
Abstract
Background
Renal anemia is the important complication in patients undergoing peritoneal dialysis (PD), and heart failure (HF) is the important complication in patients on dialysis. Decreasing endogenous erythropoietin (EPO) in patients with chronic kidney disease is a major cause of renal anemia. On the other hand, high levels of EPO have been associated with the prognosis of patients with chronic HF. The association between plasma EPO and HF in patients on PD remains unclear. This study was designed to test our hypothesis that the plasma EPO level in patients on PD was associated with the markers of HF.
Methods
We investigated 39 patients undergoing PD at our hospital. We measured plasma EPO before erythropoiesis-stimulating agent (ESA) administration at the regular outpatient visits and then at 2 weeks after the final dose of ESA was administered and investigated the clinical factors. We estimated the correlations between the plasma EPO and the other parameters, and constructed univariate and multivariate logistic regression models for the risk for HF to estimate the effectiveness of plasma EPO and other factors on HF treatment in patients undergoing PD.
Results
The plasma EPO concentration was positively correlated with the ESA dose and negatively correlated with serum ferrum, transferrin saturation, and body mass index and showed no correlation with other factors, such as the New York Heart Association (NYHA) classification and ferritin level. In univariate analysis, the factors significantly associated with HF risk were N-terminal pro-brain natriuretic peptide (NT-pro BNP), cardiothoracic ratio (CTR), serum creatinine (Cr), serum beta 2 microglobulin, dialysate dose, left ventricular mass index, left ventricular end-systolic diameter, left ventricular end-diastolic diameter, and weekly Kt/V. We performed a multivariate analysis with NT-pro BNP, Cr, and CTR, and all three factors were significant in the analysis.
Conclusion
The plasma EPO level in patients undergoing PD was positively correlated with the monthly ESA dose and was not significant as a marker of HF, as judged with the NYHA classification. Therefore, the plasma EPO level may not be a useful marker for HF in patients undergoing PD.
Similar content being viewed by others

Background
Renal anemia is one of the most common complications of chronic kidney disease (CKD) [1] and is one of the most important complications in patients undergoing peritoneal dialysis (PD). Moreover, heart failure (HF) is an important complication, which necessitates hospitalization and death in patients undergoing dialysis [2, 3]. Previous studies reported that 25–40% of HF patients have anemia that is associated with the risk for mortality and hospitalization in HF patients [4,5,6,7]. Reduction in the endogenous erythropoietin (EPO) is a major cause of renal anemia in patients with CKD [1, 8]. In contrast, high EPO levels are associated with patient prognosis in chronic HF, independent of the hemoglobin (Hb) levels [5, 9] and worse prognosis in patients with decompensated HF, including patients with impaired renal function, excluding those with estimated glomerular filtration rate (eGFR) < 10 mL/min/1.73 m2, independent of anemia and renal failure [10].
PD patients often have residual renal function and may exhibit similarities to pre-dialysis patients with CKD; however, patients on PD are mostly on erythropoiesis-stimulating agents (ESA), such as darbepoetin alfa. However, the association between the plasma EPO and HF in patients on PD remains unclear. This cross-sectional observational study was designed to test our hypothesis that the plasma EPO level in patients on PD was associated with the markers of HF because the plasma EPO level in the pre-dialysis patients with CKD was associated with HF.
Methods
Study population and study design
In this single-center retrospective observational cross-sectional study, we enrolled patients who provided informed consent for study participation, with the option of opting out. Those patients who refused to participate were not included in the trial. The present study protocol was approved by the Ethical Committee of the Nippon Medical School Hospital (B-2020-121) and registered at the University Hospital Medical Information Network as UMIN No. 000041146. The study protocol was in keeping with the principles in the Declaration of Helsinki.
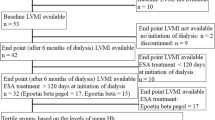
A total of 42 patients who were undergoing PD and who were regularly followed-up at the Nippon Medical School Hospital were investigated. Of these 42 patients, 3 had been treated with epoetin beta pegol. Therefore, we excluded these three patients to ensure homogeneity in the ESA used in the study; all the enrolled patients were administered only darbepoetin alfa (n = 39).
Plasma EPO was measured before ESA administration at the regular outpatient visits and then at 2 weeks after the final dose of ESA was administered in all the study subjects; as a general practice, we administered ESA to patients undergoing PD during their regular outpatient visits.
Information about the following variables were collected: body mass index; primary disease; PD vintage; dialysate creatinine to plasma creatinine ratio (D/P ratio); dialysate glucose to initial dialysate glucose ratio (D/D ratio); urinary volume; dialysate dose; intake of renin–angiotensin system inhibitor (RASi), beta blocker, statin, diuretic, and iron supplementation; New York Heart Association (NYHA) classification, interventricular septum diameter, posterior wall diameter (PWd), left ventricular end-diastolic diameter, left ventricular end-systolic diameter (LVD), left ventricular mass index (LVMI), left ventricle ejection fraction (EF), early to late diastolic transmitral flow velocity (E/A), and cardiac index; peritoneal, renal, and weekly KT/V urea; peritoneal, renal, and weekly creatinine clearance (CCr); estimated glomerular filtration rate at the start of PD; ESA dose; plasma EPO; red blood cell, hemoglobin (Hb), hematocrit, reticulocyte, iron (Fe), transferrin saturation (TSAT), and ferritin; cardiothoracic ratio (CTR); N-terminal pro-brain natriuretic peptide (NT-proBNP); and lactate, serum calcium (Ca), serum phosphorus (P), intact parathyroid hormone, serum sodium (Na), serum potassium (K), serum chlorine (Cl), blood urea nitrogen, serum creatinine (Cr), serum total protein, serum albumin, C-reactive protein, serum beta 2 microglobulin, and venous pH.
Correlations with plasma EPO
To estimate the effectiveness of plasma EPO in patients undergoing PD, we assessed the correlations between the plasma EPO and other parameters, such as the NYHA classification.
Logistic regression analysis for HF risk
We defined HF as NYHA classification II in this analysis; none of the patients was classified into NYHA classifications III and IV. Univariate and multivariate logistic regression models were constructed for the risk for HF to estimate the effectiveness of plasma EPO and other factors on HF treatment in patients undergoing PD.
Statistical analyses
All the laboratory data are presented as mean ± standard deviation values. P values < 0.05 were considered to indicate statistical significance. All the statistical analyses were performed using Prism® software version 8 (GraphPad Software, La Jolla, CA, USA). Furthermore, logistic regression analyses were performed using JMP® software version 12 (SAS Institute, Cary, NC, USA).
Results
Baseline characteristics of the participants
A total of 39 patients were included in this study (28 men and 11 women); the average patient age was 63.23 ± 12.52 years. The most prevalent primary disease was diabetes mellitus that was present in 19 patients (48.7%). The mean PD vintage was 19.41 ± 21.73 months. The average plasma EPO level was 7.933 ± 5.494 (mIU/mL); 37 patients (94.9%) received ESA, darbepoetin alfa, and the mean dose of darbepoetin alfa was 127.3 ± 78.46 (μg/mon). We estimated the cardiac ultrasonography of patients and categorized them as per the NYHA classification. Thirty patients had NYHA classification I, and nine had NYHA classification II. None of the subjects had NYHA classifications III or IV. The baseline characteristics of the patients are shown in Table 1.
Correlations with the plasma EPO
The plasma EPO concentration was positively correlated with the ESA dose (r = 0.401, p = 0.011) and negatively correlated with Fe (r = − 0.382, p = 0.016), TSAT (r = − 0.443, p = 0.005), and BMI (r = − 0.328, p = 0.041) and showed no correlation with other factors, such as NYHA classification (r = 0.082, p = 0.620) and ferritin level (r = 0.239, p = 0.144). These results have been detailed in Fig. 1.

Correlations with the plasma erythropoietin level. a Correlation between the plasma erythropoietin (EPO) and erythropoiesis-stimulating agent (ESA). b Correlation between the plasma erythropoietin (EPO) and the serum ferrum level (Fe). c Correlation between the plasma erythropoietin (EPO) and transferrin saturation (TSAT). d Correlation between the plasma erythropoietin (EPO) and body mass index (BMI). e Correlation between the plasma erythropoietin (EPO) and the New York Heart Association (NYHA) classification. ESA erythropoiesis-stimulating agent, EPO plasma erythropoietin level, Fe serum ferrum level, TSAT transferrin saturation, BMI body mass index, NYHA the New York Heart Association
Logistic regression analysis for HF risk
In univariate analysis, the factors significantly associated with HF risk were NT-pro BNP [odds ratio (OR) 1.000078, 95% confidence interval (CI) 1.000025–1.000172, p = 0.0007], CTR (OR 1.269442, 95% CI 1.073978–1.583753, p = 0.0036), Cr (OR 1.43447, 95% CI 1.113463–2.001897, p = 0.00036), serum beta 2 microglobulin (OR 1.123, 95% CI 1.031–1.249, p = 0.006), dialysate dose (OR 1.001, 95% CI 1.000–1.001, p = 0.010), LVMI (OR 1.026, 95% CI 1.004–1.053, p = 0.0160), LVDs (OR 1.121, 95% CI 1.015–1.268, p = 0.024), LVDd (OR 1.142, 95% CI 1.010–1.331, p = 0.033), and weekly Kt/V (OR 5.163, 95% CI 1.113–32.723, p = 0.036). Plasma EPO was not significantly associated with the risk of HF (OR 1.033, 95% CI 0.894–1.175, p = 0.620) in the univariate analysis.
We concluded that NT-pro BNP, CTR, and Cr are the factors that are most significantly correlated with the risk of HF. Therefore, we performed a multivariate analysis with these three factors because of the required number of participants to allow robust statistical analyses and clinical importance of these factors. CTR (OR 1.713855, 95% CI 1.180244–3.431239, p = 0.0012), Cr (OR 1.902729, 95% CI 1.163817–4.348514, p = 0.0067), and NT-pro BNP (OR 1.000072, 95% CI 1.000006–1.000198, p = 0.0295) remained significant factors in multiple analysis; all three factors were significant in multiple analysis. The results are shown in Table 2.
Discussion
Renal anemia is a very common complication of CKD [1] and is important in patients undergoing dialysis. The 2012 Kidney Disease: Improving Global Outcomes Clinical Practice Guideline for Anemia in CKD recommends that the Hb levels be maintained at 9–11.5 g/dL in these patients [11]. Another report recommended the modulation of the ESA dose to maintain Hb levels between 10 g/dL and 11 g/dL [12]. In Japan, the target Hb level in patients on PD is 11–13 g/dL [13]; therefore, we modulate the dose of ESAs, such as darbepoetin alfa and epoetin beta pegol, in patients undergoing PD. The subcutaneous administration of darbepoetin alfa is safe and effective in patients undergoing PD [14, 15]; both darbepoetin alfa and epoetin beta pegol are effective in maintaining the target Hb level in patients undergoing PD [16]. PD may be an additional treatment for refractory HF [17]; however, HF is one of the most important causes of death in patients undergoing dialysis [2] and is an important cause of hospitalization in patients undergoing PD [3]. Therefore, prognosis prediction and control of HF are extremely important in patients undergoing PD. CTR and NT-proBNP are associated with HF [18, 19], and NT-proBNP was shown to be an effective prognostic marker for HF in patients undergoing PD [20]; therefore, these parameters have been used as the conventional prognostic markers for HF in patients undergoing PD. Moreover, CTR, NT-proBNP, and the other parameters can be used to comprehensively estimate a patient’s condition, predict the prognosis, and manage HF in patients on PD; however, the use of these variables involves limitations, and more efficient systems are required.
In patients with HF, the reported prevalence of anemia is 25–40% and is associated with the risk of hospitalization and death [4,5,6,7]. High plasma EPO has been associated with patient prognosis in those with HF, independent of the Hb levels [5, 9]. Moreover, in a report on patients with renal failure, the average eGFR of the patients was 47.1 mL/min/1.73 m2, and high plasma EPO was a risk factor for worse prognosis, irrespective of the presence of anemia or renal failure [10]. However, low endogenous EPO is reported to be a major cause of renal anemia [1, 8], and a decrease in the endocrine renal function is associated with excretory renal function [8]. Compared to endogenous EPO, recombinant human EPO has the same amino acid sequence but a slightly different sugar profile [21]. Moreover, all ESAs, such as recombinant human EPO, possess the ability to bind to and activate the EPO receptor [21]. The primary way of EPO and recombinant human EPO clearance is via the EPO receptor in the bone marrow, not in the kidney or the liver [21, 22]. Darbepoetin alfa has a longer half-life than epoetin alfa, the first ESA [23]. The terminal half-life of subcutaneous darbepoetin alfa is about 70 h in patients with CKD not undergoing dialysis [24]. Moreover, the pharmacokinetics of intravenous recombinant human EPO is similar between patients with normal renal function and those with CKD, including those undergoing hemodialysis and PD [25]. Renal anemia in CKD is associated with a relative deficiency of EPO [26]. In a previous trial, the plasma EPO level was higher in patients with CKD not undergoing dialysis than that in healthy people, owing to some causes although the patients with CKD were moderately anemic; increase in the liver EPO synthesis in patients with CKD and anemia was presumed to be the reason for this finding [27]. In contrast, another study reported that the frequent use of angiotensin-converting enzyme inhibitors and angiotensin receptor blockers for patients with CKD may inhibit EPO production and its effect on the bone marrow [28]. In patients with CKD and anemia who are undergoing treatment, several complicating mechanisms may be involved in the maintenance of the Hb levels.
We hypothesized that the plasma EPO level in patients undergoing PD was associated with HF, as observed in patients before undergoing dialysis because the residual renal function is commonly observed more in those undergoing PD than in those undergoing hemodialysis. However, in this study, the plasma EPO level was not correlated with the HF parameters, such as NYHA classification; however, the ESA dose, Fe, TSAT, and BMI were correlated with the plasma EPO levels.
In this study, the plasma EPO level was positively correlated with the monthly dose of ESA; therefore, its level in patients undergoing PD may only have reflected in the ESA dose. Furthermore, the plasma EPO level was not correlated with both, the Hb level and reticulocyte count, as well as the residual renal function parameters, such as sβ2MG, weekly renal KT/V, and weekly renal CCr. These results were similar to those of a previous study that reported that there was no association between residual renal function and ESA dose in patients undergoing HD and PD [29]. Fe, TSAT, and BMI were correlated to the plasma EPO level in this study. The association of Fe and TSAT with the plasma EPO may be attributable to the defective iron utilization in patients undergoing PD in this study. The negative correlations of the plasma EPO level with Fe and TSAT in this study suggested that a high plasma EPO level increased erythropoiesis and subsequently lowered the serum Fe and TSAT and that the more frequent use of ESA in anemic patients may be beneficial. In contrast, reticulocyte count was not correlated with plasma EPO. Ferritin levels were not associated with the plasma EPO level. Although the difference between TSAT and ferritin may be associated with defective iron utilization or inflammation in patients on PD, we could not explain these mechanisms clearly in this study. Further research is necessary for clarity on this subject. In this study, BMI was also related to the plasma EPO level. The negative correlation suggested the possibility of an association between the plasma EPO level and BMI, although we were unable to clearly determine the underlying mechanism in this study.
Based on this study, although we hypothesized that the plasma EPO level in patients undergoing PD was associated with HF, the present results suggested that the plasma EPO level in patients undergoing PD may not be useful for managing HF, unlike its use in patients with CKD not undergoing dialysis.
As per the univariate analysis, NT-pro BNP, CTR, serum Cr, serum beta 2 microglobulin, dialysate dose, LVMI, LVDs, LVDd, and weekly Kt/V were significantly associated with the risk of HF. On the other hand, plasma EPO were not associated with the risk of HF significantly in the univariate analysis. Therefore, the plasma EPO level in patients undergoing PD may not be effective in HF management.
As mentioned above, NT-pro BNP and CTR are known conventional markers of HF. In addition to the results of the univariate analysis, these two factors were also found to be significantly associated with HF risk in the multivariate analysis. Therefore, these results were in agreement with most previous reports; however, the value of OR of NT-pro BNP was so small in this study. Some reasons that the large value of NT-pro BNP and not including participants with NYHA classification > III might affect the result in this study. The significance of serum Cr, serum beta 2 microglobulin, and dialysate dose suggests that residual renal function may be associated with the NYHA classification; serum Cr was also associated with the NYHA classification significantly in multivariate analysis. However, further research is necessary because there were some problems that the other factors associated with residual renal function such as renal Kt/V and urinary volume were not significant in this study to prove the effectiveness of those factors.
LVMI, LVDs, and LVDd were found to show significant associations with HF risk in the univariate analysis. Although left ventricular hypertrophy may be associated with the NYHA classification, more precise investigations are required to confirm this finding.
Anemia has been associated with HF [4]; although this study did not show a similar result, the factors of anemia, such as Hb and hematocrit, were not significant in this study. This discrepancy may be accounted for by the fact that in our patients, anemia was managed with ESA treatment and that the average Hb level of the study subjects was 10.72 ± 1.266 g/dL. Nevertheless, these results may have been influenced by some biases, such as the relatively small sample size in this study. Additional research is required to confirm these findings.
This study has some limitations. First, it was a single-center study, and the sample size was relatively small. Second, patients with NYHA classification > III were not included. Third, we excluded patients treated with epoetin beta pegol to ensure homogeneity in the ESA used in this study. Finally, we did not distinguish whether the plasma EPO was endogenous or exogenous. These limitations might have introduced certain biases in this study.
Conclusions
The plasma EPO level in patients undergoing PD was positively correlated with the monthly ESA dose and was not significant as a marker of HF, as judged with the NYHA classification. Therefore, the plasma EPO level may not be a useful marker for HF in patients undergoing PD.
Availability of data and materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BMI:
-
Body mass index
- RASi:
-
Renin angiotensin system inhibiter
- CKD:
-
Chronic kidney disease
- PD:
-
Peritoneal dialysis
- HF:
-
Heart failure
- EPO:
-
Erythropoietin
- ESA:
-
Erythropoiesis-stimulating agents
- NYHA:
-
New York Heart Association
- PWd:
-
Posterior wall diameter
- LVD:
-
Left ventricular end-systolic diameter
- LVMI:
-
Left ventricular mass index
- EF:
-
Ejection fraction
- CCr:
-
Creatinine clearance
- Fe:
-
Iron
- CTR:
-
Cardiothoracic ratio
- NT-proBNP:
-
N-terminal pro-brain natriuretic peptide
- OR:
-
Odds ratio
- CI:
-
Confidence interval
- eGFR:
-
Estimated glomerular filtration rate
- RBC:
-
Red blood cell
- Hb:
-
Hemoglobin
- Ht:
-
Hematocrit
- TIBC:
-
Toral iron binding capacity
- iPTH:
-
Intact parathyroid hormone
- BUN:
-
Blood urea nitrogen
- TP:
-
Serum total protein
- Alb:
-
Serum albumin
- CRP:
-
C-reactive protein
- sβ2MG:
-
Serum beta 2 microglobulin
References
Mimura I, Tanaka T, Nangaku M. How the target hemoglobin of renal anemia should be. Nephron. 2015;131(3):202–9 Available from: https://www.ncbi.nlm.nih.gov/pubmed/26381503.
Masakane I, Nakai S, Ogata S, et al. An overview of regular dialysis treatment in Japan (As of 31 December 2013). Ther Apher Dial. 2015;19(6):540–74 Available from: https://www.ncbi.nlm.nih.gov/pubmed/26768810.
Mitsnefes MM. Cardiovascular morbidity and mortality in children with chronic kidney disease in North America: lessons from the USRDS and NAPRTCS databases. Perit Dial Int. 2005;25(Suppl 3):S120–2 Available from: https://www.ncbi.nlm.nih.gov/pubmed/16048275.
Kleijn L, Westenbrink BD, van der Meer P. Erythropoietin and heart failure: the end of a promise? Eur J Heart Fail. 2013;15(5):479–81 Available from: https://www.ncbi.nlm.nih.gov/pubmed/23558218.
Mastromarino V, Volpe M, Musumeci MB, Autore C, Conti E. Erythropoietin and the heart: facts and perspectives. Clin Sci (Lond). 2011;120(2):51–63 Available from: https://www.ncbi.nlm.nih.gov/pubmed/20929439.
Groenveld HF, Januzzi JL, Damman K, et al. Anemia and mortality in heart failure patients a systematic review and meta-analysis. J Am Coll Cardiol. 2008;52(10):818–27 Available from: https://www.ncbi.nlm.nih.gov/pubmed/18755344.
Grote Beverborg N, van Veldhuisen DJ, van der Meer P. Anemia in Heart Failure: Still Relevant? JACC Heart Fail. 2018;6(3):201–8 Available from: https://www.ncbi.nlm.nih.gov/pubmed/29128254.
Radtke HW, Claussner A, Erbes PM, Scheuermann EH, Schoeppe W, Koch KM. Serum erythropoietin concentration in chronic renal failure: relationship to degree of anemia and excretory renal function. Blood. 1979;54(4):877–84 Available from: https://www.ncbi.nlm.nih.gov/pubmed/476305.
van der Meer P, Voors AA, Lipsic E, Smilde TD, van Gilst WH, van Veldhuisen DJ. Prognostic value of plasma erythropoietin on mortality in patients with chronic heart failure. J Am Coll Cardiol. 2004;44(1):63–7 Available from: https://www.ncbi.nlm.nih.gov/pubmed/15234408.
Nagai T, Nishimura K, Honma T, et al. Prognostic significance of endogenous erythropoietin in long-term outcome of patients with acute decompensated heart failure. Eur J Heart Fail. 2016;18(7):803–13 Available from: https://www.ncbi.nlm.nih.gov/pubmed/27126377.
Kliger AS, Foley RN, Goldfarb DS, et al. KDOQI US commentary on the 2012 KDIGO Clinical Practice Guideline for Anemia in CKD. Am J Kidney Dis. 2013;62(5):849–59 Available from: https://www.ncbi.nlm.nih.gov/pubmed/23891356.
Liu H, Yao Y, Cao Y, et al. Anemia management trends in patients on peritoneal dialysis in the past 10 years. Int J Clin Exp Med. 2015;8(10):18050–7 Available from: https://www.ncbi.nlm.nih.gov/pubmed/26770400.
Tsubakihara Y, Nishi S, Akiba T, et al. 2008 Japanese Society for Dialysis Therapy: guidelines for renal anemia in chronic kidney disease. Ther Apher Dial. 2010;14(3):240–75 Available from: https://www.ncbi.nlm.nih.gov/pubmed/20609178.
Theodoridis M, Passadakis P, Kriki P, et al. Efficient monthly subcutaneous administration of darbepoetin in stable CAPD patients. Perit Dial Int. 2005;25(6):564–9 Available from: https://www.ncbi.nlm.nih.gov/pubmed/16411523.
Kubota M, Hiramatsu M, Yamakawa M, et al. Darbepoetin alfa (KRN321) is safe and effective when administered subcutaneously once every 2 or 4 weeks to patients on peritoneal dialysis in Japan. Clin Exp Nephrol. 2011;15(6):884–92 Available from: https://www.ncbi.nlm.nih.gov/pubmed/21898029.
Washida N, Inoue S, Kasai T, et al. Impact of switching from darbepoetin alfa to epoetin beta pegol on iron utilization and blood pressure in peritoneal dialysis patients. Ther Apher Dial. 2015;19(5):450–6 Available from: https://www.ncbi.nlm.nih.gov/pubmed/25944557.
Puttagunta H. Holt SG. Peritoneal dialysis for heart failure. Perit Dial Int. 2015;35(6):645–9 Available from: https://www.ncbi.nlm.nih.gov/pubmed/26702006.
Januzzi JL, van Kimmenade R, Lainchbury J, et al. NT-proBNP testing for diagnosis and short-term prognosis in acute destabilized heart failure: an international pooled analysis of 1256 patients: the International Collaborative of NT-proBNP Study. Eur Heart J. 2006;27(3):330–7 Available from: https://www.ncbi.nlm.nih.gov/pubmed/16293638.
Giamouzis G, Sui X, Love TE, Butler J, Young JB, Ahmed A. A propensity-matched study of the association of cardiothoracic ratio with morbidity and mortality in chronic heart failure. Am J Cardiol. 2008;101(3):343–7 Available from: https://www.ncbi.nlm.nih.gov/pubmed/18237597.
Wang AY, Lam CW, Yu CM, et al. N-terminal pro-brain natriuretic peptide: an independent risk predictor of cardiovascular congestion, mortality, and adverse cardiovascular outcomes in chronic peritoneal dialysis patients. J Am Soc Nephrol. 2007;18(1):321–30 Available from: https://www.ncbi.nlm.nih.gov/pubmed/17167121.
Elliott S, Pham E, Macdougall IC. Erythropoietins: a common mechanism of action. Exp Hematol. 2008;36(12):1573–84 Available from: https://www.ncbi.nlm.nih.gov/pubmed/18922615.
Jelkmann W. The enigma of the metabolic fate of circulating erythropoietin (Epo) in view of the pharmacokinetics of the recombinant drugs rhEpo and NESP. Eur J Haematol. 2002;69(5-6):265–74 Available from: https://www.ncbi.nlm.nih.gov/pubmed/12460230.
Wilhelm-Leen ER, Winkelmayer WC. Mortality risk of darbepoetin alfa versus epoetin alfa in patients with CKD: systematic review and meta-analysis. Am J Kidney Dis. 2015;66(1):69–74 Available from: https://www.ncbi.nlm.nih.gov/pubmed/25636816.
Padhi D, Ni L, Cooke B, Marino R, Jang G. An extended terminal half-life for darbepoetin alfa: results from a single-dose pharmacokinetic study in patients with chronic kidney disease not receiving dialysis. Clin Pharmacokinet. 2006;45(5):503–10 Available from: https://www.ncbi.nlm.nih.gov/pubmed/16640455.
Takama H, Tanaka H, Nakashima D, et al. Population pharmacokinetics of darbepoetin alfa in haemodialysis and peritoneal dialysis patients after intravenous administration. Br J Clin Pharmacol. 2007;63(3):300–9 Available from: https://www.ncbi.nlm.nih.gov/pubmed/16945116.
Mercadal L, Metzger M, Casadevall N, et al. Timing and determinants of erythropoietin deficiency in chronic kidney disease. Clin J Am Soc Nephrol. 2012;7(1):35–42 Available from: https://www.ncbi.nlm.nih.gov/pubmed/22096037.
de Seigneux S, Lundby AK, Berchtold L, Berg AH, Saudan P, Lundby C. Increased synthesis of liver erythropoietin with CKD. J Am Soc Nephrol. 2016;27(8):2265–9 Available from: https://www.ncbi.nlm.nih.gov/pubmed/26757994.
Sirbu O, Floria M, Dascalita P, et al. Anemia in heart failure - from guidelines to controversies and challenges. Anatol J Cardiol. 2018;20(1):52–9 Available from: https://www.ncbi.nlm.nih.gov/pubmed/29952364.
Louw EH, Chothia MY. Residual renal function in chronic dialysis is not associated with reduced erythropoietin-stimulating agent dose requirements: a cross-sectional study. BMC Nephrol. 2017;18(1):336 Available from: https://www.ncbi.nlm.nih.gov/pubmed/29178879.
Acknowledgements
The authors thank all the participants and the staffs of the Nippon Medical School Hospital Blood Purification Center.
Funding
None
Author information
Authors and Affiliations
Contributions
KT drafted the first manuscript. YSu, AH, SA, TK, and YSa managed the patient. YSa coordinated the data analysis and helped with writing the manuscript. All authors participated in discussions and read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Ethical Committee of the Nippon Medical School Hospital (B-2020-121) and designed in accordance with the Declaration of Helsinki. The study was registered to the University Hospital Medical Information Network (UMIN No.000041146).
Consent for publication
Not applicable.
Competing interests
There are no conflicts of interest to declare in this study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Terada, K., Sumi, Y., Aratani, S. et al. Plasma erythropoietin level and heart failure in patients undergoing peritoneal dialysis: a cross-sectional study. Ren Replace Ther 7, 3 (2021). https://doi.org/10.1186/s41100-021-00319-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41100-021-00319-x