
Abstract
Background
The effect of increasing negative margin width after breast-conserving therapy (BCT) on local recurrence (LR) is controversial. LR rates vary by subtype, with the highest rates seen in triple-negative breast cancer (TNBC). This study examined LR rates in relationship to margin width in TNBC treated with BCT.
Methods
Women with TNBC who underwent BCT between 1999 and 2009 were identified. Margins were defined as positive (ink on tumor), 0.1–2.0, and 2 mm. Patients with positive margins were excluded. Statistical comparisons were by t test, Fisher’s exact test, and Wilcoxon rank sum test. Cumulative incidence of LR was compared by competing-risks methodology.
Results
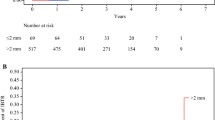
Of 535 cancers, 71 had margins ≤2 mm and 464 had margins >2 mm. At a median follow-up of 84 months (range 8–165 months), there were 37 local, 18 regional, and 77 distant recurrences or deaths as first events. Ten patients had a locoregional recurrence before planned radiotherapy and were excluded from cumulative incidence analyses. The cumulative incidence of LR at 60 months for margins ≤2 mm was 4.7 % (95 % confidence interval 0–10.0) and for >2 mm was 3.7 % (1.8, 5.5) (p = 0.11). After controlling for chemotherapy and tumor size, there was no difference in LR between the two margin groups (p = 0.06). A difference in the risk of distant recurrence or death was not observed (p = 0.53).
Conclusions
Margin width of >2 mm was not associated with reduced LR rates. These data support a negative margin definition of no ink on tumor, even in this high-risk TNBC cohort.


Similar content being viewed by others


References
Clarke M, Collins R, Darby S, et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;366(9503):2087–106.
Bouganim N, Tsvetkova E, Clemons M, et al. Evolution of sites of recurrence after early breast cancer over the last 20 years: implications for patient care and future research. Breast Cancer Res Treat. 2013;139:603–6.
Singletary SE. Surgical margins in patients with early-stage breast cancer treated with breast conservation therapy. Am J Surg. 2002;184:383–93.
Azu M, Abrahamse P, Katz SJ, et al. What is an adequate margin for breast-conserving surgery? Surgeon attitudes and correlates. Ann Surg Oncol. 2010;17:558–63.
Lovrics PJ, Gordon M, Cornacchi SD, et al. Practice patterns and perceptions of margin status for breast conserving surgery for breast carcinoma: National Survey of Canadian General Surgeons. Breast. 2012;21:730–4.
Hassani A, Griffith C, Harvey J. Size does matter: High volume breast surgeons accept smaller excision margins for wide local excision—a national survey of the surgical management of wide local excision margins in UK breast cancer patients. Breast. 2013;22:718–22.
Houssami N, Macaskill P, Marinovich ML, et al. Meta-analysis of the impact of surgical margins on local recurrence in women with early-stage invasive breast cancer treated with breast-conserving therapy. Eur J Cancer. 2010;46:3219–32.
Lowery AJ, Kell MR, Glynn RW, et al. Locoregional recurrence after breast cancer surgery: a systematic review by receptor phenotype. Breast Cancer Res Treat. 2012;133:831–41.
Groot G, Rees H, Pahwa P, et al. Predicting local recurrence following breast-conserving therapy for early stage breast cancer: the significance of a narrow (</=2 mm) surgical resection margin. J Surg Oncol. 2011;103:212–6.
Chen W, Stroom J, Sonke JJ, et al. Impact of negative margin width on local recurrence in breast conserving therapy. Radiother Oncol. 2012;104:148–54.
Hattangadi-Gluth JA, Wo JY, Nguyen PL, et al. Basal subtype of invasive breast cancer is associated with a higher risk of true recurrence after conventional breast-conserving therapy. Int J Radiat Oncol Biol Phys. 2012;82:1185–91.
Panoff JE, Hurley J, Takita C, et al. Risk of locoregional recurrence by receptor status in breast cancer patients receiving modern systemic therapy and post-mastectomy radiation. Breast Cancer Res Treat. 2011;128:899–906.
Kim MM, Dawood S, Allen P, et al. Hormone receptor status influences the locoregional benefit of trastuzumab in patients with nonmetastatic breast cancer. Cancer. 2012;118:4936–43.
Russo AL, Arvold ND, Niemierko A, et al. Margin status and the risk of local recurrence in patients with early-stage breast cancer treated with breast-conserving therapy. Breast Cancer Res Treat. 2013;140:353–61.
Fisher B, Dignam J, Bryant J, et al. Five versus more than five years of tamoxifen therapy for breast cancer patients with negative lymph nodes and estrogen receptor-positive tumors. J Natl Cancer Inst. 1996;88:1529–42.
Fisher B, Dignam J, Mamounas EP, et al. Sequential methotrexate and fluorouracil for the treatment of node-negative breast cancer patients with estrogen receptor–negative tumors: eight-year results from National Surgical Adjuvant Breast and Bowel Project (NSABP) B-13 and first report of findings from NSABP B-19 comparing methotrexate and fluorouracil with conventional cyclophosphamide, methotrexate, and fluorouracil. J Clin Oncol. 1996;14:1982–92.
Romond EH, Perez EA, Bryant J, et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med. 2005;353:1673–84.
Dahabreh IJ, Linardou H, Siannis F, et al. Trastuzumab in the adjuvant treatment of early-stage breast cancer: a systematic review and meta-analysis of randomized controlled trials. Oncologist. 2008;13:620–30.
Adkins FC, Gonzalez-Angulo AM, Lei X, et al. Triple-negative breast cancer is not a contraindication for breast conservation. Ann Surg Oncol. 2011;18:3164–73.
Parker CC, Ampil F, Burton G, et al. Is breast conservation therapy a viable option for patients with triple-receptor negative breast cancer? Surgery. 2010;148:386–91.
Zumsteg ZS, Morrow M, Arnold B, et al. Breast-conserving therapy achieves locoregional outcomes comparable to mastectomy in women with T1–2N0 triple-negative breast cancer. Ann Surg Oncol. 2013;20:3469–76.
Morrow M, Jagsi R, Alderman AK, et al. Surgeon recommendations and receipt of mastectomy for treatment of breast cancer. JAMA. 2009;302:1551–6.
McCahill LE, Single RM, Aiello Bowles EJ, et al. Variability in reexcision following breast conservation surgery. JAMA. 2012;307:467–75.
Al-Ghazal SK, Blamey RW, Stewart J, et al. The cosmetic outcome in early breast cancer treated with breast conservation. Eur J Surg Oncol. 1999;25:566–70.
Dent R, Trudeau M, Pritchard KI, et al. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res. 2007;13(15 Pt 1):4429–34.
Pogoda K, Niwinska A, Murawska M, et al. Analysis of pattern, time and risk factors influencing recurrence in triple-negative breast cancer patients. Med Oncol. 2013;30:388.
Acknowledgment
This study was funded in part through NIH/NCI Cancer Center Support grant P30 CA008748.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pilewskie, M., Ho, A., Orell, E. et al. Effect of Margin Width on Local Recurrence in Triple-Negative Breast Cancer Patients Treated with Breast-Conserving Therapy. Ann Surg Oncol 21, 1209–1214 (2014). https://doi.org/10.1245/s10434-013-3416-5
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-013-3416-5