
Abstract
Background
Systemic analgesia with paracetamol and nonsteroidal anti-inflammatory drugs plus opioids as a rescue medication had reported to be better than that depend mainly on opioids for postoperative pain relief. Thoracic paravertebral block reported to provide a comparable postthoracotomy pain relief to epidural analgesia, with fewer side effects due to its unilateral effect. Thoracic paravertebral catheter can be inserted intraoperatively under direct vision during thoracic surgery (Sabanathan’s technique). This prospective randomized study was designed to evaluate the safety and efficacy of this technique with continuous infusion of lidocaine compared to systemic analgesia for postthoracotomy pain relief.
Results
Sixty-three patients were randomized to receive a continuous infusion of lidocaine in the paravertebral catheter for 3 postoperative days (thoracic paravertebral group, n = 32) or systemic analgesia (systemic analgesia group, n = 31). All patients underwent standard posterolateral thoracotomy. There were no significant differences between both groups in age, sex, side, type, and duration of operation. Pain scores measured on visual analogue scale and morphine consumption were significantly lower in thoracic paravertebral group in all postoperative days. Spirometric pulmonary functions were not reaching the preoperative values in the third postoperative day in both groups, but restorations of pulmonary functions were superior in paravertebral group. No complications could be attributed to the paravertebral catheter. Side effects, mainly nausea and vomiting followed by urinary retention, were significantly more in systemic analgesia group (P = 0.03). Also, pulmonary complications were more in systemic analgesia group but not reaching statistical significance (P = 0.14).
Conclusion
Continuous paravertebral block by direct access to the paravertebral space using a catheter inserted by the surgeon is a simple technique, with low risk of complications, provides effective pain relief with fewer side effects, and reduces the early loss of postoperative pulmonary functions when compared to systemic analgesia.
Similar content being viewed by others


Background
Postthoracotomy pain is responsible for ineffective ventilation with inability to breathe deeply and mucous plugging leading to atelectasis, hypoxia, and ventilation perfusion mismatch predisposing to pulmonary infection and pulmonary complications [1, 2]. Multiple modalities were used to provide sufficient pain control with varying success: thoracic epidural, thoracic paravertebral, intrathecal, intercostal, interpleural analgesic techniques, and systemic analgesia [2,3,4,5]. Thoracic paravertebral block provides a comparable pain relief to epidural analgesia, with less side effects due to its unilateral effect [2, 6,7,8,9]. Recently, the group of procedure specific postoperative pain management (PROSPECT) of the European society of regional anesthesia and pain therapy recommends thoracic paravertebral block (TPVB) with local anesthetics as a bolus preoperatively or at the end of the operation followed by continuous infusion as the first choice compared to thoracic epidural analgesia (TEA) as TPVB has a lower rate of complications [10]. The main disadvantage of TPVB technique is the lack of familiarity [11]. The conventional and the most commonly used technique for paravertebral block depends on loss of resistance to air technique for percutaneous insertion of the catheter that can be aided with ultrasound guidance or nerve stimulation, and this is usually done by the anesthetist [12, 13]. Thoracic paravertebral catheters can also be safely inserted with ease under direct vision during thoracic surgery by the surgeon (Sabanathan’s technique) [14,15,16].
This study was designed to evaluate the safety and efficacy of TPVB by intraoperative insertion of the catheter directly into the paravertebral space with postoperative continuous infusion of lidocaine on postthoracotomy pain as compared to systemic analgesia.
Methods
This prospective study was conducted in our center after approval from our University Institutional Research Board (IRB) and written informed consent from all patients, in the period from June 2015 to January 2020. The study was registered in ClinicalTrials.gov (ID: NCT04482192).
Inclusion criteria were the adult patients scheduled to undergo elective posterolateral thoracotomy for pulmonary procedures with American Society of Anesthesiologists (ASA) physical status of II and III and body mass index (BMI) between 25 and 35 kg/m2.
Exclusion criteria were patients younger than 18 years, emergency surgery, previous thoracotomy, drug addiction, allergy to paracetamol (acetaminophen) or ketorolac, allergy to local anesthetics used, coagulopathy, hepatic dysfunction, chronic renal failure, history of gastric ulcer or bronchial asthma, or lack of patient consent.
Randomization into two groups, thoracic paravertebral block (TPVB) group and systemic analgesia (SA) with 1:1 allocation, was done by sealed envelopes that were prepared with a computer-generated randomization.
Patient’s sample
Based on a pilot study of 20 patients, 10 in each group, the mean visual analogue scores of pain at rest (VAS) ± SD at 6 h postoperatively for TPVB patients were 3.0 ± 1.4 and that for SA patients were 4.2 ± 1.6. The calculated significant sample size with a power of 0.85 and alpha error of 0.05 was 60 patients, with 1:1 allocation in each group.
Eighty-two patients were assessed for eligibility criteria to be included in the study, 18 patients were excluded pre-randomization, and one patient was excluded post-randomization due to re-exploration for bleeding. Sixty-three patients were analyzed in the study. Thoracic paravertebral block group (TPVB group) included 32 patients, and systemic analgesia group (SA group) included 31 patients (Fig. 1).

CONSORT flow diagram
On the day before operation, patients were trained for the use of the paper-based visual analogue scale (VAS) for pain assessment. The VAS consists of a horizontal line of 10 cm long orientated from the right (0 = no pain) to the left (10 = worst pain imaginable). The patient places a mark on the line corresponding to intensity of pain. The distance between the starting point (the right end) to the patient mark, in centimeters, is recorded as his/her pain score.
Also, patients were instructed in the use of Microspiro HI-198 (Chest Corporation, Tokyo, Japan). After training, forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), and peak expiratory flow rate (PEFR), in the sitting position, were recorded in the day before surgery.
Anesthesia
Anesthetic technique was standardized for all patients. Patients were premedicated with IV injection of glycopyrrolate 0.01 mg/kg. Anesthesia was induced with intravenous 1.5–2 mg/kg propofol and fentanyl 2 μg/kg. Intravenous atracurium 0.5 mg/kg was given to facilitate tracheal intubation. Anesthesia was maintained with isoflurane 0.8–1.2% in 100% oxygen, incremental doses (0.1 mg/kg) of atracurium, and mechanical ventilation. At the end of surgical operation, neuromuscular block was reversed using IV neostigmine 2.5 mg and glycopyrrolate 0.01 mg/kg.
Technique of intraoperative paravertebral catheter insertion
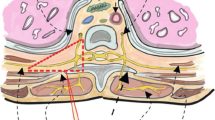
We used the technique that was described by Sabanathan et al. in 1988 [14] and modified by them in 1990 [15]. After completing the surgical pulmonary procedure and with the chest is still open, starting from the posterior end of the thoracotomy, parietal pleura is raised from the posterior chest wall to the vertebral body and for two spaces above and below the incision of thoracotomy creating a pouch. A 16-gauge disposable Tuohy needle is inserted percutaneously through a low posterior interspace. The needle is advanced until the tip appeared in the created pouch. The stylet is removed, and a 16-gauge side-holed epidural catheter is advanced into the created pouch, and the needle is withdrawn. Using a curved forceps, a small defect is done in the extrapleural fascia to be directly in the paravertebral space. The cannula is passed to the paravertebral space through the defect and advanced cranially for 2 to 3 cm. The parietal pleura is reattached to the posterior edge of the wound, and the catheter is secured. Then, a bolus dose 15–20 ml of 1% lidocaine is injected through the catheter, and the chest is closed as usual with one or two intercostal drainage tubes according to the surgical procedure.
Protocol of analgesia
All patients, in both groups, received intravenous analgesia with 1 g paracetamol and 30 mg ketorolac half an hour before the end of surgery.
Systemic analgesia (SA) group continues to receive 1 g paracetamol and 30 mg ketorolac by intravenous infusion every 6 h for 3 days. Thoracic paravertebral block (TPVB) group received continuous infusion of 0.1 ml/kg/h of 1.0% lidocaine (l mg/kg/h) using infusion pump through the inserted paravertebral catheter for 3 days. Intravenous morphine sulfate (0.05 mg/kg) was given as a rescue medication if the VAS ≥ 4 for both groups. A senior nurse was responsible for handling the analgesia regimen, and another nurse was responsible for recording pain score on visual analogue scale (VAS) and morphine consumption, as scheduled.
Objective pulmonary function
Forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), and peak expiratory flow rate (PEFR) were measured in the sitting position 24, 48, and 72 h postoperatively for all patients. Results were expressed as a percentage of the preoperative values that were done in the day before surgery.
End points
The primary end point was pain score on visual analogue scale (VAS) at rest and on coughing measured and recorded at 1, 6, 12, 24, 36, 48 h, and 72 h postoperatively. The secondary end points were total morphine consumption at the end of each postoperative day and pulmonary function tests at 24, 48, and 72 h postoperatively. Complications related to the catheter, postoperative pulmonary complications, respiratory depression (defined as respiratory rate less than 8 per min), nausea and vomiting, and urinary retention were recorded.
Statistical analysis
Continuous variables are presented as mean ± SD and categorical variables as number and percent. Continuous variables were compared using t test or Mann–Whitney test if not normally distributed, and categorical variables were compared using the chi2 test or Fischer’s Exact test if the frequency of the events is less than 5. Differences were accepted to be significant at p < 0.05. Analyses were done using IBM SPSS for Windows, Version 22.0 (IBM Corp., USA).
Results
Sixty-three adult patients included in the study, 32 in thoracic paravertebral block (TPVB) group and 31in systemic analgesia (SA) group, 36 males and 27 females. There were no significant differences between both groups regarding age, sex, ASA class, BMI, side, type, and duration of operation (Table 1).
Pain relief
Pain scores on visual analogue scale were significantly lower in TPVB group at rest and on coughing throughout the study period, indicating better pain relief in the TPVB group (Tables 2 and 3).
In addition, postoperative morphine consumption was significantly lower in TPVB group of patients in all the three postoperative days (Table 4).
Postoperative pulmonary function
In both groups, all pulmonary function tests (FVC, FEV1, and PEFR) were reduced in first postoperative day (measured 24 h postoperatively) than the preoperative values and continue to increase in the second and third days but not reaching the preoperative values at 72 h postoperatively. But, all pulmonary function tests are significantly better in TPVB group in all days (Table 5).
Complications and side effects
No complications could be attributed to the paravertebral catheter or to lidocaine. Pulmonary complications were more in SA group but without statistical significance (P = 0.14) (Table 6). Side effects were significantly more in SA group (P = 0.03). The most frequent side effects were nausea and vomiting (6 patients in SA group and 1 patient in TPVB group, P = 0.04). Urinary retentions were more in SA group but without statistical significance (P = 0.32) (Table 6).
Discussion
Postthoracotomy pain is reported as one of the most painful postoperative pain and frequently causes significant morbidity [1]. Combinations of analgesic drugs that have different mechanisms of action achieve a synergistic effect with better postoperative pain relief and fewer side effects [17]. A meta-analyses of randomized trials concluded that paracetamol (acetaminophen) in combination with a nonsteroidal anti-inflammatory drug for postoperative pain control achieved better pain relief than each drug alone, and this combination decreased opioid use [18]. According to the above concept, we used a multimodal systemic analgesia in the form paracetamol combined with ketorolac (nonsteroidal anti-inflammatory drug) plus morphine as a rescue medication for systemic (SA) analgesia group in this study.
Thoracic paravertebral space is a wedge-shaped space on both sides of vertebral column. Parietal pleura forms the anterolateral boundary of the space. Vertebrae and intervertebral foramina form its medial boundary. The space contains intercostal nerves (spinal nerves) and its posterior primary rami, the rami communicantes, and the sympathetic chain. The spinal nerves in the space formed from small bundles without enclosing fascial sheath making them highly susceptible for blockade with local anesthetics [11].. The injected local anesthetic drug in the paravertebral space diffuses cranially and caudally covering several segments resulting in unilateral somatic and sympathetic nerve block [13]. The conventional technique for TPVB is the percutaneous technique that may be aided with ultrasonic guidance or nerve stimulation with about 6 to 19% failure rate and a complication rate of 2.6 to 5% in the form of pneumothorax, vascular injury, Horner syndrome, and epidural or intrathecal spread [11]. Intraoperative insertion of the paravertebral catheter under direct vision into the paravertebral space is an alternative technique that can be done easily by the surgeon [14, 15]. Results of this study and that of many other studies [3, 14,15,16, 19,20,21,22] supported that this technique is an easy and safe and without complications related to catheter insertion.
The most commonly used local anesthetic drugs for continuous paravertebral block are bupivacaine, lidocaine, and ropivacaine. Bupivacaine and ropivacaine are long-acting local anesthetic drugs, while lidocaine is a short-acting one with a shorter half-life. So, for continuous infusion, lidocaine may be the better choice [20, 21, 23, 24]. Watson et al. [20] in a study comparing bupivacaine versus lidocaine for continuous paravertebral block after thoracotomy reported that their efficacy was equivalent with lesser risk of systemic toxicity for lidocaine. Also, Ghisi et al. [23] reported equal analgesic effect of lidocaine and ropivacaine for continuous paravertebral block, but they recommended the use of lidocaine because of its easier titratability and lower cost. As the results of this study, many investigators [16, 20, 21, 23, 24] used lidocaine for continuous paravertebral block without side effects related to the drug. Many studies [2, 4, 6, 9, 10] comparing postthoracotomy TPVB to epidural analgesia reported equivalent pain relief with lesser side effects of TPVB. TPVB is superior compared to pure intercostal nerve block in postthoracotomy pain relief as TPVB also blocks posterior primary rami and sympathetic fibers [22].
This study demonstrates significant pain relief in TPVB group compared to SA group supported by lower pain score on visual analogue scale at rest and on coughing and lesser morphine consumption. Marret et al. [25] comparing TPVB with ropivacaine to systemic analgesia and Fortier et al. [3] comparing 3 analgesic modalities (systemic analgesia, continuous wound catheter analgesia, and continuous thoracic paravertebral block with ropivacaine) demonstrated the superiority of TPVB for postthoracotomy pain relief with lesser morphine consumption as the results of our study. This study confirms the findings of other studies that there are marked alteration of pulmonary function following thoracotomy [11, 26, 27], and effective postoperative regional analgesia as thoracic paravertebral block and thoracic epidural block reduces this alteration and aids in its recovery [11, 16, 22, 24, 26]. This study recorded no significant difference in postoperative pulmonary complications between TPVB group and SA group. Nausea and vomiting were significantly more in SA group, and this is mostly due to increased morphine consumption in that group as postoperative nausea and vomiting are strongly influenced by postoperative opioid use in a dose-related manner [28, 29]. Many studies [8, 16, 22, 30] comparing TPVB with continuous local anesthetic perfusion versus intravenous or intramuscular opioids for postoperative analgesia reported better pain relief and lesser side effects in TPVB patients.
Limitations
As there were different routes of administration of analgesic drugs for each group of patients, it was very difficult to keep double blindness. Also, the number of patients can be considered as another limitation.
Conclusion
This study demonstrates that patients receiving continuous paravertebral block with lidocaine via a catheter inserted with direct access to the thoracic paravertebral space by the surgeon intraoperatively have significantly better pain relief with fewer side effects and better restoration of pulmonary functions compared to patients receiving systemic analgesia, and this technique (Sabanathan’s technique) is safe and reliable as a method for postthoracotomy analgesia.
Availability of data and materials
Data are available with the corresponding author upon request.
Abbreviations
- PROSPECT:
-
The group of procedure specific postoperative pain management
- TPVB:
-
Thoracic paravertebral block
- TEA:
-
Thoracic epidural analgesia
- ASA:
-
American Society of Anesthesiologists
- BMI:
-
Body mass index
- SA:
-
Systemic analgesia
- VAS:
-
Visual analogue score
- CONSORT:
-
Consolidated Standards of Reporting Trials
- SD:
-
Standard deviation
References
Kotze A, Scally A, Howell S (2009) Efficacy and safety of different techniques of paravertebral block for analgesia after thoracotomy: systematic review and metaregression. Br J Anaesth 103(5):626–636. https://doi.org/10.1093/bja/aep272
Joshi GP, Bonnet F, Shah R, Wilkinson RC, Camu F, Fischer B et al (2008) A systematic review of randomized trials evaluating regional techniques for postthoracotomy analgesia. Anesth Analg 107:1026–1040. https://doi.org/10.1213/ane.0b013e31817e7b40
Fortier S, Hanna HA, Bernard A, Girard C (2012) Comparison between systemic analgesia, continuous wound catheter analgesia and continuous thoracic paravertebral block: a randomised, controlled trial of postthoracotomy pain management. Eur J Anaesthesiol 29:524–530. https://doi.org/10.1097/EJA.0b013e328357e5a1
Wojtyś ME, Wąsikowski J, Wójcik N, Wójcik J, Wasilewski P, Lisowski P et al (2019) Assessment of postoperative pain management and comparison of effectiveness of pain relief treatment involving paravertebral block and thoracic epidural analgesia in patients undergoing posterolateral thoracotomy. J Cardiothorac Surg 14:78 https://doi.org/10.1186/s13019-019-0901-3
Kolettas A, Lazaridis G, Baka S, Mpoukovinas I, Karavasilis V, Kioumis I et al (2015) Postoperative pain management. J Thorac Dis 7:S62–S72. https://doi.org/10.3978/j.issn.2072-1439.2015.01.15
Krakowski JC, Arora H (2015) Con: thoracic epidural block is not superior to paravertebral blocks for open thoracic surgery. J Cardiothorac Vasc Anesth 29(6):1720-1722. https://doi.org/10.1053/j.jvca.2015.06.012. Epub 2015 Jun 10.
Casati A, Alessandrini P, Nuzzi M, Tosi M, Iotti E, Ampollini L et al (2006) A prospective, randomized, blinded comparison between continuous thoracic para-vertebral and epidural infusion of 0.2% ropivacaine after lung resection surgery. Eur J Anaesthesiol 23:999–1004. https://doi.org/10.1017/S0265021506001104
Davies RG, Myles PS, Graham JM (2006) A comparison of the analgesic efficacy and side-effects of paravertebral vs epidural blockade for thoracotomy–a systematic review and meta-analysis of randomized trials. Br J Anaesth 96:418–426. https://doi.org/10.1093/bja/ael020
Scarfe AJ, Schuhmann-Hingel S, Duncan JK, Ma N, Atukorale YN, Cameron AL (2016) Continuous paravertebral block for post-cardiothoracic surgery analgesia: a systematic review and meta-analysis. Eur J Cardiothorac Surg 50:1010–1018. https://doi.org/10.1093/ejcts/ezw168
Procedure specific postoperative pain management. (2015) Thoracotomy. http://www.esraeurope.org/prospect [Accessed 26 Jan 2020].
Rosenblatt MA, Lai Y. Thoracic nerve block techniques UpToDate Topic 100071 Version 24.0, last updated: Jun 10, 2019.https://www.uptodate.com/contents/thoracic-nerve-blocktechniques. [Accessed 23 Oct 2019]
Katz D, Khelemsky Y (2013) Paravertebral blockade techniques, clinical applications, and complications. Topics in Pain Management 28(11):1–7. https://doi.org/10.1097/01.TPM.0000431364.10401.ee
Batra RK, Krishnan K, Agarwal A (2011) Paravertebral block. J Anaesthesiol Clin Pharmacol 27(1):5–11 http://www.joacp.org/text.asp?2011/27/1/5/76608
Sabanathan S, Bickford-Smith PJ, Pradhan GN, Hashimi H, Eng JB, Mearns AJ (1988) Continuous intercostal nerve block for pain relief after thoracotomy. Ann Thorac Surg 46:425–426. https://doi.org/10.1016/s0003-4975(10)64657-7
Berrisford RG, Sabanathan SS (1990) Direct access to the paravertebral space at thoracotomy [Letter]. Ann Thorac Surg 49(5):854. https://doi.org/10.1016/0003-4975(90)90058-e
Deebis A, Abdel Sadek H (2001) Efficacy of extrapleural intercostal nerve block with continuous infusion of lidocaine on post-thoracotomy pain and pulmonary mechanics. Zagazig Med Assoc J 7(4):326–334
Maxwell C, Nicoara A (2014) New developments in the treatment of acute pain after thoracic surgery. Curr Opin Anaesthesiol 27(1):6–11. https://doi.org/10.1097/aco.0000000000000029
Elia N, Lysakoski C, Tramer MR (2005) Does multimodal analgesia with acetaminophen, nonsteroidal antiinflammatory drugs, or selective cyclooxygenase-2 inhibitors and patient-controlled analgesia morphine offer advantages over morphine alone? Meta-analyses of randomized trials. Anesthesiology 103:1296–1304. https://doi.org/10.1097/00000542-200512000-00025
Katayama T, Hirai S, Kobayashi R, Hamaishi M, Okada T, Mitsui N (2012) Safety of the paravertebral block in patients ineligible for epidural block undergoing pulmonary resection. Gen Thorac Cardiovasc Surg 60:811–814. https://doi.org/10.1007/s11748-012-0149-5
Watson DS, Panian S, Kendall V, Maher DP, Peters G (1999) Pain control after thoracotomy: bupivacaine versus lidocaine in continuous extrapleural intercostal nerve blockade. Ann Thorac Surg 67(3):825–528. https://doi.org/10.1016/s0003-4975(99)00086-7
Sullivan E, Grannis FW Jr, Ferrell B, Dunst M (1995) Continuous extrapleural intercostal nerve block with continuous infusion of lidocaine after thoracotomy. A descriptive pilot study. Chest 108(6):1718–1723. https://doi.org/10.1378/chest.108.6.1718
Sabanathan S, Mearns AJ, Bickford-Smith PJ, Eng J, Berrisford RG, Bibby SR, Majid MR (1990) Efficacy of continuous extrapleural intercostal nerve block on post-thoracotomy pain and pulmonary mechanics. Br J Surg 77:221–225. https://doi.org/10.1002/bjs.1800770229
Ghisi D, Fanelli A, Jouguelet-Lacoste J, La Colla L, Auroux AS, Chelly JE (2015) Lidocaine versus ropivacaine for postoperative continuous paravertebral nerve blocks in patients undergoing laparoscopic bowel surgery: a randomized, controlled, double-blinded, pilot study. Local Reg Anesth 8:71–77. https://doi.org/10.2147/LRA.S84476
Llevot JMR, Fayad MF, Pacheco MJB, Malo JMC, Gómez SN, Morales JO (2010) Continuous paravertebral block as an analgesic method in thoracotomy. Cir Esp 88(1):30–35. https://doi.org/10.1016/j.ciresp.2010.03.006
Marret E, Bazelly B, Taylor G, Lembert N, Deleuze A, Mazoit JX, Bonnet FJ (2005) Paravertebral block with ropivacaine 0.5% versus systemic analgesia for pain relief after thoracotomy. Ann Thorac Surg 79(6):2109–2113. https://doi.org/10.1016/j.athoracsur.2004.07.030
Sabanathan S, Eng J, Mearns AJ (1990) Alteration in respiratory mechanics following thoracotomy. JRColl Surg Edinb 35:144–150 PMID: 2203902
Borges-Santos E, Genz ICH, Longo AF, Hayahsi D, Goncalves G, Bellinetti LM et al (2012) Pulmonary function, respiratory muscle strength and quality of life in patients submitted to elective thoracotomies. Rev Col Bras Cir 39(1):004–009. https://doi.org/10.1590/s0100-69912012000100003
Roberts GW, Bekker TB, Carlsen HH, Moffatt CH, Slattery PJ, McClure AF (2005) Postoperative nausea and vomiting are strongly influenced by postoperative opioid use in a dose-related manner. Anesth Analg 101:1343–1348. https://doi.org/10.1213/01.ANE.0000180204.64588.EC
Baldini G, Bagry H, Aprikian A, Carli F (2009) Postoperative urinary retention, anesthetic and perioperative considerations. Anesthesiology 110:1139–1157. https://doi.org/10.1097/ALN.0b013e31819f7aea
Asida SM, Ibrahim A, Youssef IA, Mohamad AK, Abdelrazik AN (2012) Post-thoracotomy pain relief: thoracic paravertebral block compared with systemic opioids. Egypt J Anaesth 28:55–60. https://doi.org/10.1016/j.egja.2011.10.004
Acknowledgements
Not applicable.
Funding
No funding was received, self-funded.
Author information
Authors and Affiliations
Contributions
AD designed the study, analysis, and interpretation of data; conducted the statistical analysis; drafted the manuscript; and supervised the study. HE involved in the study design, analyzed and interpreted the data, and drafted the manuscript. OS involved in the study design, analyzed and interpreted the data, and drafted the manuscript. KE involved in the study design, conducted the literature search, performed the data collection, and drafted the manuscript. NE conducted the review of data, involved in the study design, analyzed and interpreted the data, and drafted the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The present prospective study has been approved by Zagazig University Institutional Research Board (IRB#: 6289). The need to obtain informed consent was waived by the local ethical committee.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Deebis, A., Elattar, H., Saber, O. et al. Continuous paravertebral block by intraoperative direct access versus systemic analgesia for postthoracotomy pain relief. Cardiothorac Surg 28, 17 (2020). https://doi.org/10.1186/s43057-020-00027-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43057-020-00027-y