
Abstract
Rhabdomyosarcomas with areas reminiscent of adult type rhabdomyoma are rare and almost exclusive of pretreated tumors. We present a case of 17-year-old patient who sought medical assistance due to a right painless paratesticular mass. At gross examination, the paratesticular mass was a 5 cm tumor (embryonal rhabdomyosarcoma) with a discrete 2.0 cm grayish nodule at the periphery. At microscopy, smaller nodule showed large eosinophilic granular cells suggestive of adult type rhabdomyoma. These cells were strongly and diffusely positive for desmin and multifocally positive for myogenin. Focal neuronal and neural differentiations (NSE and GFAP expression) were also detected. Awareness of benign appearing intratumoral rhabdomyoma in rhabdomyosarcomas of paratestis/retroperitonium is of relevance. Such tumor heterogeneity may be a diagnostic pitfall especially in the scenario of needle biopsies and frozen section consultation.
Similar content being viewed by others


Background
Rhabdomyosarcomas with areas reminiscent of adult type rhabdomyoma are rare and almost exclusive of pretreated tumors. Ectomesenchymomas are rare tumors that consist of rhabdomyosarcomas (mostly embryonal) with neural or neuronal components. The later are more common in young children and paratestis is one of the most common affected regions.
Case presentation
We present a case of 17-year-old patient who sought medical assistance due to a right painless paratesticular mass. The patient reported a progressive growth for 10 months, without association with trauma. Physical exam showed topical testicles with well-defined solid tumor, postero-inferior to the right testicle, without palpable lymph nodes.
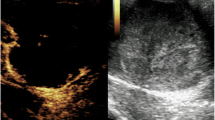
At ultrasound, there was a tumor in topography of the right epididymis tail with spheroid, heterogeneous, low echogenicity and an estimated volume of 23 cm3. Alpha-fetoprotein and human chorionic gonadotropin were not elevated. At computer tomography, a heterogeneous lesion inseparable from the epididymis was detected (Fig. 1a, b) without lymph node enlargements.

Imaging and gross findings. a Computer tomography - Axial view - long arrow indicates the paratesticular tumor and short arrow indicates right testis; b Lateral view - long arrow indicates the paratesticular tumor and short arrow indicates right testis; c Gross findings - right testis (below), the main mass and a small 2 cm nodule (upward) which prove to show adult type rhabdomyoma morphology
A right orchiectomy was performed. At gross examination, the paratesticular mass was a 5 cm vaguely lobulated and fasciculated white tumor with focal areas of gross hemorrhage (Fig. 1c). At microscopy, myxoid and cellular areas of primitive and fusiform cells predominated. Strap cells and large rhabdomyoblasts were easily recognizable. All these cells stained for myogenin and desmin. This 5 cm tumor was interpreted as an embryonal rhabdomyosarcoma (Fig. 2).

Main mass - embryonal rhabdomyosarcoma. a Cellular and myxoid areas (HE, 40x), b Rhabdomyoblasts (HE, 200x) and c Strap cells (HE, 200x). d Myogenin in primitive tumor cells (200x) and e Desmin in strap cells (200x)
A discrete 2.0 cm grayish nodule was observed in the periphery of the paratesticular mass. At microscopy, this nodule showed large eosinophilic granular cells closely packed together. Immunohistochemistry was performed for differential diagnosis between rhabdomyocites and ganglion/ganglioneuroma cells. These cells were strongly and diffusely positive for desmin and multifocally positive for myogenin. The large eosinophilic cells were negative for S100, chromogranin and synaptophysin. In focal areas, these cells stained for neuron specific enolase (NSE). Fusiform cells adjacent to large cells were negative for S100 but stained focally for glial fibrillary acidic protein (GFAP) (Fig. 3).

Nodule with large eosinophilic cells. a HE (40x), HE (200x) and b HE (400x). Desmin (200x), Neuron specific enolase (400x) and Glial fibrillary acidic protein (400x)
Discussion
Based on morphology and immunophenotype (multifocal myogenin staining and strong and diffuse expression of desmin), this discrete nodule was interpreted as an adult type rhabdomyoma area associated with the larger rhabdomyosarcoma. Focal evidence of neuronal and neural differentiation was not evidence of ganglioneuroma-like areas. Focal positivity for NSE have been described in rhabdomyoblasts of rhabdomyosarcomas (Cheng and Bostwick 2014). Based only in immunohistochemical evidence of NSE and GFAP expression, these focal areas of neuronal and neural differentiation could qualify the whole mass as an ectomesenchymoma.
Ectomesenchymoma is defined as a rhabdomyosarcoma with a neural or neuronal component (Fletcher et al. 2013). It is rare, usually affect children aged < 5 years and paratesticular region is one of the most common sites of involvement. The rhabdomyosarcoma component is usually of embryonal or spindle cell type. Neuronal or neural differentiation includes ganglion cells, ganglioneuroma, neuroblastoma or malignant peripheral nerve sheath tumor (Fletcher et al. 2013). It is not clear from WHO definition of ectomesenchymoma, however, if only immunohistochemical evidence of neuronal/neural differentiation in otherwise typical rhabdomyoma morphology would qualify these areas as neuronal/neural component.
Treatment ectomesenchymoma is based on protocols for rhabdomyosarcoma and the treatment responses are similar to those of pure rhabdomyosarcoma. Factors for good prognosis include size < 10 cm, low stage, superficial location and absence of alveolar rhabdomyosarcoma (Fletcher et al. 2013). Follow up of paratesticular ectomesenchymoma are available for seven reported cases with lung metastasis in an adult documented in one case (Kao et al. 2015). These would be the third case reported in postpuberal patients.
Embryonal rhabdomyosarcomas have better prognosis when affecting children aged 1–9 years and when located in paratestis. Treatment is based on a multidisciplinary approach: surgery with clear margins and chemotherapy is indicated for all patients. Although a combination with radiation therapy is recommended for most patients with rhabdomyosarcoma, patients with embryonal type and negative surgical margins can avoid it (Meyer and Spunt 2004). Response to treatment is predicted by risk stratification that includes data on primary site, residual disease after resection, locoregional spread and distant metastasis. Current survival rates for rhabdomyosarcomas of low, intermediate and high risk groups are 70–90%, 50–70% and 20–30%, respectively (American Cancer Society 2018).
Rare cases of embryonal rhabdomyosarcoma may show well differentiated round, polygonal and spindle shaped rhabdomyoblasts as the predominant cell type (Goldblum et al. 2014). This phenomenon is well described in cases after prolonged therapy and may result from selective survival of differentiated cells (Coffin et al. 2005). In the present case, no treatment was performed before surgery.
Conclusion
Awareness of benign appearing intratumoral rhabdomyoma in rhabdomyosarcomas of paratestis/retroperitonium is of relevance. Such tumor heterogeneity may be a diagnostic pitfall especially in the scenario of needle biopsies and frozen section consultation.
Availability of data and materials
Not applicable.
References
American Cancer Society (2018) Cancer Facts & Figures 2018. American Cancer Society, Atlanta
Cheng L, Bostwick DG (2014) Urological Surgical Pathology, 3rd edn. Elsevier Saunders, Philadelphia, p 310
Coffin CM, Lowichik A, Zhou H (2005) Treatment effects in pediatric soft tissue and bone tumors: practical considerations for the pathologist. Am J Clin Pathol 123(1):75–90. https://www.ncbi.nlm.nih.gov/pubmed/15762282.
Fletcher CDM, Bridge JA, Hogendoorn PCW, Mertens F (2013) WHO classification of tumours of soft tissue and bone, 4th edn. International Agency of Research on Cancer, Lyon, p 191
Goldblum JR, Weiss S, Folpe A (2014) Enzinger and Weiss's soft tissue tumors, 6th edn. Elsevier Saunders, Philadelphia, p 609
Kao WT, Chiang YT, Tzou KY (2015) An adult paratesticular malignant ectomesenchymoma with post-operative flare-up of lung metastasis. Urol Case Rep 3(5):164–166
Meyer WH, Spunt SL (2004) Soft tissue sarcomas of childhood. Cancer Treat Rev 30:269–280
Acknowledgements
Not applicable.
Funding
This study had no funding resources.
Author information
Authors and Affiliations
Contributions
DAA conceived the idea. DAA was the major contributor to the writing of the manuscript. MLOL and FMSP participated in the surgical treatment surgery. DAA, SCS and PA diagnosed the case. MLOL and FMSP were major contributors for critically revising the manuscript for important intellectual content. PA and SCS has given expert opinion and final approval of the version to be published. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for participation in the study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Santana, S.C., Prado, F.M.S., de Oliveira Leal, M.L. et al. Rhabdomyosarcoma with an intratumoral adult type rhabdomyoma nodule with focal neuronal differentiation - diagnosis, prognosis and treatment of a rare disease. Surg Exp Pathol 3, 10 (2020). https://doi.org/10.1186/s42047-020-00063-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42047-020-00063-2