
Abstract
Introduction
Isolated unilateral hypoglossal nerve palsy is an infrequent condition that usually appears in connection to an underlying disease. Rarely, the cause cannot be determined, and there is no symptom remission.
Case description
We report two cases of male patients who developed persistent idiopathic isolated unilateral hypoglossal nerve palsy. The younger patient complained of involuntary movements of the tongue, while the older patient developed dysarthria. In both cases, the symptoms lasted for several weeks before the initial clinical examination, and after comprehensive clinical, laboratory, and imaging investigations, no underlying cause was detected. Both patients did not show remission of symptoms on the follow-up examinations done after several months.
Discussion
Idiopathic isolated unilateral hypoglossal nerve palsy is an underreported condition, most likely due to the expected reversible nature of the disease. In the case of persistence of symptoms, extensive medical assessment is needed before postulating a diagnosis of persistent idiopathic isolated unilateral hypoglossal nerve palsy. There are no treatment guidelines for this condition, but oral steroids were reported as a treatment option. Therefore, physicians should use a systematic approach to exclude serious underlying pathology or identify a treatable condition.
Similar content being viewed by others


Background
Isolated unilateral hypoglossal nerve palsy (IUHNP) is a rare condition that is usually a manifestation of an underlying disease and therefore must be investigated extensively. Idiopathic IUNHP is even less frequent and has been reported mostly in single case reports. Signs of hypoglossal nerve palsy (HNP) encompass deviation of the tongue to the affected side, absence of power and movement on the same side, fasciculations, and at a later stage atrophy. Most patients complain of dysarthria, while a few patients complain of eating difficulties [1]. In some cases, despite extensive investigations, the cause could not be identified, and therefore, a diagnosis of idiopathic IUHNP was postulated [1,2,3,4,5,6]. Most of these cases are self-limiting, and there are only a few reported cases of persistent idiopathic IUNHP [4, 5, 7].
We report two cases of younger male patients who developed persistent idiopathic IUHNP.
Case presentation
The first patient was a 17-year-old male who was admitted after noticing involuntary movements of the tongue 1 month before the first clinical examination. An initial visit to the otolaryngologist failed to provide any diagnosis, and it was purely a cosmetic problem for the patient. He had no dysphagia or articulation problems. A clinical examination showed fasciculations and atrophy of the right side of the tongue as well as right-sided deviation (Fig. 1a). The face was otherwise symmetrical, without signs of cervical lymphadenopathy. A thorough neurologic examination revealed no other findings except decreased sensation of the right side of the tongue. His swallowing function was preserved. The patients’ medical history (MH) was unremarkable as well as there were no known neurodegenerative disorders (ND) in the patients’ family MH. Blood tests were within normal ranges and included full blood count; serum electrolytes; glucose; function tests of the liver, kidney, and thyroid; creatine kinase; vitamin B12; folate; iron; ferritin; transferrin; serum electrophoresis; C-reactive protein; and autoantibodies. Tests for treponema, Epstein-Barr virus, human immunodeficiency virus, herpes simplex virus, and cytomegalovirus were negative. Cerebrospinal fluid (CSF) tests showed normal protein levels, no abnormal cells, and no oligoclonal bands. Head and neck magnetic resonance imaging (MRI) scan (Aera 1.5 Tesla, Siemens, Germany) with targeted imaging of the hypoglossal nerve as well as skull base computed tomography (CT) scan (Somatom Force, Siemens, Germany) was normal (Fig. 1b–d) [8]. Head and neck MRI showed fatty infiltration and atrophy of the right half of the tongue due to chronic muscle denervation (Fig. 1e). The patient did not receive oral steroid treatment. Seven months after symptoms onset, there were no signs of remission and the patient did not complain of any new symptoms.

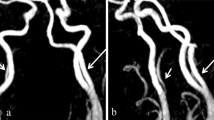
a Right-sided atrophy along with tongue deviation 7 months after onset of symptoms. b Cisternal segment of the right hypoglossal nerve (HN) on 3D constructive interference in steady state (CISS) magnetic resonance imaging (MRI) showing normal appearance (white arrow). c Normal morphology of the skull base segment of the right HN inside of the right hypoglossal canal (HC) on 3D T1-weighted contrast enhanced (CE) MRI. The HN is of hypointense signal (white arrow), while the surrounding venous plexus shows prominent CE. d Axial computed tomography scan of the skull base demonstrating a normally appearing HC (white arrow). e Head and neck T1-weighted MRI demonstrates fatty infiltration and atrophy of the right half of the tongue due to chronic muscle denervation (white arrow)
The second patient, a 44-year-old male, was referred to our institution after developing dysarthria during a period of a month and a half. The clinical examination showed visible fasciculations and atrophy of the right side of the tongue, while his swallowing was normal. His previous clinical history included right-sided periauricular headache during the last 6 months. The patient was not aware of any ND in his family MD. Blood and CSF analyses as well as tests to rule out infectious diseases performed as for the first patient were within normal ranges or negative. A head and neck MRI scan and skull base CT scan, obtained with the same imaging protocol and on the same equipment as for the first patient, did not reveal any abnormalities. Electromyography (Neuropack X1 MEB-2300, Nihon Kohden Corporation, Japan) confirmed chronic partial denervation of the right side of the tongue. The patient started with speech therapy (ST), and no pharmacological treatment was given. No remission of dysarthria was detected on the follow-up examination after 6 months, despite of ST, as well as no new symptoms were noted by the patient.
In both cases, an extensive array of investigations detected no underlying disease, and therefore, a diagnosis of persistent idiopathic IUHNP was suggested.
Discussion
HNP in general appears together with other neurological abnormalities in a large variety of diseases. A brainstem lesion frequently involves other nuclei or tracts, and a skull base lesion often affects other cranial nerves at the same time. Tumors are the predominant underlying condition of HNP [9]. Vertebral artery dissection, nasopharyngeal cancer, Chiari malformation, and dural arteriovenous fistula are other known causes [1]. These quite different etiologies emphasize the necessity of extensive medical assessment when confronted with a case of HNP, especially when postulating a diagnosis of idiopathic IUHNP.
Idiopathic IUHNP is believed to be an underreported condition which is more frequent than previously thought [6, 9]. Ahmed and colleagues found 13 single case reports [3]. Most cases are reversible without any treatment and resolve within 2 to 4 weeks, though longer recovery periods between 2 to 5 months have been reported [1, 2, 6]. The persistence of symptoms in both our cases is unusual in idiopathic IUHNP compared to most other reported cases. Ho and colleagues described a case of idiopathic IUHNP that persisted over a period of at least 5 years and suggested a pathway of investigations to make the diagnosis of idiopathic IUHNP by way of exclusion [5]. Two other cases of idiopathic IUHNP reported persistency of symptoms for a period of 36 months and 24 months respectively [4, 7]. Rarely, idiopathic IUHNP can be an early manifestation of an underlying demyelinating disease, and therefore, it has been recommended to do a repeat brain MRI scan every 3 to 5 years [3, 5].
The age of patients with isolated IUHNP varies a lot. The youngest reported patient was11 years old, while most other patients were between 25 and 81 years old [2]. No clear specific age of onset is evident as well as there is no gender prevalence. To the best of our knowledge, our younger patient is the second reported having persistent idiopathic IUNHP at the age of 17 years.
It has been suggested by Lee and colleagues that idiopathic IUHNP is a clinical entity similar to Bell’s palsy (BP) [6]. The use of oral steroids (OS) within 72 h of symptom onset in BP increases the likelihood of recovery of the facial nerve [10]. In some case reports, OS have been used to treat idiopathic IUHNP, but a literature search revealed no clinical guidelines on the use of OS as a treatment option for this condition [2]. As our patients were referred to us 1 month and 1 month and a half respectively after symptoms onset, with already visible tongue atrophy and fasciculation, we did not start OS treatment. Idiopathic IUHNP might involve speech and language impairment, and ST has been used as a rehabilitation method [5]. Our first patient had no dysarthria, and no rehabilitation was required, while ST was implemented for the second patient, but without dysarthria improvement.
Thus, following the same pathway of investigation as suggested by Ho and colleagues, we presented two cases with persistent idiopathic IUHNP [5]. IUHNP is a rare diagnosis with a challenging clinical presentation, and we recommend that physicians use a systematic approach to exclude severe underlying pathology or identify a treatable condition.
Availability of data and materials
The datasets supporting the conclusions of this article are included within the article.
Abbreviations
- IUHNP:
-
Isolated unilateral hypoglossal nerve palsy
- HNP:
-
Hypoglossal nerve palsy
- MH:
-
Medical history
- ND:
-
Neurodegenerative disorder
- CSF:
-
Cerebrospinal fluid
- MRI:
-
Magnetic resonance imaging
- ST:
-
Speech therapy
- BP:
-
Bell’s palsy
- OS:
-
Oral steroids
References
Combarros O, Alvarez de Arcaya A, Berciano J. Isolated unilateral hypoglossal nerve palsy: nine cases. J Neurol. 1998;245:98–100.
Yoon JH, Cho KL, Lee HJ, Choi SH, Lee KY, Kim SK, et al. A case of idiopathic isolated hypoglossal nerve palsy in a Korean child. Korean J Pediatr. 2011;54:515–7.
Ahmed SV, Akram MS. Isolated unilateral idiopathic transient hypoglossal nerve palsy. BMJ Case Rep. 2014:bcr2014203930.
Sayan A, Abeysinghe AH, Brennan PA, Ilankovan V. Persistent idiopathic unilateral hypoglossal nerve palsy: a case report. Br J Oral Maxillofac Surg. 2014;52:572–4.
Ho MW, Fardy MJ, Crean SJ. Persistent idiopathic unilateral isolated hypoglossal nerve palsy: a case report. Br Dent J. 2004;196:205–7.
Lee SS, Wang SJ, Fuh JL, Liu HC. Transient unilateral hypoglossal nerve palsy: a case report. Clin Neurol Neurosurg. 1994;96:148–51.
Ilardi A, Moglia C, Cammarosano S, Canosa A, Bertuzzo D, Manera U, et al. Persistent idiopathic hypoglossal nerve palsy: a motor neuron disease-mimic syndrome? Amyotroph Lateral Scler Frontotemporal Degener. 2015;16:274–6.
Alves P. Imaging the hypoglossal nerve. Eur J Radiol. 2010;74:368–77.
Keane JR. Twelfth-nerve palsy. Analysis of 100 cases. Arch Neurol. 1996;53:561–6.
Baugh RF, Basura GJ, Ishii LE, Schwartz SR, Drumheller CM, Burkholder R, et al. Clinical practice guideline: Bell’s palsy. Otolaryngol Head Neck Surg. 2013;149(Suppl 3):1–27.
Acknowledgements
Not applicable.
Funding
No source of funding.
Author information
Authors and Affiliations
Contributions
CO, MBG, and JF diagnosed the patients and collected clinical data. CO and RA carried out the literature search, review, and manuscript preparation. All authors read and approved the final manuscript.
Authors’ information
CO—MD, neurology resident
MBG—MD, neurology resident
JF—MD, consultant neurologist
RA—MD, PhD, consultant radiologist
Corresponding author
Ethics declarations
Ethics approval and consent to participate
We confirm that ethical clearance was not required for publication of this case report. Written informed consent was obtained from the patients.
Consent for publication
The patients were informed, and written consent was taken from the patients for this publication.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Olesen, C., Groen, M.B., Forsberg, J. et al. Persistent idiopathic unilateral isolated hypoglossal nerve palsy – a report of two cases. Egypt J Neurol Psychiatry Neurosurg 56, 84 (2020). https://doi.org/10.1186/s41983-020-00216-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41983-020-00216-w