
Abstract
Background
Researches to detect the ideal agent for pleurodesis are still continuous; iodopovidone is one of the best agents for pleurodesis that are commonly used. Tranexamic acid is also considered by many authors as a safe, cheap, and effective agent for pleurodesis.
Results
Group I (patients subjected to pleurodesis using tranexamic acid) had a higher complete response with a success rate 88% compared with 76% for group II (patients subjected to pleurodesis using iodopovidone) at the end of the study in 12 weeks. Complications were nearly equal in both groups. Chest pain, hypotension, and fever were the most common reported complications.
Conclusions
Tranexamic acid and iodopovidone were found to be effective alternative agents for pleurodesis with low cost and minimal complications.
Similar content being viewed by others

Background
Pleural effusion is the most common manifestation of pleural diseases with different etiologies ranging from cardiopulmonary disorders to inflammatory or malignant diseases [1]. Lung and breast cancer account for 75% of malignant pleural effusions, and 10% occurs with massive effusion with complete opacification of the hemi-thorax requiring urgent evaluation and treatment [2].
Chest tube thoracotomy is still the treatment of choice for pneumothorax and effusions [3], but it is considered an invasive procedure with potential morbidity and mortality thus the use of pigtail catheter can be considered [4].
Chemical pleurodesis is reported as the best treatment for recurrent pleural effusions when the underlying cause cannot be corrected. A large number of pleural irritants had been tried, but the research to detect the ideal, effective, safe, inexpensive, and readily available agent for pleurodesis is still continuous. Talc is one of the most commonly used agents, as it is highly effective and widely available [5, 6]. However, systemic embolization of talc has been reported, so there are serious concerns about its safety. Sclerosing agents such as tranexamic acid and iodopovidone were used for obliteration of the pleural cavity and cessation of the process of exudation. They are effective, safe, cheap, and readily available [7, 8].
Aim of the work
Evaluation of efficacy (success rate), safety (side effects), and tolerability of tranexamic acid and iodopovidone as chemical agents for pleurodesis, in the management of recurrent pleural effusion using pigtail catheter.
Methods
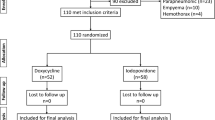
This prospective randomized study included 50 patients with unilateral recurrent pleural effusion of different etiologies divided into 2 equal groups.
Group I: Included 25 patients subjected to pleurodesis using tranexamic acid.
Group II: Included 25 patients subjected to pleurodesis using iodopovidone.
The study was done in Chest Department, Tanta University Hospital during the period from May 2016 to April 2017.
Inclusion criteria
Moderate to large amount of unilateral recurrent pleural effusion, cooperative patient, hemodynamic stability with no bleeding, or coagulation disorders.
Exclusion criteria
Complicated para-pneumonic effusions or frank empyema, patients with encysted pleural effusions.
Method of the study
All patients included in the study were subjected to complete history taking, general, and local examination, routine laboratory investigation, and diagnostic thoracocentesis, radiographic evaluation by plain chest X-rays (PA and lateral views), CT chest and chest ultrasound when needed, small-bore pigtail catheter was inserted percutaneously under local anesthesia, pleurodesis, once the pigtail in the pleural space drained 150 ml or less per day with full lung expansion confirmed by chest X-ray, injection of pleurodesis solutions was done as follows:
Group I: 4 ampules (Kapron, Amoun Company) including 500 mg tranexamic acid for each, diluted in 50 ml of normal saline solution, and 10 ml of 2% lidocaine were injected intra-pleural via pigtail catheter [7].
Group II: 20 ml of 10% povidone iodine (Betadine, Mundi-pharma Company), diluted in 80 ml of saline solution and 10 ml of 2% lidocaine were injected intra-pleural via pigtail catheter [8].
The catheter was clamped for 6 h during which the patient was turned in all directions, supine, prone, right, left lateral decubitus, and sitting position so pleurodesis solution came in contact with all pleural surfaces [8].
Complete response is defined as a symptomatic improvement of dyspnea with complete radiographic resolution of the pleural effusion, partial response as symptomatic improvement with radiological recurrence of pleural effusion that did not require additional thoracentesis treatment failure is defined as recurrent pleural effusion that required thoracentesis [9].
Follow up: The patients were followed up at 2 weeks intervals clinically and radiologically for 12 weeks
Statistical analysis
Data analysis using IBM SPSS software package (version 20)
Results
The mean age of patients in group I was 55.68 ± 11.14 years, and in group II was of 59.80 ± 7.70 years with no statistically significant difference (Table 1).
Dyspnea and chest pain were the common complaint. The majority of effusions were right sided (64.0% in group I) and (72.0% in group II). Three mesothelioma patients were non-dyspneic but suffer from severe agonizing chest pain requiring pleurodesis (Tables 2 and 3). The underlying pathologies of pleural effusion in the studied groups revealed that 24 patients had pleural effusion due to isolated hepatic hydrothorax without ascites or with mild ascites (10 in group I and 14 in group II), and 26 patients had malignant pleural effusion (15 in group I and 11 in group II). Metastatic breast cancer was the commonest cause of malignant pleural effusion followed by metastatic lung cancer and metastatic ovarian carcinoma (Table 4).
Regarding the size of the pigtail catheter used in research, significant increase in favor to the 12 French sizes in each group (96% in group I and 84% in group II ) (Table 5).
There were no significant differences between the 2 studied groups as regards to the period of placement of pigtail catheter prior to as well as after pleurodesis (Table 6).
The final follow-up of pleurodesis in both groups showed that the success rate was more in group I than group II (88.0% vs 76.0%) (Table 7).
Minor complications were founded with tranexamic acid pleurodesis as hypotension in 12%, pleuritic chest pain in 8%, shock and fever in 4%. While in iodopovidone pleurodesis, pleuritic chest pain in 12%, hypotension in 8%, empyema, fever, and shock in 4% (Table 8).
Discussion
Management of recurrent pleural effusions is considered one of the most difficult medical problems. Symptoms are caused by fluid which re-accumulates rapidly after aspiration [10]. Survival of patients with malignant pleural effusion may extend for months or even years. Therefore, the aim of treatment should be directed to relieve the distress and improve the quality of life of those patients besides the management of the primary disease [7].
The repeated aspiration to relieve dyspnea is both physically and psychologically traumatic to the patient and burden to the physician, so a more definitive management strategy must be undertaken to solve this problem, this strategy included tube thoracotomy, insertion of pleural catheter with or without pleurodesis, medical thoracoscopy, or video-assisted thoracoscopic surgery with pleurodesis [11].
Chemical pleurodesis is one of the most accepted treatments for recurrent pleural effusions. The choice of the best sclerosing agent, which is determined by the efficacy, safety, accessibility of the agent, its cost, ease of administration, and the number of administrations to achieve complete response [12].
In the present study, 50 patients were subjected to thorough investigations and they were classified into 2 equal groups 25 patients for each. The origin of effusion in group I was malignant pleural effusion in 15 patients (60%) and hepatic hydrothorax in 10 patients (40%), and in group II was malignant pleural effusion in 11 patients (44%) and hepatic hydrothorax in 14 patients (56%) as seen in Table 4. Hepatic hydrothorax as well as malignant pleural effusion is recurrent and rapidly accumulative, so many clinicians are convinced to place indwelling pleural catheters (IPCs) for non-malignant effusions like hepatic hydrothorax, sometimes spontaneous mechanical pleurodesis occurs, sometimes chemical pleurodesis with sclerosing agent is needed [13,14,15,16,17,18,19,20].
In this study, as regard the size of pigtail catheter, different diameters were used (10 F, 12 F, and 14 F) with a significant increase in favor to the 12 French sizes in each group (96% in group I and 84% in group II) as seen in Table 5. This size was the most available in market at the time of the research.
Shoji T et al. [11] continue to support the use of small-bore chest drainage and sclerotherapy, although there was no significant difference between large and small-bore catheter. Agarwal et al. [8] and Aziz et al. [21] concluded that the use of standard size pigtail catheters (8.5 F) is usually very successful in draining the pleural fluid, less time consumption, lower cost, and bedside technique makes it superior to the conventional chest tube.
In our study, pleurodesis was performed when the daily drainage volume was less than 150 ml/day, X-ray chest was done to make sure that no pleural fluid was left and the underlying lung was re-expanded. In accordance to our research, Martinez et al. [22] mentioned that pleurodesis is performed after radiographical confirmation of complete lung re-expansion. Also Shoji T et al. [11] made pleurodesis when chest tube fluid drainage decreased to less than 150 ml/day and the lung was fully re-expanded on chest X-ray.
In this study, as regard days of placement of pigtail after pleurodesis, the mean durations of the inserted tube post pleurodesis were 1.20 in group I, and 1.0 in group II, as seen in Table 6. Heffner et al. [23] showed that the chest tubes were removed from most patients when drainage of pleural fluid decreased to less than 100 ml/day after pleurodesis. In other patients, the chest tube was routinely removed several hours after instillation of doxycyline. Tomlinson and Sahn [24] said that the chest drain is usually left in position for 24-72 h, but it may be left longer if the drainage of fluid continues.
On a search for the cheapest and most available sclerosing agent with the least side effects, the present study aimed to evaluate the effectiveness of tranexamic acid and iodopovidone as chemical agents for pleurodesis in recurrent pleural effusion.
In group 1, we used 4 ampules (2000 mg of tranexamic acid) for each patient and the patients were followed up at 2 weeks intervals for 12 weeks, 22 patients showed complete response with a success rate of 88%, and 3 patients (12%) show failure of pleurodesis, the first case was malignant mesothelioma which failed due to failure of lung expansion and thickening of the pleura as shown by CT chest, and the other two cases were hepatic hydrothorax (Figs. 1 and 2).

a Plain chest X-ray PA view showing massive right-sided pleural effusion before drainage. b Plain chest X-ray PA view showing evacuation of the effusion with the pigtail pleural catheter seen in place. c Plain chest X-ray PA view showing complete evacuation of the effusion after pleurodesis by iodopovidone (case 1)

a Plain chest X-ray PA view showing massive left-sided pleural effusion before drainage. b Plain chest X-ray PA view showing evacuation of the effusion with the pigtail pleural catheter seen in place. c Plain chest X-ray PA view showing complete evacuation of the effusion after pleurodesis by tranexamic acid (case 2)
The success rate in the present study was higher than Eman et al. [25] study, as they achieved a success rate of 73.5%, but lower than EL-Bouhi et al. [7], as the success rate was 90%, their higher success rate may be due to higher dose used which was 10 ampoules (5000 mg of tranexamic acid).
The results in the present study were higher than the results of most of the other studies that use other chemical agent for pleurodesis. For example, Zimmer et al. [26] found a success rate of 65% on using bleomycin for pleurodesis, and Martínez et al. [22] achieved a success rate of 60-80% on using tetracycline for pleurodesis.
In our study, minor complications were founded with tranexamic acid pleurodesis as seen in Table 8 as hypotension in 12%, pleuritic chest pain in 8%, shock and fever in 4%.
In a study done by Bediwy and Galal [27], who investigated pigtail catheter insertion for draining pleural effusions of different etiologies. They evaluated success and complications of pigtail catheter insertion in 51 cases of pleural effusion. They recorded complications including chest pain at the site of insertion requiring analgesia (45.09), pneumothorax (19.6), blockade of the catheter (3.92), and infection (1.96). Blockade of the catheters and infection were associated with procedure failure.
The reported complications with different sclerosing agents are chest pain, fever, and cough, as seen in Janssen et al. [28].
In group II, we used 20 ml of 10% povidone iodine, diluted in 80 ml of saline solution and 10 ml of debocaine 2%. Regarding the doses of the pleurodetic agent, our study agreed with Agarwal et al. [8], who recommended the utilization of 20 ml of 10% iodo-povidone mixed with 80 ml normal saline solution.
In our study, the patients were followed up for12 weeks, 19 patients showed complete response, (the success rate 76%), and 6 patients show failure of pleurodesis (24%). The causes of failure in the first case were due to secondary bacterial infection and empyema, and intercostal tube was inserted via thoracoscope to drain the pus from the pleural space. Two cases were hepatic hydrothorax which failed due to massive transudative effusion due to loss of protein and fluid accumulate rapidly, one case showed accidental dislodgment of pigtail catheter, and two cases were malignant effusion.
These results were consistent with those of Carlos and his colleagues [29], who found that iodopovidone is one of the best sclerosing agents in recurrent effusions regardless the etiology, as it is effective, safe, inexpensive, and readily available. In 2004, Shaw and Agarwal [30] meta-analysis observational studies on the success rate and safety of chemical pleurodesis using iodopovidone revealed that its success rate ranged from 64.2 to 100%, with an overall success rate of 90.6%.
These results agreed with those of Ritesh et al. [31] who studied efficacy and safety of iodopovidone as a chemical pleurodesis for variety of indications in 256 patients, which included pleural effusions (157 patients), and pneumothorax (108 patients). The pleural effusions were mainly malignant effusions, and the pneumothorax was spontaneous, both primary (where the underlying lung is healthy) and secondary (where the pneumothorax occurs as a complication of some underlying pulmonary disease). There were no deaths related to chemical pleurodesis with iodopovidone.
Our results were consistent with those studies done by Dey et al. [32], who studied 38 patients with symptomatic malignant or recurrent pleural effusion and pneumothorax, had pleurodesis using iodopovidone. A complete response with no recurrence during follow-up was obtained in 34 patients (89.5%), and failure in 4 cases (10.5%) all failed cases had malignant pleural effusion.
In this work, minor complications were founded in iodopovidone pleurodesis as pleuritic chest pain (12%), hypotention (8%), empyema, fever and shock (4%), as seen in Table 8.
In a study done by Mohsen et al. [33] to compare the success, safety, and outcome of thoracoscopic talc poudrage (TTP) versus povidone iodine pleurodesis (PIP) through a thoracostomy tube in management of malignant pleural effusion due to metastatic breast cancer. Twenty-two received talc poudrage and 20 patients received pleurodesis by instilling povidone iodine through a thoracostomy tube. Talc was associated with severe pleuritic chest pain, fever, and longer hospital stay. Both groups achieved good symptom control.
Das et al. [34] reported that povidone iodine is equally effective and safe as talc, and may be preferred because of easy availability, low cost, and it can be used for recurrent pleural effusions. While in Helmy et al. [35] study, 20 patients with hepatic hydrothorax had pleurodesis using povoiodine in 8 patients, vibramycin in 6 patients, and talc slurry in other 6 patients. The outcome revealed that chemical pleurodesis was effective in the treatment of hepatic hydrothorax in 15/20 patients (75%), the success rate was 87.5% in patients treated by iodopovidone, 66.7% in vibramycin, and 66.7% in patients treated with talc slurry. However, a single case treated by talc slurry died of hepatocellular insufficiency 14 days following the procedure.
Conclusions
We concluded that tranexamic acid and iodopovidone were found to be an effective alternative agent for pleurodesis with low cost and minimal complications.
We recommend wider use of these cheap sclerosing agents instead of the costly one with the same results.
Availability of data and materials
All data generated or analyzed during this study are included in this published article [and its supplementary information files].
References
Diaz-Guzman E, Dweik RA (2007) Diagnosis and management of pleural effusions: a practical approach. ComprTher 33(4):237–246
Khaleeq G, Musani AI (2008 Jul) Emerging paradigms in the management of malignant pleural effusions. Respir Med 102(7):939–948
Munnell ER (1997) Thoracic drainage. Annals of Thoracic Surgery 63(5):1497–1502
Roberts JS, Bratton SL (1998 Oct) and BroganTV. Efficacy and complications of percutaneous pigtail catheters for thoracostomy in pediatric patients. Chest 114(4):1116–1121
Kalomenidis I (2011 Oct) Beyond talc pleurodesis: do we really need new methods? Respirology 16(7):1020–1022
Diacon AH, Wyser C, Bolliger CT, Tamm M, Pless M, Perruchoud AP et al (2000) Prospective randomized comparison of thoracoscopic talc poudrage under local anesthesia versus bleomycin instillation for pleurodesis in malignant pleural effusions. Am J Respir Crit Care Med 162:1445–1449
El-Bouhi M, El-Naggar T, Mansour M (2000) Pleurodesis with tranexamic acid. The Egyptian Journal of Chest Diseaes and Tuberculosis. 49:15–18
Agarwal R, Aggarwal AN, Gupta D (2006) Efficacy and safety of iodopovidone pleurodesis through tube thoracostomy. Respirology. 11(1):105–108
Stefani A, Natali P, Casali C, Morandi U (2006) Talc poudrage versus talc slurry in the treatment of malignant pleural effusion. A prospective comparative study. Eur J Cardiothorac Surg 30(6):827–832
Lee YC, Baumann MH, Maskell NA, Waterer GW, Eaton TE, Davies RJ et al (2003) Pleurodesis practice for malignant pleural effusions in five English-speaking countries. Chest 124(6):2229–2238
Shoji T, Tanaka F, Yanagihara K, Inui K, Wada H (2002) Phase II study of repeated intrapleural chemotherapy using implantable access system for management of malignant pleural effusion. Chest 121(3):821–824
Walker Renad PB, Vaughan LM, Sahn SA (1994) Chemical pleurodesis for treatment of malignant pleural effusions. Ann Intern Med 120(1):56–64
Goergen N, Strickland J, Buchan K (2019) Decompressive talc pleurodesis for hepatic hydrothorax. Br J Hosp Med (Lond) 80(8):480–481
Hou F, Qi X, Guo X (2016 Nov) Effectiveness and safety of pleurodesis for hepatic hydrothorax: a systematic review and meta-analysis. Dig Dis Sci 61(11):3321–3334
Chaaban T, Kanj N, Bou AI (2019 Aug) Hepatic hydrothorax: an updated review on a challenging disease. Lung. 197(4):399–405
Ortega Quiroz RJ, Moscote Granadillo M, Díaz Hernández A, Spath Spath A, Rodríguez María R, Reyes Romero A et al (2019) Hepatic hydrothorax: presentation of 3 cases with different therapeutic approaches. Rev Gastroenterol Peru. 39(1):64–69
Aboudara M, Maldonado F. Indwelling pleural catheters for benign pleural effusions: what is the evidence? .Curr Opin Pulm Med. 2019 Jul;25(4):369-373.Baig
MA MMB, Attar BM, Khan Z, Demetria M, Gandhi SR (2018 Aug 6) Efficacy and safety of indwelling pleural catheters in management of hepatic hydrothorax: a systematic review of literature. Cureus 10(8):e3110
Shojaee S, Rahman N, Haas K, Kern R, Leise M, Alnijoumi M et al (2019 Mar) Indwelling tunneled pleural catheters for refractory hepatic hydrothorax in patients with cirrhosis: a multicenter study. Chest. 155(3):546–553
Sharaf-Eldin M, Bediwy AS, Kobtan A, Abd-Elsalam S, El-Kalla F, Mansour L et al (2016) Pigtail catheter: a less invasive option for pleural drainage in Egyptian patients with recurrent hepatic hydrothorax. Gastroenterol Res Pract.:4013052
Aziz F, Penupolu S, Flores D (2012) Efficacy of percutaneous pigtail catheters for thoracostomy at bedside. J Thorac Dis. 4(3):292–295
Martínez-Moragón E, Aparicio J, Rogado MC, Sanchis J, Sanchis F, Gil-Suay V (1997) Pleurodesis in malignant pleural effusions: a randomized study of tetracycline versus bleomycin. Eur Respir J 10(10):2380–2383
Heffner JE, Standerfer RJ, Torstveit J, Unruh L (1994) Clinical efficacy of doxycycline for pleurodesis. CHEST 105(6):1743–1747
Tomlinson JR, Sahn SA (2009) Treatment of pleural effusion. Chest 89(3):470–477
Mohammed E, Eisa S, Abdelghaffar N (2015) Efficacy of tranexamic acid as pleurodesis agent in malignant pleural effusion. Egyptian Journal of Chest Diseases and Tuberculosis 64(3):587–591
Zimmer PW, Hill M, Casey K, Harvey E, Low DE (1997) Prospective randomized trial of talc slurry versus bleomycin in pleurodesis for symptomatic malignant pleural effusions. Chest 112(2):430–443
Bediwy AS, Galal HA (2012) Pigtail catheter use for draining pleural effusions of various etiologies. Pulmonolgy 12:6–12
Janssen JP, Collier G, Astoul P, Tassi GF, Noppen M, Rodriguez-Panadero F et al (2007) Safety of pleurodesis with talc poudrage in malignant pleural effusion: a prospective cohort study. Lancet 369(9572):1535–1539
Carlos A, Rafael L, Alberto R (2003 April) Iodopovidone pleurodesis for recurrent pleural effusions. Chest 123:1318–1319
Shaw P, Agarwal R (2004) Pleurodesis for malignant pleural effusions. Cochrane Database Sys Rev 1:CD002916
Ritesh Agarwal, Aggarwal AN, Gupta D, and Jindal SK: Efficacy and safety of iodopovidone in chemical pleurodes Chest 2006; 100(11) 2043–7.
Dey A, Bhuniya S, Datta Chaudhuri A, Pandit S, Saha-Dutta CM, Sengupta A, Saha I (2010) Iodopovidone pleurodesis: experience of a tertiary hospital in Kolkata. Singapore Med J 51(2):163–165
Mohsen TA, Zeid A, Meshref M, Tawfeek N, Redmond K, Ananiadou OG (2011) Local iodine pleurodesis versus thoracoscopic talc insufflation in recurrent malignant pleural effusion: a prospective randomized control trial. Eur J. CardiothoracSurg 40(2):282–286
Das SK, Saha SK, Das A, Halder AK, Banerjee SN, Chakraborty M (2008) A study of comparison of efficacy and safety of talc and iodopovidone for pleurodesis of malignant pleural effusions. J. Indian Med Assoc. 106(9):590–592
Helmy N, Akl Y, Kaddah S, Hafiz HA, Makhzangy HE (2010) Egyptian experience in using chemical pleurodesis as an alternative management in refractory hepatic hydrothorax. Arch Med Sci. 6(3):336–342
Acknowledgements
Not applicable.
Funding
This study had no funding from any resource.
Author information
Authors and Affiliations
Contributions
AHA was responsible for study design and final revision ASE shared in study design and was responsible for the practical part of the research, selection of cases, data collection and statistics, manuscript preparation, editing, and reviewing. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved from the research ethics committee of the Faculty of Medicine, Tanta University, with reference number (13532). A written consent form was obtained from every patient to participate in the research work after sufficient explanation before initiating the study.
Consent for publication
All participated patients signed an informed written consent form to publish the data with respect to the privacy of patients and confidentiality of the data as patients’ names were replaced by code numbers to confirm their privacy and the results of the study were used only for scientific purpose.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Abd El Zaher, A.H., El Dib, A.S. A study of efficacy and safety of tranexamic acid versus iodopovidone in pleurodesis via pigtail catheter in management of recurrent pleural effusion. Egypt J Bronchol 14, 19 (2020). https://doi.org/10.1186/s43168-020-00016-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43168-020-00016-z