A. (2007). Gauging possibilities for action based on friction underfoot. Journal of Experimental Psychology: Human Perception and Performance, 33, 1145–1157. doi:10.1037/0096-1523.33.5.1145
Mark, L. S. (1987). Eyeheight-scaled information about affordances: A study of sitting and stair climbing. Journal of Experimental Psychology: Human Perception and Performance, 13, 361–370. doi:10.1037/0096-1523.13.3.361
Mark, L. S., Baillet, J. A., Craver, K. D., Douglas, S. D., & Fox, T. (1990). What an actor must do in order to perceive the affordance for sitting. Ecological Psychology, 2, 325–366.
Murkoff, H., & Mazel, M. (2008). What to expect when you’re expecting (4th ed.). New York, NY: Workman.
Soltani, H., & Fraser, R. B. (2000). A longitudinal study of maternal anthropometric changes in normal weight, overweight and obese women during pregnancy and postpartum. British Journal of Nutrition, 84, 95–101.
Stefanucci, J. K., & Geuss, M. N. (2010). Duck! Scaling the height of a horizontal barrier to body height. Attention, Perception, & Psychophysics, 72, 1338–1349. doi:10.3758/APP.72.5.1338
Stoffregen, T. A., Yang, C., & Bardy, B. G. (2005). Affordance judgments and nonlocomotor body movement. Ecological Psychology, 17, 75–104.
Stoffregen, T. A., Yang, C., Giveans, M. R., Flanagan, M., & Bardy, B. G. (2009). Movement in the perception of an affordance for wheelchair locomotion. Ecological Psychology, 21, 1–36.
US Institute of Medicine, Committee on Nutritional Status During Pregnancy and Lactation. (1990). Nutrition during pregnancy: Part I, Weight gain. Washington, DC: National Academies Press.
Wagman, J. B., & Taylor, K. K. R. (2005). Perceiving affordances for aperture crossing for the person-plus-object system. Ecological Psychology, 17, 105–130.
Warren, W. H. (1984). Perceiving affordances: Visual guidance of stair climbing. Journal of Experimental Psychology: Human Perception and Performance, 10, 683–703. doi:10.1037/0096-1523.10.5.683
Warren, W. H., & Whang, S. (1987). Visual guidance of walking through apertures: Body-scaled information for affordances. Journal of Experimental Psychology: Human Perception and Performance, 13, 371–383.
Whitcome, K. K., Shapiro, L. J., & Lieberman, D. E. (2007). Fetal load and the evolution of lumbar lordosis in bipedal hominins. Nature, 450, 1075–1078.
Wichmann, F. A., & Hill, N. J. (2001). The psychometric function: II. Bootstrap-based confidence intervals and sampling. Perception & Psychophysics, 63, 1314–1329. doi:10.3758/BF03194545
Wilmut, K., & Barnett, A. L. (2010). Locomotor adjustments when navigating through apertures. Human Movement Science, 29, 289–298.
Withagen, R., & Michaels, C. F. (2005). The role of feedback information for calibration and attunement in perceiving length by dynamic touch. Journal of Experimental Psychology: Human Perception and Performance, 31, 1379–1390.
Wu, W., Meijer, O. G., Lamoth, C. J., Uegaki, K., van Dieën, J. H., Wuisman, P. I., … Beek, P. J. (2004). Gait coordination in pregnancy: Transverse pelvic and thoracic rotations and their relative phase. Clinical Biomechanics, 19, 480–488.
Yu, Y., Bardy, B. G., & Stoffregen, T. A. (2011). Influences of head and torso movement before and during affordance perception. Journal of Motor Behavior, 43, 45–53.
Author note
This research was supported by National Institute of Health and Human Development Grant No. R37-HD33486 to K.E.A. Portions of this work were presented at the 2007 meeting of the Vision Sciences Society and the 2009 International Conference on Perception and Action. We gratefully acknowledge the members of the NYU Infant Action Lab for their help collecting the data and for providing comments on the manuscript. We thank Gladys Chan for her beautiful line drawings, and Scott R. Robinson for suggesting the title.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Franchak, J.M., Adolph, K.E. Gut estimates: Pregnant women adapt to changing possibilities for squeezing through doorways. Atten Percept Psychophys 76, 460–472 (2014). https://doi.org/10.3758/s13414-013-0578-y
Published:
Issue Date:
DOI: https://doi.org/10.3758/s13414-013-0578-y