
Abstract
Background
Aneurysmal subarachnoid hemorrhage (aSAH) is an acute neurosurgical emergency with a significant fatality rate. In addition to acute brain injury, a considerable part of patients suffering from aSAH develops secondary brain damage such as cerebral vasospasm (CVS). CVS exacerbates the mortality. Therefore, it is urgently needed to find a biomarker, which could predict secondary brain and lead to operation by physicians more promptly. S100B, produced and released by astrocytes, has proven to be an important biomarker for brain injury.
Methods
In this present study, 51 patients with aSAH were included. Five CSF samples from each patient were obtained via lumbar puncture and were detected using electrochemiluminescence immunoassay (ECLIA).
Results
It indicated that S100B had a higher concentration in CSF of patients treated by surgical clipping after aSAH than that treated with endovascular coiling. In addition, the mean CSF S100B level in patients without CVS was much lower compared with patients with CVS. And, the expression of S100B increased along with the Fisher Grade at the same day after aSAH attacked and decreased as time went on. Moreover, the CSF S100B level of different time points and the mean CSF S100B level can predict the risk of CVS.
Conclusions
These data suggest that CSF S100B can be served as a predictor of CVS, which triggers an immediate management by clinicians to prevent secondary exacerbation.
Similar content being viewed by others


Background
Subarachnoidhemorrhage (SAH) accounts for about 6–8% of all strokes [1], among which the common cause is rupture of intracerebral aneurysm. The other causes are mainly vertebral artery dissection, arteriovenous malformation bleeding, or due to perimesencephalic SAH and some undefined causes [2]. The overall incidence rate of SAH is nearly 9 per 100,000 persons in one year, higher than that in the Scandinavian countries, which is the highest in Finland with 19.7 per 100,000 in one year [3]. Among those patients, there are more than 50% who are suffering from aneurysmal SAH (aSAH). However, less than 25% would reach proper medical attention [4].
The aSAH is an acute neurosurgical emergency with a significant fatality rate. How to manage ruptured intracranial aneurysms is a common challenge for neurosurgeons. More and more investigations focus on how to decrease its morbidity and mortality. In addition, one third of the patients with aSAH would develop secondary brain damage, including cerebral vasospasm (CVS) [5]. CVS exacerbates the mortality, and to find out a predictor of CVS in patients with severe SAH could reduce secondary brain damage [6].
S100B, a calcium-binding protein, is produced and released by astrocytes [7]. Increased S100B probably explains for either astrocytes’ reactions to brain injury or glial damage, as beneficial or detrimental physiological purposes [8, 9]. It is well known that S100B has previously been evaluated as a potential prognostic tool in acute ischemic stroke as well subarachnoid hemorrhage [10,11,12]. The level of S100B is found to be helpful to predict clinical outcome after SAH [13]. Therefore, S100B may serve as a marker to predict the secondary brain injury reliably and initiate therapeutic operation by physicians in a timelier way [14].
In the past few decades, the concentration of S100B is reported to be positively correlated with cerebral injury level after aSAH [15, 16]. Treatment modalities of aSAH is closely related to cerebral injury levels, but the difference of CSF S100B of patients with treatment modalities is not very clear. We tried to measure concentrations of CSF S100B of patients with different treatment modalities after aSAH and investigate that whether the S100B could serve as a potential predictor of CVS in patients after aSAH.
Methods
Patients
The experiment was approved by our local ethics committee (Ethics Committee of The 2nd Affiliated Hospital of HMU, China) and was conducted according to the principles of the Helsinki Declaration and Good Clinical Practice. Informed consent was obtained from each patient or patient’s next-of-kin.
Eligible patients between January 2010 and October 2013 were admitted. SAH was confirmed by CT. Only patients who were age 18 years or more and who suffered from a first aSAH were included. The following patients with exclusion criteria were excluded: primary central nervous disorders; died before the last lumbar puncture; external ventricular drainage (EVD) or ventricular peritoneal shunt more than 3 days of ictus; a decision not to perform clipping or coiling; a severe complication during the treatment such as intracranial infection, rebreeding, status epilepticus and massive brain infarction; pregnancy or nursing state; removal of part of brain as internal decompression.
Patients were enrolled into two groups according to the treatment modalities, ones treated with surgical clipping (n = 27) and the others treated with endovascular coiling (n = 24). At admission, Glasgow Coma Scale (GCS) score [17] and WFNS grading scale [18] were used to assess the clinical severity. Routinely, an electrocardiogram and troponin Ic assay (Stratus Analyzer by Dade, MAy, France) were obtained.
Keep Systolic arterial blood pressure from 140 to 160 mmHg. Seizures were routinely prevented by depakine 500 mg doses every 8 h for 30 days.
Confirmatory findings of CVS included arterial narrowing >50% detected on digital subtraction angiography (DSA) or computed tomographic angiography (CTA); anterior circulation peak mean velocity (PMV) > 160 cm/s, Lindegaard Ratio > 3, or PMV >90 cm/s for the basilar artery detected on daily transcranial Doppler (TCD) sonography. We proceeded to CTA immediately once SAH was established on a non-contrast CT scan. In addition, patients who were in relatively good condition would be asked to have DSA examination routinely. Delayed cerebral ischemia (DCI) caused by CVS was assessed by follow-up CT scans more than 24 h after treatment; determined as hypointensive changes reflecting partial or total involvement of the territory of a cerebral artery on CT scans and not attributable to an operative complication or spreading tissue ischemia.
Nimodipine administration (6 × 60 mg) was started once the patients were admitted into the ICU and was routinely used after operation. But oral nimodipine was discontinued during episodes of profound arterial hypotension requiring high-dose catecholamine support. Those patients, who weighed more than 70 kg, were demanded to take the medicine twice a day, and once per day for those who weighed less than 70 kg.
Samples
A total of five CSF samples from each patient were obtained. Day 1 was defined from the day of burst. The Baseline sample (first CSF sample) was obtained between day 2 and 4. It depends on when the patient had received treatments and had received an EVD. The CSF sample was collected 6 h after removal of the head drainage tube. On day 6, 8, 10 and 12 after ictus, the each sample was obtained. Prior to sampling, 2 ml of CSF was discarded, because of a dilution effect or precaution to contamination. About 7 ml of each sample was harvested into a 15 ml centrifuge tube, placed in ice immediately, and centrifuged at RCF. 2000 for 20 min at 4 °C. The supernatant was immediately used for assays or stored at −80 °C. Electrochemiluminescence immunoassay (ECLIA) was used to analyse the samples. The equipment used was Elecsys 2010, Roche Diagnostics (Mannheim, Germany) and Modular Analytics E170. The detection range was from 0.005 to 39 μg/L. Samples were analyzed in duplicates.
Statistical analysis
Statistics were performed using Microsoft Excel 2013 or the SPSS Graduate Pack, version 11.0, statistical software (SPSS). S100B levels between patients with and without CVS and the two operating methods were compared by Student t-test. Fisher Exact Test, Standard Deviation (SD), Student’s t test were used for the analysis of the data in Table 1. Descriptive statistics, including 2-way analysis of variance, mean and SD were used to determine statistically significant differences. P < 0.05 was considered to be statistically significant.
Results
A total of 51 patients with aneurysm, treated with endovascular coiling (24 patients) or surgical clipping (27 patients) within 48 h of aSAH ictus, were included. Their mean age was 57 years (from 31 to 87 years). There were 24 females and 27 males. The mean score of the WFNS grading scale was 3.5, while the mean GCS score on admission was 7, and the mean Fisher grade was 3.6.
Treatment methods depended on the expertise of the admitting neurosurgeon, aneurysm location and morphology. After the first lumbar puncture on day 2–4, CSF samples were obtained once every other day at the 6th, 8th, 10th and 12th day respectively following ictus. The S100B in CSF was measured by ECLIA. We compared the S100B in the two groups of patients under the same disease severity and these data indicated that the expression of S100B increased significantly along with the Fisher grading of patients at the same day after aSAH attacked, despite of treating modalities or whether having vasospasm or not (Fig. 1a). However, as time goes on, it decreased obviously and significantly in Grade 1 and 2 (Fig. 1b). Although the concentration of S100B reduced over time in Grade 3, 4 and 5, it was not statistically significantly (Fig. 1b).

The expression of CSF S100B increased along with the Fisher grading of patients and decreased as time went on. The S100B in CSF was measured by ECLIA assay at day 2-4, 6, 8, 10, and 12 after aSAH attacked. a It indicated that the S100B level increased along with the Fisher grading at the same day after rupture. *P < 0.05, **P < 0.01, and ***P < 0.001, compared to the Grade 1. b The CSF S100B decreased in a time-dependent manner significantly in Grade 1 and 2, but not significantly in Grade 3, 4 and 5. ##P < 0.01, ###P < 0.001, ***P < 0.001, compared to the Baseline sample. c The CSF S100B levels in patients treated with surgical clipping or endovascular coiling at each day. There are no statistical differences between the two operating methods. CSF, cerebrospinal fluid. aSAH, aneurysmal subarachnoid hemorrhage
Although there was a tendency that the amount of S100B of patients treated with surgical clipping was somehow higher than that treated with endovascular coiling at each day, it was not statistically significant (Fig. 1c).
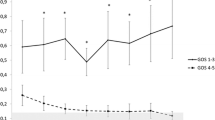
Compare to patients who developed CVS, there come out no differences significantly in gender, age, GCS score, Fisher grade or WFNS grade, even the treatment modalities (Table 1). However, CSF S100B level in patients who developed CVS was much higher than those who did not at each day (Table 1). In addition, we analyzed the variation of CSF S100B between patients with and without CVS in surgical clipping group (Fig. 2a) or the endovascular coiling group (Fig. 2b). And the analysis showed consistent tendency. Moreover, the CSF S100B level of different time points (day 2–4, day 6, day 8, day10 and day 12) and the mean CSF S100B level can predict the risk of CVS using univariate analysis. The receiver-operating characteristic (ROC) curves was obtained for the S100B level of different time points and the risk of CVS (Fig. 2c). For example, area under the ROC curve of day 2–4 CSF S100B level was 0.767. By multivariate analysis, the CSF S100B level of different time points as well as the mean CSF S100B level could not predict the risk of CVS (Additional file 1: Table S1). These data suggest that CSF S100B can be a predictor of CVS, but cannot predict the risk of CVS independently.

The CSF S100B level in patients with and without CVS. The CSF S100B in patients with CVS was higher than that without CVS in surgical clipping group (a), or the endovascular coiling group (b). c The area under the receiver-operating characteristic curve of Day 2-4 was 0.767, and 0.802, 0.791, 0.775, 0.797, 0.801 on Day 6, 8, 10, 12 or mean value, respectively. *P < 0.05, **P < 0.01. CSF, cerebrospinal fluid. CVS, cerebral vasospasm
Discussion
There are two treatment modalities of aSAH to completely, immediately, permanently, and safely occlude the dome of aneurysm and preserve the parent artery. The debates and researches of their merits and faults have been always existing since the advent of two ways. It has been reported by both the Barrow Ruptured Aneurysm Trial (BRAT) [19] and the International Subarachnoid Aneurysm Trial (ISAT) [20, 21] that there come out better early clinical condition by endovascular coiling after aneurysms rupture than that by clipping. Recently, a meta-analysis also draw the same conclusion [22]. In addition, some investigations show that surgical clipping is more prone to hydrocephalus [23], cerebral vasospasm [22, 24] and epilepsy [21]. In this study, there was a difference of mean CSF S100B between high grade and low grade, which demonstrated that the brain injury degree of high grade was significantly higher than that of low grade. Although the mean CSF S100B in patients who received endovascular coiling seemed to be lower compared with that of patients who received surgical clipping, it was not statistically significant.
Within the study period, the concentration of mean CSF S100B decreased tardily over time after rupture and be higher in the high grade group than that in the low grade group, which is consistent with some previous studies [15, 25, 26]. Brain damage, which causes high S100B level, may be highly related to the CVS. Post-traumatic vasospasm usually develops within 3 days of brain injury, while aneurysmal CVS may develop in 4 days after the hemorrhage [27].
CVS exacerbates the mortality. It may be a major target of intervention after the surgery of aSAH. To find out a specific biomarker for predicting CVS is very important, since earlier identification and therefore earlier treatment of CVS would decrease the mortality and morbidity of patients. In our study, we found that the mean CSF S100B or S100B level at different time points in patients without CVS were much lower than that in patients with CVS, which suggested the potential role of S100B as an important prognostic factor of C VS.
In this study, 7 of 27 patients in clipping group had decompressive craniectomy. And it indicated that patients with decompressive craniectomy came out a higher CSF S100B level at every time points, compared to patients without (Additional file 2: Table S2). Generally, patients with poor grade tend to need decompressive craniectomy, which may be the reasonable explanation for the higher S100B.
In addition, we adopted strict selection criteria, some interference factors such as intracranial infection, rebreeding or removal of part of brain as internal decompression were excluded. While the above factors increase the accuracy of this investigation, there are also several limitations in this study. Fewer cases were included in this study. However we can conclude that, CSF S100B can be used as a predicttor of CVS. And combination with other biochemical markers such as glial fibrillary acidic protein (GFAP), neuron-specific enolase (NSE) and malondialdehyde (MDA) [16] might be of greater utility.
Conclusion
S100B in CSF increased along with the Fisher grading of patients and decreased as time went on after aSAH attacked (Grade 1–2), despite treating modalities or whether having vasospasm or not. Mean CSF S100B level in patients without CVS was much lower than that in patients with CVS. The CSF S100B level of different time points and the mean CSF S100B level can predict the risk of CVS using univariate analysis.
These data suggest that CSF S100B can be served as a predictor of CVS, but cannot predict the risk of CVS independently.
Abbreviations
- aSAH:
-
Aneurysmal subarachnoid hemorrhage
- CT:
-
Computed tomography
- CNS:
-
Central nervous system
- CSF:
-
Cerebrospinal fluid
- CTA:
-
Computed tomographic angiography
- CVS:
-
Cerebral vasospasm
- DCI:
-
Delayed cerebral ischemia
- DSA:
-
Digital subtraction angiography
- EVD:
-
External ventricular drainage
- ECLIA:
-
Electrochemiluminescence immunoassay
- GFAP:
-
Glial fibrillary acidic protein
- GCS:
-
Glasgow coma scale score
- MDA:
-
Malondialdehyde
- NSE:
-
Neuron-specific enolase
- PMV:
-
Anterior circulation peak mean velocity
- SD:
-
Standard deviation
- SPSS:
-
Statistical software
- TCD:
-
Transcranial doppler sonography
References
Jose Biller M, John C. Godersky Harold P. Adams Jr. Management of Aneurysmal Subarachnoid Hemorrhage. Stroke. 1988;19:1300–05.
van Gijn J, Rinkel GJ. Subarachnoid haemorrhage: diagnosis, causes and management. Brain. 2001;124:249–78.
de Rooij NK, Linn FH, van der Plas JA, Algra A, Rinkel GJ. Incidence of subarachnoid haemorrhage: a systematic review with emphasis on region, age, gender and time trends. J Neurol Neurosurg Psychiatry. 2007;78:1365–72.
Diringer MN. Management of aneurysmal subarachnoid hemorrhage. Crit Care Med. 2009;37:432–40.
Roger VL, Go AS, Lloyd-Jones DM, Adams RJ, Berry JD, Brown TM, Carnethon MR, Dai S, de Simone G, Ford ES, et al. Heart disease and stroke statistics--2011 update: a report from the American Heart Association. Circulation. 2011;123:e18–e209.
Zhou Y, Martin RD, Zhang JH. Advances in experimental subarachnoid hemorrhage. Acta Neurochir Suppl. 2011;110:15–21.
Donato R, Sorci G, Riuzzi F, Arcuri C, Bianchi R, Brozzi F, Tubaro C, Giambanco I. S100B’s double life: intracellular regulator and extracellular signal. Biochim Biophys Acta. 2009;1793:1008–22.
Herrmann M, Ehrenreich H. Brain derived proteins as markers of acute stroke: their relation to pathophysiology, outcome prediction and neuroprotective drug monitoring. Restor Neurol Neurosci. 2003;21:177–90.
Kleindienst A, Hesse F, Bullock MR, Buchfelder M. The neurotrophic protein S100B: value as a marker of brain damage and possible therapeutic implications. Prog Brain Res. 2007;161:317–25.
Stranjalis G, Korfias S, Psachoulia C, Kouyialis A, Sakas DE, Mendelow AD. The prognostic value of serum S-100B protein in spontaneous subarachnoid haemorrhage. Acta Neurochir. 2007;149:231–7. discussion 237-238
Foerch C, Wunderlich MT, Dvorak F, Humpich M, Kahles T, Goertler M, Alvarez-Sabin J, Wallesch CW, Molina CA, Steinmetz H, et al. Elevated serum S100B levels indicate a higher risk of hemorrhagic transformation after thrombolytic therapy in acute stroke. Stroke. 2007;38:2491–5.
Whiteley W, Tseng MC, Sandercock P. Blood biomarkers in the diagnosis of ischemic stroke: a systematic review. Stroke. 2008;39:2902–9.
Zaidat OO, Ionita CC, Hussain SI, Alexander MJ, Friedman AH, Graffagnino C. Impact of ruptured cerebral aneurysm coiling and clipping on the incidence of cerebral vasospasm and clinical outcome. J Neuroimaging. 2009;19:144–9.
Taha MM, Nakahara I, Higashi T, Iwamuro Y, Iwaasa M, Watanabe Y, Tsunetoshi K, Munemitsu T. Endovascular embolization vs surgical clipping in treatment of cerebral aneurysms: morbidity and mortality with short-term outcome. Surg Neurol. 2006;66:277–84. discussion 284
Moritz S, Warnat J, Bele S, Graf BM, Woertgen C. The prognostic value of NSE and S100B from serum and cerebrospinal fluid in patients with spontaneous subarachnoid hemorrhage. J Neurosurg Anesthesiol. 2010;22:21–31.
Kaneda K, Fujita M, Yamashita S, Kaneko T, Kawamura Y, Izumi T, Tsuruta R, Kasaoka S, Maekawa T. Prognostic value of biochemical markers of brain damage and oxidative stress in post-surgical aneurysmal subarachnoid hemorrhage patients. Brain Res Bull. 2010;81:173–7.
Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2:81–4.
Teasdale GM, Drake CG, Hunt W, Kassell N, Sano K, Pertuiset B, De Villiers JC. A universal subarachnoid hemorrhage scale: report of a committee of the world federation of neurosurgical societies. J Neurol Neurosurg Psychiatry. 1988;51:1457.
McDougall CG, Spetzler RF, Zabramski JM, Partovi S, Hills NK, Nakaji P, Albuquerque FC. The barrow ruptured aneurysm trial. J Neurosurg. 2012;116:135–44.
Molyneux A, Kerr R, Stratton I, Sandercock P, Clarke M, Shrimpton J, Holman R, International Subarachnoid Aneurysm Trial Collaborative G. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet. 2002;360:1267–74.
Molyneux AJ, Kerr RS, Yu LM, Clarke M, Sneade M, Yarnold JA, Sandercock P, International Subarachnoid Aneurysm Trial Collaborative G. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet. 2005;366:809–17.
Li H, Pan R, Wang H, Rong X, Yin Z, Milgrom DP, Shi X, Tang Y, Peng Y. Clipping versus coiling for ruptured intracranial aneurysms: a systematic review and meta-analysis. Stroke. 2013;44:29–37.
Koh KM, Ng Z, Low SY, Chua HZ, Chou N, Low SW, Yeo TT. Management of ruptured intracranial aneurysms in the post-ISAT era: outcome of surgical clipping versus endovascular coiling in a Singapore tertiary institution. Singap Med J. 2013;54:332–8.
Dumont AS, Crowley RW, Monteith SJ, Ilodigwe D, Kassell NF, Mayer S, Ruefenacht D, Weidauer S, Pasqualin A, Macdonald RL. Endovascular treatment or neurosurgical clipping of ruptured intracranial aneurysms: effect on angiographic vasospasm, delayed ischemic neurological deficit, cerebral infarction, and clinical outcome. Stroke. 2010;41:2519–24.
Amiri M, Astrand R, Romner B. Can S100B predict cerebral vasospasms in patients suffering from subarachnoid Hemorrhage? Front Neurol. 2013;4:65.
Jung CS, Lange B, Zimmermann M, Seifert V. CSF and serum biomarkers focusing on cerebral vasospasm and ischemia after subarachnoid Hemorrhage. Stroke Res Treat. 2013;2013:560305.
Zubkov AY, Lewis AI, Raila FA, Zhang J, Parent AD. Risk factors for the development of post-traumatic cerebral vasospasm. Surg Neurol. 2000;53:126–30.
Acknowledgements
We are grateful to the sample donors for the study.
Funding
The work was supported by Heilongjiang Province Education Department Foundation (12531395); the Health Agency Project (2011-099).
Availability of data and materials
Data are stored in corresponding author of this paper and are available upon request.
Author information
Authors and Affiliations
Contributions
RYL designed the study and drafted the manuscript with JLL, JQC. YLL participated in doing the endovascular coiling. QBL and XYL did the statistical analysis. YF revised the manuscript. QHY, MHC,MLL and ZFH collected CSF samples of patients. CLJ performed surgical clipping and designed the research. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by our local ethics committee (Ethics Committee of the 2nd Affiliated Hospital o f Harbin Medical University, Harbin, China) and was conducted in compliance with the Declaration of Helsinki. The experimental protocol was approved by the Clinical Research Ethics Committee of the 2nd Affiliated Hospital of Harbin Medical University (2013-R-024).
Consent for publication
Patients agreed upon CSF collection in the 2nd affiliated hospital of HMU (a teaching hospital), their information can be used for scientific purposes.
Competing interests
The authors declare that there are no competing interests.
Additional files
Additional file 1: Table S1.
Multivariate analysis for the prediction of CVS. (DOCX 21 kb)
Additional file 2: Table S2.
CSF S100B levels (μg/L) in patients with decompressive craniectomy compared to patients without. (DOCX 19 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Li, R., Li, J., Li, Q. et al. CSF S100B in patients treated by endovascular coiling or surgical clipping after aneurysmal subarachnoid hemorrhage and its correlation to cerebral vasospasm. Chin Neurosurg Jl 3, 24 (2017). https://doi.org/10.1186/s41016-017-0089-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41016-017-0089-0