
Abstract
Background
To assess the added value of the dual-volume technique when used with the routine single-volume 3D DSA in the follow-up of endovascularly treated aneurysms.
Results
Seventeen patients (10 females and 7 males) who underwent coiling of their cerebral aneurysms were assessed by 3D DSA using single- and dual-volume techniques. Recanalization of the aneurysm was depicted in 10 cases on the dual-volume technique, only 4 of which were detected on the single-volume 3D DSA technique. Thus, the use of the dual-volume technique upgraded our management plan from follow-up to re-treatment in 6 cases (35%)
Conclusion
The dual-volume technique of 3D DSA is superior to the single-volume technique in visualization of the endovascular devices distinctly, resulting in better evaluation of the aneurysm recanalization and its relation to the parent vessel and occluding device.
Similar content being viewed by others

Background
Treatment of cerebral aneurysms aims to prevent possible aneurysm rupture or re-bleeding. Endovascular embolization is now considered the first line of treatment owing to its minimal invasiveness with reduced mortality and morbidity rates as compared with the surgical intervention [1].
Following endovascular treatment (EVT) of a cerebral aneurysm in about 20% of patients, reopening of the aneurysm or its neck occurs which necessitates retreatment in approximately half of them to ensure long-term protection from bleeding [2]. In addition, the appearance of de novo aneurysms is another concern for all patients with intracranial aneurysm which occurs in about 5 to 10% of patients. Some of these carry enough risk for bleeding despite their small size [3]. Hence, imaging follow-up is crucial for detection and preventive treatment of recurrent or of newly developed aneurysms after EVT [4].
Ideally, the first imaging follow-up should be scheduled 3–6 months after the EVT with further follow-up studies in varying time intervals according to the department’s regimen and the characteristics of the patient and the aneurysm [4].
Although CT angiography (CTA) and MR angiography (MRA) are routinely used to initially diagnose cerebral aneurysms, their use for evaluation of aneurysms following EVT is much more challenging [5]. The high attenuation of the endovascular coil mass causes marked streaky beam hardening artifact on CT and CTA, which typically obscures the aneurysm, the adjacent parent, and branch vessels as well as the surrounding brain parenchyma [6]. In MRA, the coil-induced susceptibility artifacts, slow and complex flow within the residual aneurysm (resulting in spin saturation and de-phasing respectively) coupled with the long acquisition time and the risk of gadolinium-induced nephrogenic systemic fibrosis in patients with renal impairment, are all major limitations in imaging of coiled aneurysms [5].
For the above reasons, digital subtraction angiography (DSA) is considered the gold standard for the assessment of occluded aneurysms by EVT. Three-dimensional (3D) reconstruction of rotational angiography significantly improved the performance of DSA. It requires a flat-panel angiographic system with a motorized rotating C-arm. The acquisition comprised of two rotational scans. The first one collects subtraction masks, while the second scan acquires images during the passage of contrast medium. Software reconstructions then enable extraction of bony structures, deletion of unnecessary vessels, and rotation and zooming of the image, as well as differentiation between vascular contrast filling and vascular devices [7].
In clinical practice, 3D DSA is more sensitive than 2D DSA to small aneurysms and aneurysm remnants [8]. Therefore, 3D DSA was proposed to become a new gold standard of interventional cerebral vascular imaging due to its high spatial resolution with 3D imaging and dynamic information [9]. However, in 3D DSA with single-volume reconstruction, the image quality is degraded by device-related artifacts making recanalization difficult to detect and with difficulty in planning further intervention [7]. The dual-volume reconstruction technique was developed to reduce artifacts and provide more details regarding the aneurysm, parent vessel, and side branches as well as the used endovascular devices [10]. It is derived from the 3D DSA 3 volume data sets which are native (mask), fill, and subtracted-fill. The mask and the subtracted-fill data sets are optimized separately by choosing the best contrast, widowing and color coding, and then fusing them into a single dual-volume image. These images are particularly helpful to differentiate vessels from medical devices and appreciate their relationship with bone structures increasing the accuracy for depicting residual lesions [11].
To the best of our knowledge, few data are available in the literature addressing the advantage of the dual-volume reconstruction technique over the single-volume 3D DSA.
The purpose of this study was to assess the added value of the dual-volume technique when used with the routine single-volume 3D DSA in the follow-up of endovascularly treated aneurysms.
Methods
Patients
From March 2018 through December 2018, 17 consecutive patients on their regular follow-up after EVT of cerebral aneurysm were included in this study. They were 10 females and 7 males (age range 33–67 years; mean = 51.24). The study was approved by our local institutional review board.
DSA technique
A motorized AXIOM Artis® C-arm (Siemens Healthcare, Erlangen, Germany) with 360° rotational run was used to acquire 3D DSA of the cerebral circulation (256 image acquisition). The acquisition comprised of two rotational scans. The first scan was acquired before contrast injection to collect subtraction masks. The second scan acquired images during the passage of iodinated contrast material. Opacification of each artery was done by injection of about 15–20 ml non-ionic contrast (Ultravist®-300) at a rate of 3–4 ml/s. Images were then transferred to the work station (LEONARDO®, Siemens Healthcare, Erlangen, Germany), where the software reconstruction of 3D images was performed to produce the dual-volume images. These enabled the extraction of bony structures and the deletion of unnecessary arteries. Image rotation and zooming were also done with the ability to differentiate between the density of the contrast filling and that of the endovascular device.
Image interpretation
An intervention neuroradiologist (AA) with more than 15 years’ experience assessed the single-volume and the dual-volume reconstructions of the 3D DSA performed for each of the 17 patients. The following factors were individually assessed in each reconstruction:
-
Aneurysm location and occlusion status
-
Position of the residual aneurysm in relation to the coil mass
-
Status of the parent artery and nearby branches
-
Coil migration
Results
Demographic data
A total of 17 aneurysms were imaged. The treated aneurysms were located in the anterior communicating artery (ACOM) in 9 cases, the posterior communicating artery (PCOM) in 3 cases, and the middle cerebral artery (MCA) bifurcation in 3 cases. One case showed basilar tip aneurysm and other one had pericallosal aneurysm. Aneurysms were treated via endovascular approach by either simple coiling or balloon-assisted coiling according to the aneurysmal neck size. Data are summarized in Table 1.
Dual- versus single-volume techniques
Recanalization of the aneurysm was depicted in 10 cases on the dual-volume technique, only 4 of which were seen on the single-volume 3D DSA technique (Figs. 1 and 2). Thus, the use of the dual-volume technique upgraded our management plan from follow-up to re-treatment in 6 cases (35%). Two cases were retreated by simple coiling, other 3 cases were retreated by balloon-assisted coiling, while stent-assisted coiling was done in 5 cases.

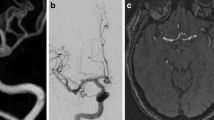
Recanalization of basilar tip aneurysm. a DSA of the basilar artery showing recanalization at the aneurysm neck. b 3D DSA with dual-volume technique clearly differentiates the densities of the occlusion coil and the recanalized part of the aneurysm. c Dual 3D DSA clearly depicts the recanalized part. d DSA final control AP view showing total occlusion of the sac. e Lateral view subtracted DSA image shows total occlusion of the aneurysmal sac. f Post-embolization non-subtracted image shows the added coil cast

PCOM aneurysm. a DSA: the PCOM is seen originating from the neck of the aneurysm. b DSA showing successful coiling of the aneurysmal sac sparing the PCOM artery. c Follow-up DSA 6 months later shows partial recanalization along the neck of the aneurysm. d Dual 3D conventional angiography clearly depicts the recanalization along the aneurysm neck with patent PCOM artery
Discussion
Single-volume reconstruction technique of the 3D DSA depends on multiple image projections allowing the formation of a volumetric representation of the vessel. A complete acquisition comprised of two rotational scans. Subtraction masks are collected in the first scan (mask run). Then, images are acquired during the passage of a contrast material in the second scan (contrast run). Then, both scans are fused and reconstructed as one volume. With the increase in neuro-interventional procedures, it has been important to evaluate the vessels as well as the devices in the treatment of cerebral aneurysms during the follow-up studies [12]. In addition, the accurate position of the re-canalized aneurysm in relation to the parent vessel and endovascularly placed device is very critical for planning proper treatment. In the dual-volume reconstruction of 3D DSA, the obtained data volumes (mask run and contrast run) are first separately reconstructed then fused together. So, we have a separate volume for the vessels and another one for the devices which are modified individually to give the required contrast, windowing, and color coding. This permits more reliable localization of the aneurysm delineating its recurrence or residual in the follow-up studies with consequent improvement in the intervention treatment planning [10].
In the present study, we compared single-volume versus dual-volume reconstruction techniques of 3D DSA in the follow-up evaluation of cerebral aneurysms after their EVT. Objective assessment of both images revealed improved identification of aneurysm recanalization in the dual-volume images. This was in agreement with the study done by Adeeb et al [10], who stated higher overall agreement rate and improved reliability between the raters in the dual-volume technique with better delineation of aneurysm location and its relation to the surrounding vasculature, occlusion status, and the presence of coil migration. Former Chinese studies were conducted addressing the role of the dual-volume technique of 3D DSA [13,14,15]. Zhang et al. [13] studied 20 patients after coil embolization by Guglielmi detachable coil to explore the value of dual-volume reconstruction technique in the follow-up of these patients. They concluded that dual-volume reconstruction technique can display the location of coil bolus, degree of occlusion, and aneurysm size, with evaluation of the embolization effect by multifarious imaging modes, providing a great deal of information for the evaluation of coil embolization of intracranial aneurysm.
Conclusion
The dual-volume reconstruction 3D DSA is superior to the single-volume technique in visualization of the endovascular devices distinctly, resulting in better evaluation of the aneurysm recanalization and its relation to the parent vessel and occluding device. In our practice, we currently use the dual-volume reconstruction for patients during their follow-up evaluation after EVT of cerebral aneurysms.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ACOM:
-
Anterior communicating artery
- CTA:
-
CT angiography
- DSA:
-
Digital subtraction angiography
- EVT:
-
Endovascular treatment
- MCA:
-
Middle cerebral artery
- MRA:
-
MR angiography
- PCOM:
-
Posterior communicating artery
References
Cognard C, Pierot L, Anxionnar R, Ricolfi F (2011) Clarity study group. Results of embolization used as the first treatment choice in a consecutive non selected population of ruptured aneurysms: clinical results of the clarity GDC study. Neurosurgery 69:837–841
Ferns SP, Sprengers ME, van Rooij WJ, Rinkel GJ, van Rijn JC, Bipat S et al (2009) Coiling of intracranial aneurysms: a systematic review on initial occlusion and reopening and retreatment rates. Stroke 40:e523–e529
Kemp WJ III, Fulkerson DH, Payner TD, Leipzig TJ, Horner TG, Palmer EL et al (2013) Risk of hemorrhage from de novo cerebral aneurysms. J Neurosurg 118:58–62
Soize S, Gawlitza M, Raoult H, Pierot L (2016) Imaging follow-up of intracranial aneurysms treated by endovascular means why, when, and how? Stroke 47:1407–1412
Wallace RC, Karis JP, Partovi S, Fiorella D (2007) Noninvasive imaging of treated cerebral aneurysms, part I: MR angiographic follow-up of coiled aneurysms. AJNR Am J Neuroradiol 28:1001–1008
Masaryk AM, Frayne R, Unal O et al (2000) Utility of CT angiography and MR angiography for the follow-up of experimental aneurysms treated with stents or Guglielmi detachable coils. AJNR Am J Neuroradiol 21:1523–1531
Cieściński J, Serafin Z, Strześniewski P et al (2012) DSA volumetric 3D reconstructions of intracranial aneurysms: a pictorial essay. Pol J Radiol Pol Med Soc Radiol 77:47–53
Zhou B, Li MH, Wang W et al (2010) Three-dimensional volume-rendering technique in the angiographic follow-up of intracranial aneurysms embolized with coils. J Neurosurg 112:674–680
Pierot L, Costalat V, Moret J, Szikora I, Klisch J, Herbreteau D et al (2016) Safety and efficacy of aneurysm treatment with WEB: results of the WEBCAST study. J Neurosurg 124:1250–1256
Adeeb N, Griessenauer CJ, Patel AS, Moore J, Ardejani PD, Gupta R, Motiei-Langroudi R, Ogilvy CS, Thomas AJ (2016 Dec) Reliability of dual- vs single-volume reconstruction of three-dimensional digital subtraction angiography for follow-up evaluation of endovascularly treated intracranial aneurysms. Interv Neuroradiol 22(6):687–692
Castillo M, Ramalho J (2013) Vascular imaging of the central nervous system: physical principles, clinical applications, and emerging techniques. Wiley Blackwell, Hoboken, New Jersey
Van Rooij WJ, Sprengers ME, de Gast AN et al (2008) 3D rotational angiography: The new gold standard in the detection of additional intracranial aneurysms. AJNR Am J Neuroradiol 29:976–979
Xiang-hai Z, Jin-hua C, Xiao-feng W, Lin Z, Hong-ye YAN (2014) Application of dual volume reconstruction technique in embolization of intracranial aneurysms. Med J Chin PLA 39:144–148
Zhao L, Wang J, Xu JR et al (2012) Clinical application of double volume reconstruction technique in evaluating interventional embolization for cerebral aneurysms [J]. J Intervent Radiol 21(12):1020–1022
Sun J, Shi WC, Su ZG, et al. Clinical value of dual volume reconstruction in interventional treatment of 16 cases of intracranial aneurysm [J]. Harbin Med J, 2012, 32(5): 337-341
Acknowledgements
Not applicable
Funding
This study had no funding from any resource.
Author information
Authors and Affiliations
Contributions
YI participated in the sequence alignment and drafted the manuscript. AO participated in the sequence alignment and helped to draft the manuscript. AA participated in the design of the study and performed the statistical analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The local ethics committee of Ain Shams University ruled that no formal ethics approval or consent to participate were required in this retrospective study. However, non-formal IRB approval was obtained.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Abdel Samad, A.M., Ibrahim, Y.A. & Othman, A.I.A. Added value of three-dimensional digital subtraction angiography, using dual-volume reconstruction technique, in post-treatment follow-up of cerebral aneurysms. Egypt J Radiol Nucl Med 50, 41 (2019). https://doi.org/10.1186/s43055-019-0037-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-019-0037-4