
Abstract
Hyperphosphatemia is a risk factor for cardiovascular disease and mortality in individuals with end-stage kidney disease (ESKD). Thus, it represents a potential target for interventions to improve clinical outcomes in ESKD. Phosphorus reduction therapy for maintained hemodialysis (MHD) patients encompasses phosphate binder medication, adequate dialysis, and also dietary phosphorus control. The main strategy in achieving dietary phosphorus reduction involves intensive education by a dietitian. The purposes of this patient education process are: (a) to obtain patient background information, (b) to assess patient knowledge, (c) to evaluate patient nutritional status, (d) to educate the patient using various approaches, and (e) to optimize the patient’s nutritional state. Here, we review the management of dietary phosphorus by dietitians and summarize our strategy and the activities we use in diet counseling for MHD patients.
Similar content being viewed by others



Background
The occurrence of kidney disease and subsequent kidney failure continues to increase throughout Japan. By the end of 2012, the number of patients on dialysis reached as high as 300,000 [1]. It is currently estimated that more than 13,300,000 people suffer from chronic kidney disease (CKD) [2]. In CKD, progressive impairment of kidney function leads to the retention of many substances, including potassium and phosphorus. Thus, hyperphosphatemia is a common secondary complication in patients with end-stage kidney disease (ESKD). This complication is a consequence of the reduction in filtered phosphate load, which subsequently plays an important role in the development of renal osteodystrophy and in the increased risk of mortality and cardiovascular diseases [3,4,5,6].
Phosphate homeostasis is maintained through the concerted action of various hormones and factors in the intestine, kidney, and skeleton [7, 8]. Following further impairment of residual renal function in people with CKD, the reduction in phosphate excretion breaks down this complex balance and induces hyperphosphatemia. The management of serum phosphate is therefore vital for reducing the risk of mortality and cardiovascular events. Such management requires a multi-factorial approach, including appropriate use of phosphate-binding agents, delivery of an adequate dose of renal replacement therapy, and dietary restriction of phosphate [9,10,11,12,13]. Medical staff caring for maintained hemodialysis (MHD) patients often face difficulties in successfully implementing phosphate management.
Previous studies suggested that patient education may improve phosphate control, patient knowledge about dietary phosphorus, and patient compliance to an adequate diet regimen—variables essential to maintaining phosphorus at acceptable levels [14, 15]. Herein, we review the management of dietary phosphorus intake for MHD patients and introduce our approach for improving dietitians’ skills at educating MHD patients.
The physiological role of dietary phosphorus
Phosphorus is an essential mineral used for growth and repair of the body’s cells and tissues [8] and serves as a vital component of an array of biologically active molecules such as nucleic acids, signaling proteins, phosphorylated enzymes, and cell membranes. While some phosphorus is stored in tissues throughout the body, most (85%) is present in the body as phosphate within bones and teeth. However, phosphorus is continuously in flux between the bone and extracellular fluid, and all tissues can absorb and secrete phosphate to meet physiological demands.
Phosphate homeostasis is a complex, highly regulated process. In individuals with CKD, the serum phosphorus concentration is usually maintained within the normal range (2.5 to 4.5 mg/dl) by a variety of compensatory mechanisms until CKD has progressed to stage 5 or become ESKD [16]. In ESKD patients who lose the ability to excrete excess phosphorus, the extent of phosphorus retention depends on the patient’s intake of phosphorus-containing food [17]. Therefore, the management of dietary phosphorus is critical throughout the progressive course of kidney disease, up to dialysis-dependent end-stage renal failure.
Dietary sources of phosphorus
Because phosphorus is found in a wide variety of foods, complying with a dietary phosphorus restriction is very challenging for MHD patients. Kalantar-Zadeh et al. demonstrated a strong linear correlation (R 2 = 0.83) between dietary protein and phosphorus content (Fig. 1). This correlation yields a regression equation that can be used to estimate daily phosphorus intake from daily protein intake in MHD patients. On average, the ratio of phosphorus to protein is 15 mg of phosphorus per gram of protein [11]. The Japanese Society for Dialysis Therapy recommendation for MHD patients is a phosphorus intake of (1.2–1.4 mg/day/kg) × 15 mg/day.

Estimated phosphorus intake (in mg/dl) calculated from daily protein intake (in g/d) in 107 MHD patients from the NIED study. This figure was kindly provided by Prof. Kalantar-Zadeh. Regression equation: phosphorus = 11.8 protein + 78 (r = 0.91, P = 0.001)
Information reporting the phosphorus content as milligram per gram of protein (mg/g protein) is especially useful to identify which foods supply less phosphorus for the same amount of protein. Dietitians recommend foods and supplements with an inorganic phosphorus-protein ratio of less than 10 mg/g. Analyses of phosphorus content (mg/100 g edible portion) in various natural food groups have shown that the highest phosphorus load comes from nuts, hard cheeses, egg yolks, meat, poultry, and fish [17,18,19,20,21]. Rather than compelling patients to give up their favorite foods, dietitians aim to provide appropriate recommendations and practical information. For example, rather than eliminating eggs entirely, patients can be advised to instead consume fresh, non-processed egg white (which has a phosphorus-protein ratio less than 2 mg/g), because egg white contains a high amount of essential amino acids and low amounts of fat, cholesterol, and phosphorus [22].
In addition to assessing food based on its phosphorus content as milligram per gram of protein, the protein digestibility-corrected amino acid score (PDCAAS) can also be used for the management of dietary phosphorus. PDCAAS is a method for evaluating protein quality based on both human requirements for, and the ability to digest, amino acids. Because the formula for calculating the PDCAAS is very complicated, dietitians perform the calculations and use the assessment for educating patients [23].
Almost all foods contain phosphorus, although the actual intake of phosphorus depends upon the total amount of phosphorus in the diet and its bioavailability. In healthy individuals, the recommended dietary intake for phosphorus is 1000 mg/day for men and 800 mg/day for women (for further information, see Overview of Dietary intakes for Japanese 2015 [2]). In fact, total dietary phosphorus comes from three different sources which are thought to have different bioavailability and physiologic roles: (1) naturally occurring organic phosphorus, which serves as a component of cell membranes, tissue structures, and phosphoprotein; (2) inorganic phosphorus, which is added during food processing and is present to a lesser extent in naturally occurring phosphorus salts; and (3) inorganic phosphorus present as an active or inactive ingredient in over-the-counter medications, common prescription medications, dietary supplements, and food enrichment/fortification substances (Table 1) [20].
-
1.
Dietary organic phosphorus
-
(a)
Phosphorus from animal protein
The main dietary sources of phosphorus are members of the protein food group: meat, poultry, fish, eggs, and dairy products. Animal- and plant-based foods both each have high organic phosphorus content. However, different sources of animal protein contain different proportions of phosphorus. For example, Noori et al. showed that the amount of phosphorus in egg white is much less than in egg yolk or poultry (e.g., chicken, turkey) and that fish contain less phosphorus than the equivalent amount of red meat (e.g., beef, veal). Following ingestion, between 40 and 60% of animal-based phosphorus is absorbed; this varies by the degree of gastrointestinal vitamin receptor activation [24]. However, meat and dairy products are frequently supplemented with phosphate additives, which may markedly increase the total phosphorus content. Ando et al. recently reported that boiling food in soft water and cooking sliced food in a pressure cooker are preferable cooking procedures for MHD patients as these procedures reduce phosphorus content while preserving protein content [25].
-
(b)
Phosphorus from plants
Many fruits and vegetables contain only small amounts of organic phosphate, but some seeds and beans such as cacaos and soy possess a high phosphorus content. In plants—especially beans, peas, and nuts—phosphorus is present mostly in the storage form of phytic acid or phytate. Because humans lack the digestive enzymes to degrade phytate, plant phosphorus in its predominant phytate form is less absorbable. In contrast to animal-based foods, phosphorus absorption from plant-based foods by the human gastrointestinal tract is usually less than 40%. Therefore, a diet relying on plant protein rather than animal protein would presumably lead to better management of a patient’s phosphorus burden [22, 26]. However, Noori et al. noted that there are three important caveats to this plant-based diet. First, the yeast-based phytate in whole grains makes the phosphorus content of leavened breads more effectively absorbed than the phosphorus content of cereals or flat breads. Second, the effects of probiotics on enhancing phytate-associated phosphorus release and absorption are currently unknown. Third, the biological value (quality) of plant proteins tends to be lower than that of animal proteins, and for people with marginal protein intakes, this could leads to inadequate protein nutrition [24].
-
(c)
Rice as a major Japanese food
Rice is a staple food for Japanese people. In Japan, the average daily consumption per person reaches 155 g/day and, in the form of steamed rice, becomes 330 g/day [2]. Kanno et al. [27] and Watanabe et al. [28] reported that phosphorus intake is reduced by using wash-free rice. Uehara et al. [29] demonstrated that five rounds of washing polished rice for 20 s each could reduce its amount of phosphorus. Given that special protein-controlled rice for CKD patients is very expensive (usually 2.5 to 4.5 times the expense of ordinary steamed rice), it is economically better for patients to instead eat polished rice and/or well-washed rice.
-
(a)
-
2.
Inorganic phosphorus from food additives
Phosphorus is the main component of many preservatives and additive salts found in processed foods (e.g., as an acidifier emulsifier or adhesive agent in foods such as processed cheese and some carbonated drinks) (Fig. 2). Additives are used in food processing for a variety of purposes such as extending shelf life, improving color, enhancing flavor, and retaining moisture [20, 30]. The presence of inorganic phosphorus in foods is often obscured by the use of complex names or ingredients on food labels (Fig. 3). Importantly, almost all the inorganic phosphorus in processed foods can be absorbed.
Fig. 2 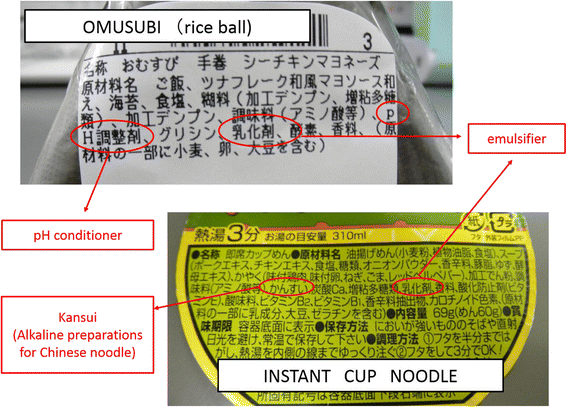
Phosphorus is not directly listed in food ingredients. Instead, phosphate-containing pH conditioners, emulsifiers, and/or kansui (an alkaline preparation for Chinese noodles) are included
Fig. 3 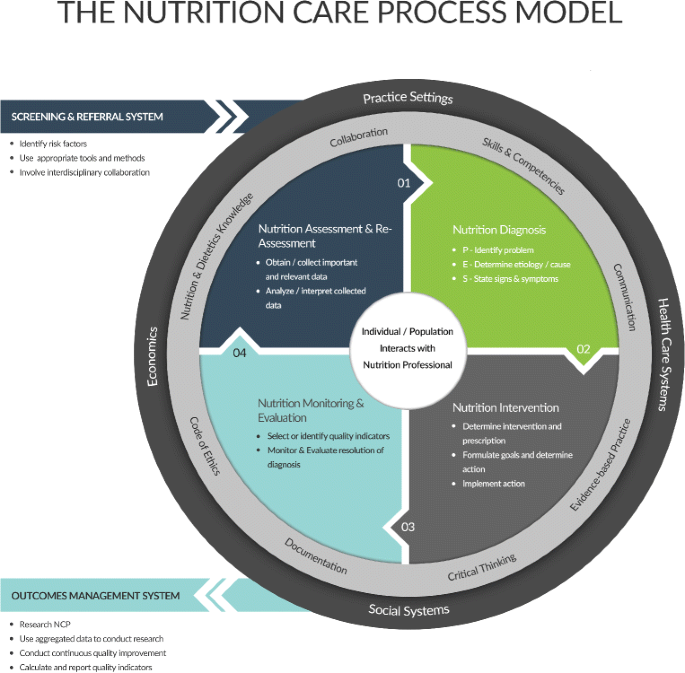
The Nutrition Care Process (NCP) model. Permission to use this figure has been obtained from the Academy of Nutrition and Diabetes (USA). This model is a graphic visualization that illustrates the steps of the NCP as well as internal and external factors that impact application of the NCP. The central component of the model is the relationship of the target patients or group and the registered dietitian and nutritionist (RDN). One of the two outer rings represents the skill and abilities of the RDN along with application of evidenced-based practice, application of the Code of Ethics, and knowledge of the RDN. The second of the outer rings represents environmental factors such as healthcare system, socioeconomics, and practice setting that impacts the ability of the target patient or group to benefit from RDN services
In the USA and other Western countries, the phosphorus added during processing contributes an average of 500 mg/day per capita. Depending on food preferences, these compounds can contribute from 300 mg to as much as a gram of phosphorus towards an individual’s daily intake. In Japan, both lifestyle and food preferences have changed and become more similar to those of Western cultures.
Phosphate additives are a serious concern for kidney patients at all stages of CKD. Specific preparation methods for processed foods can reduce the food’s amount of phosphorus [20, 25, 31, 32], Table 1. Recently, Takemasa et al. demonstrated that the phosphorus content in sausages could be reduced by chopping and boiling [30]. Similarly, Ando et al. [25] reported that boiling food in soft water and cooking sliced food in a pressure cooker could reduce phosphorus content while preserving protein content.


Nutritional counseling
Serum phosphate concentrations reflect the dynamic balance between dietary phosphorus absorption, urinary phosphorus excretion, and internal exchange with the bone, soft tissue, and intracellular stores [33]. In MHD patients—who possess severely limited urinary phosphorus excretion and still-efficient gut phosphorus absorption—dietary absorption is a critical determinant of serum phosphate concentration. The importance of dietary phosphate intake is further boosted by the widespread use of activated vitamin D analogs, which increase gut absorption of phosphorus [34], and by the relatively poor phosphate clearance provided by standard hemodialysis three times per week. Preventing gut absorption of dietary phosphorus either by restricting intake or prescribing oral phosphorus binders is currently the cornerstone of managing hyperphosphatemia in MHD patients.
Compared to phosphate binders, dietary phosphorus restriction is underutilized in MHD patients. This is likely due to fear of exacerbating protein energy wasting (PEW), the assumption that patients will be poorly compliant with yet another layer of dietary restriction in addition to those already in place (e.g., for fluid, salt) and the logistical challenges of continuous dietary counseling. In support of these concerns, some previous reports suggest that hemodialysis patients are less likely to adhere to a phosphate dietary restriction than to potassium, sodium, or fluid restriction [14, 35].
To help a patient successfully follow phosphate dietary restrictions, dietitians must listen attentively to patients’ concerns and actively identify issues to be solved in order to adequately manage serum phosphorus concentrations. Individual counseling, based on learning needs and preferences, is offered by dietitians to MHD patients with hyperphosphatemia [36,37,38]. This counseling includes advice on avoiding phosphate-rich foods and phosphate additives as shown in Tables 2 and 3. The dietary modification can be achieved through ongoing education from dietitians and other medical team members and through support from family and friends [39]. Towards this end, the Academy of Nutrition and Dietetics in the USA proposed the Nutrition Care Process (NCP). This systematic approach provides high-quality nutrition care through the following four steps: (1) nutrition assessment and reassessment, (2) nutrition diagnosis, (3) nutrition intervention, and (4) nutrition monitoring and evaluation [40, 41]; Fig. 3.
A number of large studies have examined the association between educational attainment and outcomes in patients with kidney disease. In an analysis of 61,457 participants in the Kidney Early Evaluation Program, lower educational attainment was independently associated with reduced kidney function and increased mortality [42]. Several interrelated pathways have been proposed to explain the relationship between educational attainment and health including (a) health knowledge and behaviors, (b) employment and income [43], and (c) social and psychological factors. In particular, education contributes to health by improving health knowledge, affording adequate health literacy, and improving coping and problem-solving skills [44, 45]. These advantages allow patients to make better decisions about their health, engage in healthy behaviors, and self-manage their medical conditions [46].
Successful control of diet is often challenging, and the availability of a variety of educational resources is very beneficial when working with patients and their families [47]. In an ideal situation, patients are allowed to learn at their own speed. Many medical teams have developed an array of educational tools that include written, visual, or auditory programs to instruct patients on how to effectively modify their diets. Dietitians in our hospital also evaluate and educate MHD patients using original question sheets and tools (Additional file 1; Tables 2, 3, and 4; Figs. 4, 5, and 6). Many patients have noted that altering diet behavior is one of the hardest challenges in adjusting to dialysis. A recent survey of nutrition trends in CKD patients showed that the greatest perceived obstacles to positive dietary change included the fear of giving up favorite foods, confusion regarding dietary recommendations, and false beliefs regarding the length of time required to prepare healthy foods.

Educational leaflets on dietary phosphorus made by the Kyoto working committee on food for dialysis patients. Leaflets address (a) carbonated beverages, (b) Japan McDonald’s, and Kentucky Fried Chicken Japan (c). Food information is published with permission from these companies

Leaflet on preparation methods for reducing phosphorus in processed food

Recipes on diet supplementation for avoiding PEW
Additional file 1: Movie of dietitian’s counseling. (MP4 185512 kb)
In addition to education, assessing patients’ knowledge is an important factor in estimating patient compliance to the renal diet [46, 47]. Dietitians initiate the processes of assessment and education in order to (1) establish communication with patients and their families, (2) provide information to address any underlying nutritional issues, and (3) calm the fears that many patients have regarding the implementation of the many changes required in their lives [48]. In support of this approach, Reddy et al. [41] found that an education program significantly improved patients’ general knowledge of phosphorus and phosphate binders and was associated with a significant reduction in serum phosphate in patients with hyperphosphatemia.
Knowledge of phosphate binders as common drugs prescribed to dialysis patients
Phosphate binders limit the absorption of dietary phosphorus into the body through the intestine, thus reducing the amount of phosphorus that enters the circulation. Usually, phosphate binders are taken 5–10 min before or immediately after meals and snacks. Dietitians should know that the combination of phosphate binders and adequate nutrition can help to avoid malnutrition. The two common types of phosphorus binders are calcium-based phosphate binders and calcium-free phosphate binders. New phosphate binders have been released recently, and dietitians also need to keep up with such developments [49].
Key points for patient education
In the first counseling session with a patient, dietitians should assess the patient’s level of understanding regarding phosphorus and hyperphosphatemia. The dietitian should then instruct the patient to:
-
(a)
Take vegetable-based protein rather than animal-based
-
(b)
Check the ingredient list (do not forget the phosphorus in popular beverages)
-
(c)
Reduce processed food consumption
-
(d)
Prepare and cook foods to reduce phosphorus content
-
(e)
Use food supplements to avoid PEW.
To convince patients to effectively control dietary phosphorus and protein intake, dietitians need to provide patients with educational resources, such as booklets or leaflets; demonstrate how to recognize and avoid inorganic phosphorus additives; show how to select protein sources and achieve protein adequacy; and explain to patients how to estimate the phosphorus content of chosen foods [50,51,52,53]. The dietitian should also advise that reading the additives listed in food labels on packages can help patients restrict consumption of phosphorus in processed and fast foods.
Monitoring of nutritional status
Regular evaluation of nutritional status includes the measurement of the percent usual body weight and percent standard body weight. Patients can also be evaluated using subjective global assessments, diet diaries, normalized protein catabolic rates, and renal laboratory evaluations. A renal laboratory evaluation should assay the following serum constituents: albumin, glucose, glycosylated hemoglobin and glycosylated albumin (for diabetic patients only), hematocrit, calcium, phosphate, calcium phosphate, potassium, and cholesterol. Results from these assays, when used with the national renal diet guidelines, can then assist renal dietitians in developing a nutrition plan that is appropriate for each patient [37].
Tools to measure body composition tools are extremely useful for the assessment of adult malnutrition at the bedside. Of the available tools, bioimpedance has been the most widely investigated in clinical research. This tool is used by clinicians for assessment purposes in Europe and elsewhere around the globe, in large part due to the affordability, portability, and ease of the use of bioimpedance devices [54]. A bioimpedance measurement takes less than 15 min and is completely noninvasive, making it advantageous for repeat measurements. We assess patient nutritional status using such impedance methods as those offered with the InBody bioimpedance device (InBody, Ltd., Tokyo, Japan).
Importance of avoiding PEW
Recent data indicate that imposed dietary phosphorus restriction may compromise the patient’s ability to achieve adequate protein intake, thereby leading to PEW and possibly to increased mortality. Thus, nutritional management is a critical component in CKD treatment as there is a high prevalence of PEW. The concept of PEW was proposed in 2007 by the International Society of Renal Nutrition and Metabolism [55]. This state is characterized by the simultaneous loss of systemic body protein and energy stores in patients with CKD, leading to the loss of both muscle and fat mass and cachexia [56, 57]. PEW is caused by hypercatabolic status, uremic toxins, malnutrition, and inflammation and is both exceptionally common and closely associated with mortality and morbidity in CKD patients [58, 59]. In a recent study, patients with CKD who exhibited serum albumin concentrations below 3.5 mg/dl had a higher rate of mortality [11]. To avoid PEW, the nutritional modifications for CKD patients include adjustments in dietary protein, sodium, potassium, and phosphate intake based on the patient’s nutritional status, which is regularly evaluated as described above.
The concept of PEW should be distinguished from malnutrition. CKD-related factors may contribute to the development of PEW; these factors occur in addition to or independent of inadequate nutrient intake due to anorexia and/or dietary restrictions.
Supplementation for MHD patients with malnutrition
The high prevalence of malnutrition in patients on dialysis, and the elevated protein requirements for patients on hemodialysis or peritoneal dialysis, have been documented [58, 59]. Poor appetite, inflammation, and protein loss during dialysis make it difficult for patients to achieve their nutritional targets, especially with regard to protein intake. Thus, we propose the use of protein supplements such as Enjoyprotein® (Clinico Co., Ltd., Tokyo, Japan), which has less potassium, and mid-chain fatty acids (MCFAs), which are well-absorbed fatty acids.
-
1)
Enjoyprotein®
This high-protein supplement has lower levels of both potassium and phosphorus, with a phosphate-to-protein ratio of 0.90 mg/g. The high amount of protein in this supplement helps CKD patients to take in adequate nutrition and to avoid PEW (Fig. 6).
-
2)
MCFA
In contrast to longer fatty acids, MCFAs are readily absorbed from the gastrointestinal tract and directly enter the portal system. Furthermore, MCFA absorption does not require modification, unlike with the absorption of long-chain or very-long-chain fatty acids. In addition, the digestion of MCFA does not require bile salts. Thus, MCFA supplementation is attracting attention as a means for ensuring adequate nutrition in patients with malnutrition or malabsorption. For such patients in our hospital, we cook rice porridges with Enjoyprotein and MCT oil (The Nisshin Oillio Group, Ltd., Tokyo, Japan), as described below.
-
3)
Chikara-gayu (rice porridge supplemented with Enjoyprotein® and MCT oil)
We cook chikara-gayu for malnutrition patients. This special porridge is prepared using the following ingredients (the taste is improved by adding salt):
-
1.
Porridge 150 g
-
2.
Nisshin MCT oil 9 g
-
3.
Enjoyprotein® 5.5 g
-
4.
Salt 0.42 g
Activities and approaches for dietitians
Team Kidney in Kyoto Katsura Hospital
Team Kidney was established in our hospital in 2015 as a team including nephrologists, pharmacists, nurses, clinical engineers, medical technologists, physiotherapists, dietitians, staffs of regional medical cooperative office, and medical secretaries. This multi-disciplinary team works cooperatively to prevent CKD progression by working with a regional medical network of general practitioners, planning educational events, and coordinating admissions to a nephrology ward. Figure 7 shows physiotherapists giving a lecture in a kidney disease seminar. As a part of the activities, nurses, dietitians, and sometimes medical doctors talk to hemodialysis patients about the importance of diet modification, particularly in terms of reducing phosphorus intake. To assess patient understanding, a questionnaire focused on phosphorus and hyperphosphatemia is administered to patients (Tables 2 and 3). Dietitians conduct counseling with the assistance of a handbook, and pharmacists educate the patients about effects of phosphorus-binding medications, vitamin D, cinacalcet, and other drugs.

Photo of a lecture by physiotherapists in Kyoto Katsura Hospital
Kyoto working committee on foods for dialysis patients
This society was established in 1973 in Kyoto for dietitians working at institutes with a dialysis unit and/or with MHD patients 5 years after renal replacement therapy was granted universal coverage under Japan’s National Health Insurance. The society aims to conduct research by surveying CKD patients’ nutrition and to identify meals suitable for MHD patients. Currently, 20 dietitians from 16 different institutes and dietitian training facilities belong to this society. One representative event is the annual cooking workshop for MHD patients (Fig. 8).

Photo of annual cooking lesson for dialysis patients
Task force consortium for kidney disease in Kyoto
This society was established in 1979 to promote activities preventing CKD progression. Nephrologists, pharmacists, dietitians, and patients with CKD are the members of the executive committee, which organizes lectures open to the public and provides a site for individual dietary counseling by specialists such as dietitians. The committee also conducted a survey of institutes in Kyoto Prefecture on approaches for preventing renal replacement therapy in diabetes patients. In 2015, traditional Japanese cuisine (Washoku) was added to UNESCO Intangible Cultural Heritage List. Washoku is considered among the most highly rated foods in terms of providing a balanced level of nutrients with low fat. However, Kyo-ryori (local cuisine in Kyoto) tends to have a higher salt content, which is linked to accelerated progression of CKD. Therefore, the society recently developed a new logo indicating adequate salt intake, the “Teki-en” (適塩 in Japanese), which would be much more acceptable for patients rather than the logo for reduced salt intake, “Gen-enn” (減塩 in Japanese) (Fig. 9). The society is involved in campaigns to educate patients about managing salt reduction.

Campaign logo for Teki-en (適塩, adequate salt intake)
Conclusions
Diet therapy for MHD patients is as integral to maintaining patient health as taking drugs and receiving adequate dialysis. The dietitian should be one of the principal specialists for educating patients about diet and how best to prepare their food. Open communication and a good rapport between dietitian and patient are vital to improving the patient knowledge and diet compliance. Over time, the work of dietitians will positively change patients’ lifestyles. We are confident that, through intensive nutritional intervention, we can prevent complications caused by hyperphosphatemia in ESKD.
Abbreviations
- CKD:
-
Chronic kidney disease
- ESKD:
-
End-stage kidney disease
- MCFA:
-
mid-chain fatty acid
- MHD:
-
Maintained hemodialysis
- NCP:
-
Nutrition Care Process
- PDCAAS:
-
Protein digestibility-corrected amino acid score
- PEW:
-
Protein energy wasting
References
Nakai S, Hanafusa N, Masakane I, Taniguchi M, Hamano T, Shoji T, et al. Overview of regular dialysis treatment in Japan (as of 31 December 2012). Ther Apheres Dial. 2014;18(6):535–602.
Overview of dietary reference intakes for Japanese (2015), http://www0.nih.go.jp/eiken/english/research/project_dris.html Accessed 1 Sep 2016.
Block GA, Hulbert-Shearon TE, Levin NW, Port FK. Association of serum phosphorus and calcium phosphate product with mortality risk in chronic hemodialysis patients: a national study. Am J Kidney Dis. 1998;31(4):607–17.
Tentri F, Blayney MJ, Albert JM, Gillespie BW, Kerr PG, Bommer J, et al. Mortality risk for dialysis patients with different levels of serum calcium, phosphorus, and PTH: the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis. 2008;52(3):519–30.
Young EW, Akiba T, Albert JM, McCarthy JT, Kerr PG, Mendelssohn DC, et al. Magnitude and impact of abnormal mineral metabolism in hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am J Kidney Dis. 2004;44 Suppl 2:34–8.
Sullivan C, Sayre SS, Leon JB, Machekano R, Love TE, Poter D, et al. Effect of food additives on hyperphosphatemia among patients with end-stage renal disease: a randomized controlled trial. JAMA. 2009;301(6):629–35.
Bergwitz C, Juppner H. Regulation of phosphate homeostasis by PTH, vitamin D, and FGF23. Ann Rev Med. 2010;61:91–104.
Quarles LD. Endocrine functions of bone in mineral metabolism regulation. J Clin Invest. 2008;118(12):3820–28.
Isakova T, Xie H, Yang W, Xie D, Anderson AH, Scialla J, Chronic Renal Insufficiency Cohort (CRIC) Study Group, et al. Fibroblast growth factor 23 and risks of mortality and end-stage renal disease in patients with chronic kidney disease. JAMA. 2011;305(23):2432–9.
Palmer SC, Hyen A, Macaskill P, Pellegrini F, Craig JC, Elder GJ, et al. Serum levels of phosphorus, parathyroid hormone, and calcium and risks of death and cardiovascular disease in individuals with chronic kidney disease: a systematic review and meta-analysis. JAMA. 2011;305(11):1119–27.
Kalantar-Zadeh K, Gutenurnst L, Mehrotra R, Kovesdy CP, Bross R, Shinaberger CS, et al. Understanding sources of dietary phosphorus in the treatment of patients with chronic kidney disease. Clin J Am Soc Nephrol. 2010;5(3):519–30.
Combe C, McCullough KP, Asano Y, Ginsberg N, Maroni BJ, Pifer TB. Kidney Disease Outcomes Quality Initiative (K/DOQI) and the Dialysis Outcomes and Practice Patterns Study (DOPPS): nutrition guidelines, indicators, and practices. Am J Kidney Dis. 2004;44((5) Suppl 2):39–46.
Cannata-Andia JB, Fernandez-Martin JL, Locatelli F, London G, Gorriz JL, et al. Use of phosphate-binding agents is associated with a lower risk of mortality. Kidney Int. 2013;84(5):998–1008.
Caldeira D, Amaral T, David C, Sampaio C. Educational strategies to reduce serum phosphorus in hyperphosphatemic patients with chronic kidney disease: systemic review with meta-analysis. J Ren Nutr. 2011;21(4):285–94.
Ashurst Ide B, Dobbie H. A randomized controlled trial of an educational intervention to improve phosphate levels in hemodialysis patients. J Ren Nutr. 2003;13(4):267–74.
Kovesdy CP, Kalantar-Zadeh K. Bone and mineral disorders in pre-dialysis CKD. Int Urol Nephrol. 2008;40(2):427–40.
Sherman RA, Mehta O. Phosphorus and potassium content of enhanced meat and poultry products: implications for patients who receive dialysis. Clin J Am Soc Nephrol. 2009;4(8):1370–3.
Calvo MS, Urbarri J. Contribution to total phosphorus intake: all sources considered. Semin Dial. 2013;26(1):54–61.
Japanese Society of Nephrology. Dietary recommendations for chronic kidney disease, 2014. Nihon Jinzo Gakkai Shi. 2014;56(5):553–99. Japanese.
Capisti A, Kalantar-Zedeh K. Management of natural and added dietary phosphorus burden in kidney disease. Semin Nephrol. 2013;33(2):180–90.
Gonzalez-Parra E, Gracia-Iguacel C, Egido J, Ortiz A. Phosphorus and nutrient in chronic kidney disease. Int J Nephrol. 2012. doi:10.1155/2012/597605.
Kalantar-Zadeh K. Patient education for phosphorus management in chronic kidney disease. Patient Prefer Adherence. 2013;7:379–90.
Schaafsma G. The protein digestibility-corrected amino acid score. J Nutr. 2000;130(7):1865S–7S.
Noori N, Kalantar-Zadeh K, Kovesdy CP, Bross R, Benner D, Kopple JD. Association of dietary phosphorus intake and phosphorus to protein ratio with mortality in hemodialysis patients. Clin J Am Soc Nephrol. 2010;5(4):883–92.
Ando S, Sakuma M, Morimoto Y, Arai H. The effect of various boiling conditions on reduction of phosphorus and protein in meat. J Ren Nutr. 2015;6:504–9.
Moe SM, Zidehsarai MP, Chambers MA, Jackman LA, Radcliff JS, Trevino LL, et al. Vegetarian compared with meat dietary protein source and phosphorus homeostasis in chronic kidney disease. Clin J Am Soc Nephrol. 2011;6:257–64.
Kanno Y, Inoue T, Matsumoto G, Tanaka T, Mogi K, Suzuki H. The control of serum phosphate by pre-washed rice (Musenmai) for hemodialysis patients (in Japanese). J Jpn Soc Cli Nutr. 2004;25:219–21.
Watanabe S, Kannno Y, et al. The efficacy of pre-washed rice (Musenmai) on diet therapy for hemodialysis patients (in Japanese). J Jpn Soc Dial Ther. 2006;39(6):1187–90.
Uehara Y, Yanagisawa K, Takeuchi S, Suwa A, Uchiyama K, Iashida H, et al. The effectiveness and usefulness of washing rice five times to reduce serum phosphorus and potassium in hemodialysis patients (in Japanese). J Jpn Soc Dial Ther. 2015;48(7):423–9.
Takemasa M, Asahara A, Sugemasa M. Amount of phosphorus contained in some sausage samples from supermarkets. Kawasaki Medical Welfare Journal. 2015;25(1):227–33.
Noori N, Sims JJ, Kopple JD, Shah A, Colman S, Shinaberger CS, et al. Organic and inorganic dietary phosphorus and its management in chronic kidney disease. Ira J Kidney Dis. 2010;4(2):89–100.
Ohnishi R, et al. Management of phosphorus for CKD—the prevalence of phosphorus containing food additives. Jpn J Clin Nutr. 2014;124(3):317–24.
Urbarri J. Phosphorus additives in food and their effect in dialysis. Clin J Am Soc Nephrol. 2009;4(8):1290–2.
Ramierez JA, Emmett M, White MG, Faith N, Santa ACA, Morawski SG, et al. The absorption of dietary phosphorus and calcium in hemodialysis patients. Kidney Int. 1986;30:753–9.
Hoover H. Compliance in patients on hemodialysis: a review of literature. J Am Diet Assoc. 1989;89:957–9.
Japanese Society of Dialysis therapy. Dietary guideline for dialysis patients in Japan. J Jpn Soc Dial Ther. 2014;47(5):287–291. Japanese.
Japanese society of Nephrology. Special issue: evidence-based practice guideline for the treatment of CKD. Nihon Jinzo Gakkai Shi. 2013;55(5):585–860. Japanese.
Standard Tables of Food Composition in Japan, 2010. . 2010.
Beanlands H, Horsburgh ME, Fox S, Howe A, Heather LC, et al. Caregiving by family and friends of adults receiving dialysis. Neph Nurs J. 2005;32(6):621–31.
Kent PS, McCarthy MP, Burrowes JD, McCann L, Goeddeke-Merickel CM, et al. Academy of Nutrition and Diabetes and National Kidney Foundation: revised 2014 standards of practice and standards of professional performance for registered dietitian nutritionist (competent, proficient, and expert) in nephrology nutrition. J Acad Nutr Diet. 2014;114(9):1448–57.
Reddy V, Symes F, Sethi N, Scally AJ, Scott J, Mumtaz R, Stoves J. Dietitian-led education program to improve phosphate control in a single center hemodialysis population. J Ren Nutr. 2009;19(4):314–20.
Choi A, Weekley CC, Chen SC, Li S, Tamura MK, Norris KC, et al. Association of educational attainment with chronic disease and mortality: the Kidney Early Evaluation Program (KEEP). Am J Kidney Dis. 2011;58(2):228–34.
Gutierrez OM, Anderson C, Isakova T, Scialla J, Negrea L, Anderson AH, et al. Low socioeconomic status associates with higher serum phosphate irrespective of race. J Am Soc Nephrol. 2010;21(11):1953–60.
Locatelli F, Fouque D, Hemiburger O, Drueke TB, Cannata-Andia JB, Horl WH. Nutritional status in dialysis patients: a European consensus. Nephrol Dial Transplant. 2002;17:563–72.
Green JA, Cavanaugh KL. Understanding the influence educational attainment on kidney health and opportunities for improved care. Adv Chronic Kidney Dis. 2015;22(1):24–30.
Pollock J, Jaffery JB. Knowledge of phosphorus compared with other nutrients in maintenance dialysis patients. J Ren Nutr. 2007;17(5):323–8.
Yokum D, Glass G, Cheung DF, Cunningham J, Fan S, Madden AM. Evaluation of a phosphate management protocol to achieve optimum serum phosphate levels in hemodialysis patients. J Ren Nutr. 2008;18(6):521–9.
Packard DP, Milton JE, Shunler LA, Short RA, Tuttle RR. Implications of chronic kidney disease for dietary treatment in cardiovascular disease. J Ren Nutr. 2006;16(3):259–68.
Gutekunst L. An update on phosphate binders: a dietitian’s perspective. J Ren Nutr. 2016;26(4):209–18.
Clements L, Ashurst I. Dietary strategy to halt the progression of chronic kidney disease. J of Renal Care. 2006;32:192–7.
Cl D, Holdsworth M, Atson V, Prsygodzka F. Knowledge of dietary restrictions and the medical consequence. J Am Diet Assoc. 2004;104:35–40.
Murphy-Gutekunst L. Hidden phosphorus in popular beverages. Nephrol Nurs J. 2005;32(4):443–5.
Sullivan CM, Leon JB, Sehgal AR. Phosphorus-containing food additives and the accuracy of nutrient databases: implications for renal patients. J Ren Nutr. 2007;17(5):350–4.
Russell MK. Functional assessment of nutrition status. Nutr Clin Pract. 2015;30(2):211–8.
Fouque D, Kalantar-Zadeh K, Kopple J, Cano N, Chauveau P, Cuppari L, et al. A proposed nomenclature and diagnostic criteria for protein-energy wasting in acute and chronic kidney disease. Kidney Int. 2008;73(4):391–8.
Obi Y, Qader H, Kovesdy CP, Kalantar-Zadeh K. Latest consensus and update on protein-energy wasting in chronic kidney disease. Curr Opin Clin Nutr Metab Care. 2015;18(3):254–62.
Carrero JJ, Stenvinkel P, Cappari S, Ikizler TA, Kalantar-Zadeh K, Kaysen G, et al. Etiology of the protein-energy wasting syndrome in chronic kidney disease: a consensus statement from the international society of renal nutrition and metabolism (ISRNN). J Ren Nutr. 2013;23(2):77–90.
Kovesdy CP. Malnutrition in dialysis patients—the need for intervention despite uncertain benefits. Semin Dial. 2015;20(1):28–34.
Kovesdy CP, Shinaberger CS, Kalantar-Zadeh K. Epidemiology of dietary nutrient intake in ESRD. Semin Dial. 2010;23(4):353–8.
Acknowledgements
We thank Prof. Kalantar-Zadeh for his kind advice and for providing his slides (which formed the basis of Fig. 1 and Table 1), Ms. Maureen and Dr. Steiber for their efforts as members of the American Academy of Nutrition and Dietetics to provide the NCP diagram (Fig. 3), all members of Team Kidney in Kyoto Katsura Hospital, and Dr. Marlini Muhamad (Physiology Department, NUI Galway, Ireland) for her advice on the English language used in this review.
Funding
None to declare
Availability of data and materials
Please contact the author for data request.
Authors’ contributions
KY and HM wrote this article. Both authors read and approved the final manuscript.
Authors’ information
Ms. Kawate is the head of the Div. of Nutrition, and Dr. Miyata is the director of the Dept. of Nephrology and Dialysis Unit in Kyoto Katsura Hospital.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
None required.
Ethics approval and consent to participate
Not applicable.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kawate, Y., Miyata, H. The importance of nutritional intervention by dietitians for hyperphosphatemia in maintained hemodialysis patients. Ren Replace Ther 3, 19 (2017). https://doi.org/10.1186/s41100-017-0095-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41100-017-0095-x