
Abstract
Background
Benzodiazepines (BDZ) are a class of psychoactive drugs that have been widely used for the treatment of many medical conditions. In this paper, a case of an atypical pattern of diazepam dependence in a patient with epilepsy is presented. The article may be an interesting proposition for rational management in the treatment of benzodiazepine dependence in a patient with non-withdrawal and withdrawal seizures. Detoxification is used then to optimize neurological treatment.
Case presentation
A 52-year-old Caucasian male, diagnosed with epilepsy with partial complex, and rarely tonic-clonic seizures and benzodiazepine (diazepam) misuse, was admitted to a detoxification unit specialized to treat substance dependence. This patient presented an atypical schedule of substance misuse with a weekly dose of 40 to 45 mg of diazepam, taken once a week, every Saturday. The patient reported having a group of symptoms that usually preceded generalized seizures that were described as the “aura” manifesting as confusion, derealisation, anxiety, and difficulties in speaking. First Saturday after admission to the hospital, the first aura experience was reported, while diazepam level in serum was higher than usual, which was supporting also strong psychological background for withdrawal. On weekend days, 3 weeks after admission, when the patient was receiving 3 mg of diazepam daily, he developed a severe “aura.” The EEG showed no seizure activity. Two weeks later (again Friday to Saturday), the patient reported the occurrence of aura, the EEG recording showed paroxysmal discharges, generalized multiple spikes associated with slow waves, lasting about 30 s, accompanied by eyelid myoclonia and disturbed consciousness. A week later another aura developed that resolved spontaneously without a seizure. Twelve days later, diazepam was completely removed; the elimination of serum benzodiazepines took place. The patient did not report aura until the end of the stay and he was dismissed 5 weeks later.
Conclusions
The differential diagnosis of an aura can be challenging. Carefully proceed serum monitored elimination of benzodiazepines in epileptic patients may serve in safety benefits and helps to achieve detoxification goals. Hence, it is important to prevent, recognize, and treat benzodiazepine dependence in every patient and may improve epilepsy treatment outcome.
Similar content being viewed by others


Highlights
-
1
Rational management in the treatment of benzodiazepine dependence in epilepsy.
-
2
Differential diagnosis of aura can be challenging during benzodiazepine withdrawal.
-
3
Recognition and treatment of benzodiazepine dependence in epileptic patient may improve treatment outcome of epilepsy.
Background
Benzodiazepines (BDZ) are a class of psychoactive drugs that have been widely used for the treatment of many medical conditions. The most common indications for the use of benzodiazepines include, among others, anxiety disorders, insomnia, alcohol withdrawal, and seizures [1, 2]. They play an important role in the emergency management of acute seizures and status epilepticus. However, the clinical use of benzodiazepines for the prophylactic treatment of epilepsy is limited due to its side effects and the high risk of development of tolerance and dependence [3].
The use of benzodiazepines is associated with insomnia and impulsiveness secondary to drug reduction or discontinuation, dependence, and acute withdrawal syndrome, or even suicide risk. Due to possible medical issues with BDZ use, it is recommended to discontinue them after the indications for use have ceased [4]. The typical course of BDZ dependence consists of everyday use with a possible escalation of the dose to relieve withdrawal symptoms. In the case of dependence, BDZ detoxification is a primary treatment [2].
In this paper, a case of an atypical pattern of diazepam dependence in a patient with epilepsy is presented. The article may be an interesting proposition for rational management in the treatment of benzodiazepine dependence in a patient with non-withdrawal and withdrawal seizures. Detoxification is used then to optimize neurological treatment. This paper adheres to CARE guidelines (http://www.care-statement.org/downloads) for reporting of case reports.
Case presentation
A 52-year-old Caucasian male, diagnosed with epilepsy of unknown etiology with complex partial, and rarely tonic-clonic seizures (2001) and benzodiazepine (diazepam, a long active benzodiazepine) misuse (2003) was admitted to a detoxification unit specialized to treat substance dependence. The patient met the diagnostic criteria of diazepam dependence according to ICD-10. All previous attempts (in outpatient clinic environment), to stop taking BDZ were unsuccessful, mainly due to withdrawal symptoms and worsening the course of treatment of epilepsy (more frequent seizures).
The most common model for taking BDZ is to take them every day, or several times a day. This patient presented an atypical schedule of substance misuse with a weekly dose of 40 to 45 mg of diazepam, taken once a week, every Saturday. The studied subject had a history of epilepsy with partial complex, and rarely tonic-clonic seizures (TCS) for which he had been receiving gabapentin 2400 mg daily, and carbamazepine 1200 mg daily. The last TCS had occurred 10 years before the current admission. Since 2 years before admission, the course of treatment got worsened. Simple, complex partial seizures and multiple auras occurred. For this reason, another antiepileptic was added—levetiracetam 1000 mg daily. The subject was referred to the hospital in order to optimize neurological treatment by BDZ detoxification.
The patient reported having a group of symptoms that usually preceded generalized seizures that was described as “aura” manifesting as confusion, derealisation, anxiety, and difficulties in speaking. The symptoms usually appeared every 6-7 days and as the patient reported taking diazepam “as a prevention of generalized seizure.” The history of dependence had started about 2 years after the diagnosis of epilepsy.
The patient’s history and data were analyzed; the diagnosis of epilepsy was revised by the consultant specialist of neurology. The detoxification process was designed, proposed, and accepted by the patient. Admission to the hospital took place 4 days after the last diazepam use—40 mg. Benzodiazepine serum level was measured and planned for the next days. On admission, diazepam 34 mg daily was administered and tapered gradually. The dosage was decreased by 1-2 mg per day until 5 mg was reached, followed by a decrease of 1 mg per week. The doses have been spaced evenly throughout the day with the frequency of every 6 h. No PRN (as needed) doses were accepted.
During the gradual reduction of diazepam, the patient reported aura symptoms every, including the first, Saturday that resolved spontaneously or after administration of prescribed medications. After the admission to the hospital, the first aura (Saturday) experience was reported, while the diazepam level in serum was higher than usual, which was supporting also strong psychological background for withdrawal and focused our attention on its importance. On weekend days, 3 weeks after admission, when the patient was receiving 3 mg of diazepam daily, he developed a severe “aura.” The EEG showed no seizure activity. Magnetic resonance imaging showed a new cortical-subcortical lesion (in comparison to previous MRI 11 years ago) surrounded by a limb of glycolysis in the right frontal lobe, and a similar lesion described earlier in the right temporal lobe. A specialist neurologist consultation and opinion were requested. After the event, according to neurological assessment, the levetiracetam dose was increased up to 2000 mg per day. Serum levels of antiepileptic drugs reached 8.0 μg/ml for carbamazepine and 6.11 μg/ml for levetiracetam.
Two weeks later (again Friday to Saturday), the patient reported the occurrence of aura, the EEG recording showed paroxysmal discharges, generalized multiple spikes associated with slow waves, lasting about 30 s, accompanied by eyelid myoclonia and disturbed consciousness. There were described changes in frontotemporal regions—slow background activity with sharp-and-slow waves. Routine check-up EEG 3 days after was normal.
A week later, another aura developed that resolved spontaneously without a seizure. Twelve days later, diazepam was completely removed; the elimination of serum benzodiazepines took place. The patient did not report aura until the end of the stay and he was dismissed 5 weeks later. At his evaluation, he had no complaints.
Conclusions
This case presentation may have some limitations. It may not be clear whether the studied patient is a true epileptic or had one of the non-epileptic episodic events as it is more passing with either functional seizure or drug withdrawal induced. However, taken history and three different opinions of specialists of neurology have confirmed that the studied subject was epileptic, and did not use benzodiazepines previous to the first seizure episode.
The differential diagnosis of an aura can be challenging. The collection of symptoms described by the patient occurs across a wide range of disorders, including cardiac, psychiatric, and neurological conditions. It can be particularly difficult to differentiate partial seizures without generalization of temporal lobe origin from panic disorder, as all of the above symptoms can be found in both conditions. There is also a possibility of comorbidity of these medical states. The seizure may also occur as a result of withdrawal from benzodiazepines. However, the course of the disease and additional tests confirmed the occurrence of epileptic seizures during the hospital stay.
After the first introduction, benzodiazepines were adopted for treating all forms of epilepsy. However, cognitive impairment and dose-related tolerance become problems with continued use and none are now considered first-line choices for long-term epilepsy therapy. Misuse of BDZ besides socio-economic costs leads to many long-term adverse effects that include dependency, cognitive decline, falls, and risk of cancer [5]. Discontinuation with the aim of abstinence results in the enhancement of quality of life. Carefully proceed serum monitored elimination of benzodiazepines in epileptic patients may serve in safety benefits and helps to achieve detoxification goals. Hence, it is important to prevent, recognize, and treat benzodiazepine dependence in every patient and may improve epilepsy treatment outcome.
Availability of data and materials
Authors declare possibility to provide data if required.
Abbreviations
- BDZ:
-
Benzodiazepines
- EEG:
-
Electroencephalography
- MRI:
-
Magnetic resonance imaging
- PRN:
-
Drug administered “when necessary”
- TCS:
-
Tonic-clonic seizures
References
Votaw VR, Geyer R, Rieselbach MM, McHugh RK. The epidemiology of benzodiazepine misuse: a systematic review. Drug Alcohol Depend. 2019;200:95–114. https://doi.org/10.1016/j.drugalcdep.2019.02.033.
Silczuk A, Heitzman J. New regulations regarding e-prescriptions may increase the risk of acute withdrawal syndromes in patients dependent on benzodiazepines or non-benzodiazepine hypnotics. Psych Pol. 2020;54(2):351–8. https://doi.org/10.12740/PP/115555.
Shorvon SD. Drug treatment of epilepsy in the century of the ILAE: the second 50 years, 1959-2009. Epilepsia. 2009;50(Suppl 3):93–130. https://doi.org/10.1111/j.1528-1167.2009.02042.x.
Fluyau D, Revadigar N, Manobianco BE. Challenges of the pharmacological management of benzodiazepine withdrawal, dependence, and discontinuation. Ther Adv Psychopharmacol. 2018;8(5):147–68. https://doi.org/10.1177/2045125317753340.
Penninkilampi R, Eslick GD. A systematic review and meta-analysis of the risk of dementia associated with benzodiazepine use, after controlling for protopathic bias. CNS Drugs. 2018;32(6):485–97. https://doi.org/10.1007/s40263-018-0535-3.
Acknowledgements
N/A
Funding
Authors declare that the paper did not require funding.
Author information
Authors and Affiliations
Contributions
AS prepared the research concept and the design of the publication. NP wrote the article and made the graphic design. AS critically revised it. Both authors contributed equally to the final version of the publication, have read, and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This paper is a case study report and therefore Bioethics Committee consent was not required. Paper was prepared in accordance to the CARE guidelines.
Consent for publication
A written consent for publication is given by the patient.
Competing interests
Authors declare no possible competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
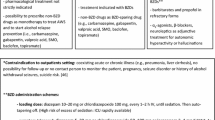
Diagram 1: Diazepam substitution vs. elimination and seizure episodes.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Piskorska, N., Silczuk, A. Atypical benzodiazepine misuse and withdrawal in patient with epilepsy: a case report. Egypt J Neurol Psychiatry Neurosurg 56, 113 (2020). https://doi.org/10.1186/s41983-020-00248-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41983-020-00248-2