
Abstract
Background
Screw loosening of a cement-retained, implant-supported fixed partial denture causes the abutment and restoration to be completely separated as one unit from the implant body. In such circumstances, drilling of an access hole through the restoration is made to retrieve the abutment screw connection, and a new restoration is then fabricated.
Method
This clinical case presents a patient whose implant-supported fixed partial denture was completely detached from the implants, and it was retrieved from the abutment’s screw connection using acetic acid (vinegar).
Results
The cement was dissolved and the fixed partial denture was easily separated from the abutment screw connections thus avoiding damage of the restoration.
Conclusion
A new and simple technique was described to retrieve the FPD restoration from the abutments’ screw connections using undiluted acetic acid (vinegar).
Similar content being viewed by others


Background
Implants have revolutionized the dental practice in the last few decades. Implant-supported prostheses are considered a better alternative to the conventional fixed or removable prostheses because they are highly esthetic, functional restorations with long-term predictability (Modi et al. 2014).
Both screw retention and cementation techniques are used to attach the prosthesis to the implants or implant abutments. While some practitioners favor screw-retained prosthesis because they can be retrieved with high predictability and provide a reversible, more stable and secure implant/abutment interface, other practitioners prefer cement-retained prosthesis, because the procedure is simple and offers favorable esthetics, passive placement, and better occlusal loading (Patil 2011; Saponaro et al. 2015).
Previous studies showed that screw retention methods are equally suitable for the partially edentulous patient, although cement-retained restorations are more frequently used. The reason for that was that cement-retained crowns have more in common with regular fixed prosthodontics than do screw-retained restorations and as such have a wider appeal to practitioners of all experience levels (Sherif et al. 2014). Although several studies have proved the reliability and long-term success of these cement-retained restorations, abutment-screw loosening and ultimate screw fracture is a challenging complication in those restorations and may result in masticatory and psychiatric problems to the patient (Chaar et al. 2011).
This clinical case report describes a situation where the cemented fixed partial denture (FPD) restoration was retrieved from the abutment’s screws connection using undiluted acetic acid.
Case presentation
A 51-year-old female came to the Dental Clinic of the National Research Centre, complaining of complete detachment of her implant—supported FPD from their respective implants in the maxillary right first premolar-molar area and holding the abutment with the cemented FPD restoration as one unit in her hand (Fig. 1).

Three-unit porcelain fused to a metal fixed partial denture
First, the patient signed a written informed consent before sharing in this case report, and then, a thorough medical and dental history was taken during which the patient revealed that the implants were placed 4 years ago. The patient also denied having any parafunctional habits such as bruxism or clenching.
Clinical examination
Visual examination revealed two improperly aligned implants in the premolar-molar area (Fig. 2). And clinical examination demonstrated absence of tenderness or inflammations in the surrounding gingiva or the soft tissues, and no implant mobility was detected.

Misaligned implants in the region of the premolar-molar area
Diagnostic assessment
Periapical radiograph was made to assess the bone support, examine the implant body, and detect any fracture.
Intervention
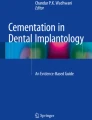
The implant’s internal connection was inspected for possible food debris impaction and was irrigated using a plastic syringe filled by 0.12% chlorohexidine mouthwash (Hekma Pharma, Egypt). A decision was taken to retrieve the abutments’ screw connections from the FPD using 5% acetic acid (vinegar) (sugar cane Wadi Food, Wadi Food Industries Co., Egypt) rather than perforation of restoration to locate the screw access to enable re-cementation of the FPD restoration Fig. 3.

Abutments and screws completely separated from the restoration
To debond the cemented FPD from the abutments, the FPD was suspended in undiluted vinegar for 24 h in such a way that only one abutment was completely immersed one at a time. The pH value of the acetic acid was measured using a pH meter (Hanna Instrument, Romania, Model H12550) and the pH was 2.
After debonding and complete separation of the first abutment from the restoration, the same procedure was repeated for the other abutment.
Residual soft cement was carefully removed from the restoration and the abutment using an excavator.
The retrieved abutments were then placed on the implants, and a periapical radiograph was taken to confirm the correct seating of the abutments to the implant platforms. Tightening of the abutments was done using a wrench torque to 35 N, and the screw access hole was filled with cotton pellets and a cold cured resin material (Acrostone, WHW Plastic, England, packed by Anglo Egyptian Lab).
The FPD restoration was cemented using zinc oxide non-eugenol cement (3M ESPE; Germany) Fig. 4. Excess cement was carefully removed, and a final periapical radiograph was taken to verify the absence of excess luting cement. The occlusion was checked using articulating paper (Horseshoe, USA) to detect any occlusal interferences, and the patient was scheduled for recall appointments.

Cemented FPD in place
Discussion
Implant prostheses are well-documented treatment modalities for completely and partially edentulous patients (Friberg et al. 2008; Turkyilmaz and Jones 2012). However, mechanical complications with the implant components or restorations do arise which may affect the success and durability of the implant restoration (Jung et al. 2008; Hsu et al. 2012). Implant restoration problems such as fractures of the veneer resin or porcelain, loosening and/or fracture of the abutment screw, or even implant fracture have been reported in previous studies (Wittneben et al. 2014). Most of the previously mentioned complications have been attributed to functional overloading, bruxism, and/or improper implant placement (Jugdev et al. 2014). Moreover, their certain circumstances necessitate the retrieval of cemented implant restoration such as unsatisfactory esthetics, poor fitting margins, irresolvable peri-implantitis, or bone loss (Sahu et al. 2014). In the present case report, the patient did not suffer from any parafunctional habits such as bruxism or clenching which could have been the reason for abutment detachment, since screw loosening complication incidences are high among such individuals. On the other hand, clinical examination showed improper implant alignment, which might have caused the separation of the FPD restoration from the implant body after 4 years of implant placement.
In situations where the abutment screw is loosened from the implant body, while the crown remains cemented to the abutment, crown removal without damage to the implant body is a challenging procedure. The most frequently applied technique to retrieve a loosened abutment screw is to perforate the lingual or occlusal portion of the porcelain restoration to locate the screw access hole for screw removal followed by fabrication of a new restoration (Saponaro et al. 2015).
Several alternative techniques have been described for the retrieval of cement-retained, implant-supported restorations with minimal damage. Doerr (2002) demonstrated a method to locate the implant abutment access chamber and abutment screw accurately, so that the implant restoration can be retrieved without damage. Recently, a cement debonding technique using a porcelain furnace was introduced by Saponaro et al. (2015) to separate the implant abutment screw from the retainer.
Many studies reported the adverse effects of the aqueous environment and pH changes on the physical and mechanical properties of both cement types over the time. Deterioration of cement materials in these conditions could be attributed to water absorption and lowered pH. While part of the absorbed water act as plasticizer, causing reduction of the strength of the luting cement, the lowered pH (acidic medium) causes dissolution of the cement (Doerr 2002; Uno et al. 1996).
A previous in vivo study was conducted to evaluate the solubility of three types of luting cements and revealed that polycarboxylate and zinc phosphate cements dissolved more than glass ionomer cement. In addition, a scanning electron microscopy demonstrated pits and widespread cracks on the surfaces of glass ionomer and polycarboxylate cements, whereas zinc phosphate showed a great number of pits (Hersek and Canay 1996).
The previously mentioned facts motivated the authors of the present study to try a simple, cheap, and easy method to break up and dissolve the cement, hence debonding of the restoration from their respective abutments. The immersion of FPD in acetic acid (pH value 2.5) for 24 h was able to dissolve cement in the present case. Consequently, the FPD restoration was easily separated and retrieved safely and this was in accordance with the previously mentioned studies (Uno et al. 1996).
This clinical case also highlights a common complication of improper implant placement, which could result from the lack of practitioner’s experience. Therefore, more practices are needed to avoid such complications.
Conclusions
In this clinical report, a new simple technique was described to retrieve the FPD restoration from the abutments’ screw connections using undiluted acetic acid (vinegar). The acetic acid dissolved the luting cement and the abutment screw connection was separated successfully from the FDP without causing damage to the restoration. Efficient training and skills are essential for the clinicians to avoid similar complications.
References
Chaar MS, Att W, Strub JR (2011) Prosthetic outcome of cement retained implant-supported fixed dental restorations: a systematic review. J Oral Rehabil 38:697–711
Doerr J (2002) Simplified technique for retrieving cemented implant restorations. J Prosthet Dent 88(3):352–353
Friberg B, Raghoebar GM, Grunert I, Hobkirk JA, Tepper G (2008) A 5-year prospective multicenter study on 1-stage smooth-surface Branemark system implants with early loading in edentulous mandibles. Int J Oral Maxillofac Implants 23:481–486
Hersek N, Canay S (1996) In vivo solubility of three types of luting cement. Quint Int 27:211–216
Hsu YT, Fu JH, Al-Hezaimi K, Wang HL (2012) Biomechanical implant treatment complications: a systematic review of clinical studies of implants with at least 1year of functional loading. Int J Oral Maxillofac Implants 27:894–904
Jugdev J, Farahani AB, Lynch E (2014) The effect of air abrasion of metal implant abutments on the tensile bond strength of three luting agents used to cement implant superstructures: an in vitro study. Quintessence Int 29(4):784–790
Jung RE, Pjetursson BE, Glauser R, Zembic A, Zwahlen M, Lang NP (2008) A systematic review of the 5-year survival and complication rates of implant supported single crowns. Clin Oral Implants Res 19:119–130
Modi R, Mittal R, Kohli S, Singh A, Sefa I (2014) Screw versus cement retained prosthesis. A review. Int J Adv Health Sci 1(6):26–32
Patil PG (2011) A technique for repairing a loosening abutment screw for a cement-retained implant prosthesis. J Prosthodont 20(8):652–655
Sahu N, Lakshmi N, Azhagarasan NS, Agnihotri Y, Rajan M, Hariharan R (2014) Comparison of the effect of implant abutment surface modifications on retention of implant supported restoration with a polymer based cement. J Clin Diagn Res 8(1):239–242
Saponaro PC, Heshmati RH, Lee DJ (2015) Using a porcelain furnace to debond cement-retained implant crown from the abutment after screw fracture. A clinical report. J Prosthodont 24:239–242
Sherif S, Susarla H, Kapos T et al (2014) A systematic review on screw versus cement-retained implant-supported fixed prosthodontics. J Prosthodont 23:1–9
Turkyilmaz I, Jones JD (2012) Long term success of 6 implants supporting a mandibular screw-retained fixed dental prosthesis: a clinical report. J Prosthet Dent 107:280–283
Uno S, Finger WJ, Fritz U (1996) Long-term mechanical characteristics of resin-modified glass ionomer restorative materials. Dent Mater 12:64–69
Wittneben JG, Millen C, Bragger U (2014) Clinical performance of screw versus cement retained fixed implant supported reconstructions. A systematic review. Quintessence Int 29:84–98
Funding
All authors equally shared in financing the cost of the research paper.
Availability of data and materials
All data and material are available.
Author information
Authors and Affiliations
Contributions
MIM conceived the idea. MIM, ARM, SAN and ANE were responsible for the clinical part of the case presentation and wrote the paper and revised the final version of the paper. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The patient signed a written informed consent before the beginning of the treatment.
Consent for publication
The patient signed a written informed consent that her age and the type of restoration will be used to publish this case report.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Elboraey, A.N., Moussa, A.R., Nasry, S.A. et al. A simple method to debond a cement-retained implant-supported fixed partial denture from its abutment screw connection: a case report. Bull Natl Res Cent 42, 1 (2018). https://doi.org/10.1186/s42269-018-0002-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42269-018-0002-9