
Abstract
Background
Cowden syndrome is characterized by multiple hamartomas in various tissues, including the skin, brain, breast, thyroid, mucous membrane, and gastrointestinal tract, and is reported to increase the risk of malignant disease.
Case presentation
We describe the case of a 52-year-old woman in whom a tumor was diagnosed in the left cerebellar hemisphere and treated by surgical resection. Phosphatase and tensin homolog (PTEN) mutation in exon 8 insertion was found in the brain tumor tissue and leukocytes. This finding supported the diagnosis of Cowden syndrome. She consequently developed endometrial cancer and underwent abdominal total hysterectomy with bilateral salpingo-oophorectomy. Four years later, hormone receptor-positive breast cancer was found in the right breast, and breast-conserving surgery with radiation therapy and sentinel lymph node biopsy was performed.
Conclusions
Herein, we describe a patient who was diagnosed as having familial breast cancer associated with PTEN mutation-related Cowden syndrome. We also reviewed reports of this syndrome in the literature for disease appraisal.
Similar content being viewed by others

Background
Estimates show that up to 15% of breast cancer patients have one or more first-degree relatives with breast cancer [1]. Inherited breast cancer is caused by penetrant susceptibility genes and most often involves germ line mutations of the BRCA1 and BRCA2 genes in about 15% of familial breast cancer patients. Tumor protein 53 (TP53), cadherin 1 (CDH1), liver kinase B1 (LKB1), and phosphatase and tensin homolog (PTEN) are rarely associated with the development of breast cancer, which occurs in only about 3% of patients with familial breast cancer. Breast cancer in approximately half of women with a familial history may also result from unexplained genes [2].
Cowden syndrome (CS) is an autosomal dominant inherited cancer syndrome associated with germ line mutations in PTEN, a tumor suppressor gene. CS is characterized by multiple hamartomas and developing breast, thyroid, and endometrial malignancies. Dysplastic cerebellar gangliocytoma called Lhermitte-Duclos disease (LDD) is also associated with CS [3, 4]. The cumulative lifetime risks of any cancer diagnosis is 89% for CS patients, and the morbidities are 85% in breast cancer, 32% in LDD, 21% in thyroid cancer, 19% in endometrial cancer, 15% in renal cancer, 16% in colon and rectum cancers, and 15% in kidney cancer [4, 5]. Herein, we report a case of PTEN-mutated hereditary breast cancer with LDD.
Case presentation
The patient was a 52-year-old woman with a prior history of chronic thyroiditis. Her sister was diagnosed as having congenital hydrocephalus and her mother as having heart valve disease. Her father died of myocardial infarction. The patient had a fall and sustained a head injury. Brain T2-weighted magnetic resonance imaging (MRI) revealed alternating isointense and hyperintense bands in the left cerebellar hemisphere (Fig. 1a). Surgical resection of the tumor in the cerebellar hemisphere was performed, and the histopathological diagnosis was dysplastic gangliocytoma. The patient was subsequently referred for genetic counseling. Genetic testing of her leukocytes and resected tumor revealed mutation in the exon 8 insertion of the PTEN gene (Fig. 2), leading to a diagnosis of CS associated with LDD.

MRI and CT at the age of 50 years. a MRI showed alternating isointense and hyperintense bands in the left cerebellar hemisphere (arrow). b Whole-body CT screening detected an adenomatous goiter (arrow). c CT also demonstrated uterine cancer (arrow)

Analysis of PTEN gene mutations. Genomic DNAs for germ line mutation analyses were obtained from the buffy coat and resected tumor. Polymerase chain reaction products were sequenced directly using an automated DNA-sequencing system (Model 3130; Applied Biosystems, Foster City, CA). PTEN sequencing demonstrated that a germ line mutation c. 288 insertion A was found in exon 8, which caused a frameshift mutation (p.V290fs*8). A reverse primer was used in this analysis
After genetic diagnosis, computed tomography (CT) whole-body screening revealed an adenomatous goiter (Fig. 1b) and uterine cancer (Fig. 1c). Thus, abdominal total hysterectomy with bilateral salpingo-oophorectomy was performed. The histopathological finding was endometrioid adenocarcinoma with no lymph node metastasis. At the age of 55 years, the follow-up CT for uterine cancer incidentally revealed a tumor in the right breast. Mammography (MMG) showed a smooth mass in the left breast (Fig. 3a). An irregular indistinct mass (12 × 11 × 10 mm) was detected in the right breast by ultrasonography (US) (Fig. 3b). However, she did not visit our hospital for the required additional examination. Two years later, a breast mass was detected in the breast cancer screening. A spiculated mass was observed in the right breast on MMG (Fig. 4a), and the tumor increased in size (20 × 20 × 11 mm) as shown by US (Fig. 4b). Core needle biopsy revealed invasive ductal carcinoma: estrogen and progesterone receptor-positive, Her2 2+, and Ki-67 20%. The patient underwent breast-conserving surgery and sentinel lymph node biopsy. Histopathological examination confirmed an invasive micropapillary carcinoma measuring 2.5 × 2.1 × 1.3 cm.

MMG and US examinations at the age of 55 years. a A smooth mass was detected in the left breast by MMG. b An irregular indistinct mass (12 × 11 × 10 mm) was found in the right breast by US

MMG and US at the age of 57 years. a A spiculated mass was observed in the right breast. b The size of the irregular indistinct tumor in the right breast increased (20 × 20 × 11 mm) as shown by US
Immunohistochemistry revealed estrogen receptor-positive and progesterone receptor-positive staining, Her2 2+, and Ki-67-positive staining of 10% (Fig. 5). The lymph nodes were not involved. She was given 50 Gy radiation and hormone therapy as adjuvant therapy. Any sign of recurrent disease has not been found in the 3 years since the last surgery for her breast cancer.

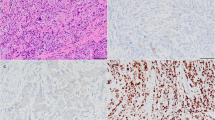
Histopathological features of the tumor in this case. a Invasive micropapillary carcinoma (H&E staining, ×200). b Immunohistochemistry showed Her2 receptor 2+ (×200). c Estrogen receptor-positive staining of 100% (×200). d Progesterone receptor-positive staining of 100% (×200)
Discussion
Previous studies have shown that approximately 20 to 34% of patients with CS carry germ line mutations of PTEN, a gene located on chromosome 10q23 [6,7,8]. These include 19–29% missense mutations, 19–33% nonsense mutations, 20% insertions, 2–14% small deletions, 10–11% splice site mutations, 1–29% frameshift mutations, 3% large deletions, and 3% promoter mutations [6, 7, 9]. In the present case, adenine was inserted in the codon of exon 8, resulting in the rearrangement of the amino acid sequence from valine to serine (Fig. 2). There were 27 reported cases of CS with deleterious mutation in Japan from 1984 to 2017 (May) according to Igaku Chuo Zasshi which is updated by the Japan Medical Abstracts Society.
PTEN participates in regulating the phosphoinositide 3 kinase (PI3K)-AKT and mTOR signaling pathways for negative regulation, controls cell proliferation and cell cycle progression, and promotes apoptosis. Thus, a loss of PTEN function correlates with the development of various human cancers [10]. It has been reported that PTEN is a gene in which mutation is most frequently found in primary breast cancers [11]. It remains controversial how the abnormality of this gene function may affect the prognosis of breast cancer patients. Previous reports of cases with CS revealed that most breast cancers were hormone receptor-positive including the present case (Table 1) [12,13,14,15,16,17,18,19,20,21,22,23,24,25]. Based on the history of the present case representing a slow-growing tumor, the clinical course of this case may be favorable. CS has a high risk of transforming into malignant tumors; thus, cancer surveillance is an important management for other organs [26]. The National Comprehensive Cancer Network (NCCN) recommendation is to undergo thyroid ultrasound, colonoscopy, renal ultrasound, annual dermatologic examination, and annual endometrial biopsies. After genetic diagnosis, we performed screening for breast, thyroid, and endometrial malignancies. Endometrial adenocarcinoma was found. Usually, the recommended treatment for hereditary breast cancer associated with BRCA1 mutation is mastectomy because it is a more aggressive cancer with a poor prognosis. However, as PTEN-related breast cancer tends to grow slowly, patients are not always required to undergo mastectomy. We therefore performed breast-conserving surgery in the present case.
The American Cancer Society and NCCN guidelines recommend MRI in addition to MMG for high-risk patients including those with PTEN hamartoma tumor syndrome [27, 28]. It may be necessary to apply screening of breast MRI to patients with a high risk for high-grade hereditary breast cancers such as BRCA1 mutation carriers. However, screening breast MRI may not be practical to apply to all hereditary breast cancer cases because of its relatively low specificity and the high cost of enhanced breast MRI. It is also difficult to perform pathological examination if the lesion is detected only by MRI.
However, the usual screening management for breast cancer may be insufficient for patients with CS, because the mean age at diagnosis of breast cancer is reported to be about 40 years old in women with CS [29], which is younger than in the usual population. Thus, it is necessary to consider starting MMG screening at an earlier age and performing it more frequently such as once a year. Ultrasound could be another option, which may be useful for younger women and women with dense breasts [30].
Conclusions
In conclusion, we report the case of a rare familial breast cancer syndrome of CS. Unlike other familial breast cancers such as those with BRCA1 mutation, breast cancers with CS are generally hormone receptor-positive and may have a favorable clinical course.
Abbreviations
- CS:
-
Cowden syndrome
- CT:
-
Computed tomography
- LDD:
-
Lhermitte-Duclos disease
- MMG:
-
Mammography
- MRI:
-
Magnetic resonance imaging
- PTEN:
-
Phosphatase and tensin homolog
- US:
-
Ultrasonography
References
Collaborative Group on Hormonal Factors in Breast Cancer. Familial breast cancer: collaborative reanalysis of individual data from 52 epidemiological studies including 58,209 women with breast cancer and 101,986 women without the disease. Lancet. 2001;358(9291):1389–99.
Couch FJ, Nathanson KL, Offit K. Two decades after BRCA: setting paradigms in personalized cancer care and prevention. Science. 2014;343(6178):1466–70.
Zhou XP, Marsh DJ, Morrison CD, Chaudhury AR, Maxwell M, Reifenberger G, et al. Germline inactivation of PTEN and dysregulation of the phosphoinositol-3-kinase/Akt pathway cause human Lhermitte-Duclos disease in adults. Am J Hum Genet. 2003;73(5):1191–8.
Riegert-Johnson DL, Gleeson FC, Roberts M, Tholen K, Youngborg L, Bullock M, et al. Cancer and Lhermitte-Duclos disease are common in Cowden syndrome patients. Hered Cancer Clin Pract. 2010;8(1):6.
Tan MH, Mester JL, Ngeow J, Rybicki LA, Orloff MS, Eng C. Lifetime cancer risks in individuals with germline PTEN mutations. Clin Cancer Res. 2012;18(2):400–7.
Pilarski R, Stephens JA, Noss R, Fisher JL, Prior TW. Predicting PTEN mutations: an evaluation of Cowden syndrome and Bannayan-Riley-Ruvalcaba syndrome clinical features. J Med Genet. 2011;48(8):505–12.
Tan MH, Mester J, Peterson C, Yang Y, Chen JL, Rybicki LA, et al. A clinical scoring system for selection of patients for PTEN mutation testing is proposed on the basis of a prospective study of 3042 probands. Am J Hum Genet. 2011;88(1):42–56.
Nelen MR, Padberg GW, Peeters EA, Lin AY, van den Helm B, Frants RR, et al. Localization of the gene for Cowden disease to chromosome 10q22-23. Nat Genet. 1996;13(1):114–6.
Marsh DJ, Coulon V, Lunetta KL, Rocca-Serra P, Dahia PL, Zheng Z, et al. Mutation spectrum and genotype-phenotype analyses in Cowden disease and Bannayan-Zonana syndrome, two hamartoma syndromes with germline PTEN mutation. Hum Mol Genet. 1998;7(3):507–15.
Stambolic V, Suzuki A, de la Pompa JL, Brothers GM, Mirtsos C, Sasaki T, et al. Negative regulation of PKB/Akt-dependent cell survival by the tumor suppressor PTEN. Cell. 1998;95(1):29–39.
Cancer Genome Atlas Network. Comprehensive molecular portraits of human breast tumours. Nature. 2012;490(7418):61–70.
Kanayama Y, Noshima S, Samura M, Okazaki M, Zenpo N, Kamei T, et al. A case of Cowden disease with multiple primary cancer. J Jpn Surg Assoc. 2011;72(12):3026–9.
Morse CB, Garcia RL, Calhoun KE, Swisher EM. Premalignant alterations in breast and endometrium associated with a PTEN mutation in a woman with Cowden syndrome: implications for preventive care. Gynecol Oncol Rep. 2015;9(12):13–6.
Kalin A, Merideth MA, Regier DS, Blumenthal GM, Dennis PA, Stratton P. Management of reproductive health in Cowden syndrome complicated by endometrial polyps and breast cancer. Obstet Gynecol. 2013;121(2 Pt 2 Suppl 1):461–4.
Peiró G, Adrover E, Guijarro J, Ballester I, Jimenez MJ, Planelles M, et al. Synchronous bilateral breast carcinoma in a patient with Cowden syndrome: a case report with morphologic, immunohistochemical and genetic analysis. Breast J. 2010;16(1):77–81.
Erickson J, Lyon DE. Breast cancer in Cowden syndrome. Manifestation of a familial cancer syndrome. Clin J Oncol Nurs. 2010;14(1):33–5.
Winter H, McEwen A. Cowden syndrome presenting as advanced breast cancer in a young woman with macrocephaly. Intern Med J. 2012;42(10):1160–1.
Seo M, Cho N, Ahn HS, Moon HG. Cowden syndrome presenting as breast cancer: imaging and clinical features. Korean J Radiol. 2014;15(5):586–90.
Sabaté JM, Gómez A, Torrubia S, Blancas C, Sánchez G, Alonso MC, et al. Evaluation of breast involvement in relation to Cowden syndrome: a radiological and clinicopathological study of patients with PTEN germ-line mutations. Eur Radiol. 2006;16(3):702–6.
Ball S, Arolker M, Purushotham AD. Breast cancer, Cowden disease and PTEN-MATCHS syndrome. Eur J Surg Oncol. 2001;27(6):604–6.
Walsh S, Carter M, Tubridy N, McDermott EW. Lhermitte-Duclos and Cowden diseases: breast cancer as an unusual initial presentation of these overlapping conditions. BMJ Case Rep. 2011;20:bcr0820114730.
Fackenthal JD, Marsh DJ, Richardson AL, Cummings SA, Eng C, Robinson BG, et al. Male breast cancer in Cowden syndrome patients with germline PTEN mutations. J Med Genet. 2001;38(3):159–64.
Baù MG, Arisio R, Cristini G, Bertone E, Campogrande M. Screening-detected breast carcinoma in a patient with Cowden syndrome. Breast. 2004;13(3):239–41.
Nakamura T, Sako H, Harada S, Watanabe N, Okugawa K, Nakano K, et al. A case of Cowden syndrome. J Kyoto Pref Univ Med. 2012;121(4):223–9.
Kikuchi S, Uchino M, Noguchi S, Yamashita H, Kawaguchi H. A case of Cowden disease with thyroid mass, parathyroid adenoma and breast cancer. Folia Endocrinol Japonica. 2014;90(2):523 (in Japanese).
Daly MB, Axilbund JE, Buys S, Crawford B, Farrell CD, Friedman S, et al. Genetic/familial high-risk assessment: breast and ovarian. J Natl Compr Canc Netw. 2010;8(5):562–94.
Bevers TB, Anderson BO, Bonaccio E, Buys S, Daly MB, Dempsey PJ, et al.; National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: breast cancer screening and diagnosis. J Natl Compr Canc Netw. 2009; 7(10): 1060-96.
Saslow D, Boetes C, Burke W, Harms S, Leach MO, Lehman CD, et al.; American Cancer Society Breast Cancer Advisory Group. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007; 57(2): 75-89.
Pilarski R. Cowden syndrome: a critical review of the clinical literature. J Genet Couns. 2009;18(1):13–27.
Ohuchi N, Suzuki A, Sobue T, Kawai M, Yamamoto S, Zheng YF, et al.; J-START investigator groups. Sensitivity and specificity of mammography and adjunctive ultrasonography to screen for breast cancer in the Japan Strategic Anti-cancer Randomized Trial (J-START): a randomised controlled trial. Lancet. 2015; S0140-6736 (15): 00774-6.
Acknowledgements
We thank Dr. Edward Barroga (http://orcid.org/0000-0002-8920-2607), Associate Professor and Senior Editor from the Department of International Medical Communications of Tokyo Medical University, for reviewing and editing the manuscript.
Funding
None.
Author information
Authors and Affiliations
Contributions
Authors’ contributions
FK and TI wrote the manuscript. AU, JA, and TI performed the operation. ES diagnosed the disease pathologically. HK, KY, MH, YK, ST, MO, and TI contributed to the design and drafting of the manuscript. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Consent for publication
Informed consent was obtained from the patient for the publication of this case report.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Kimura, F., Ueda, A., Sato, E. et al. Hereditary breast cancer associated with Cowden syndrome-related PTEN mutation with Lhermitte-Duclos disease. surg case rep 3, 83 (2017). https://doi.org/10.1186/s40792-017-0355-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40792-017-0355-6