
Abstract
Intramedullary astrocytomas (IMAs) are rare tumors, and few studies specific to the molecular alterations of IMAs have been performed. Recently, KIAA1549-BRAF fusions and the H3F3A p.K27M mutation have been described in low-grade (LG) and high-grade (HG) IMAs, respectively. In the present study, we collected clinico-radiological data and performed targeted next-generation sequencing for 61 IMAs (26 grade I pilocytic, 17 grade II diffuse, 3 LG, 3 grade III and 12 grade IV) to identify KIAA1549-BRAF fusions and mutations in 33 genes commonly implicated in gliomas and the 1p/19q regions. One hundred seventeen brain astrocytomas were analyzed for comparison. While we did not observe a difference in clinico-radiological features between LG and HG IMAs, we observed significantly different overall survival (OS) and event-free survival (EFS). Multivariate analysis showed that the tumor grade was associated with better OS while EFS was strongly impacted by tumor grade and surgery, with higher rates of disease progression in cases in which only biopsy could be performed. For LG IMAs, EFS was only impacted by surgery and not by grade. The most common mutations found in IMAs involved TP53, H3F3A p.K27M and ATRX. As in the brain, grade I pilocytic IMAs frequently harbored KIAA1549-BRAF fusions but with different fusion types. Non-canonical IDH mutations were observed in only 2 grade II diffuse IMAs. No EGFR or TERT promoter alterations were found in IDH wild-type grade II diffuse IMAs. These latter tumors seem to have a good prognosis, and only 2 cases underwent anaplastic evolution. All of the HG IMAs presented at least one molecular alteration, with the most frequent one being the H3F3A p.K27M mutation. The H3F3A p.K27M mutation showed significant associations with OS and EFS after multivariate analysis. This study emphasizes that IMAs have distinct clinico-radiological, natural evolution and molecular landscapes from brain astrocytomas.
Similar content being viewed by others


Introduction
The recently updated 4th edition of the World Health Organization (WHO) Classification of Central Nervous System (CNS) tumors in 2016 (WHO 2016) drastically changed histological diagnosis in neuropathology by integrating molecular data into daily diagnostic practice [30, 51]. The current WHO 2016 classification of CNS tumors is based on clinical criteria, histology and molecular characteristics to achieve accurate determination of the prognosis and response to treatment and to improve patient management [30]. The WHO 2016 classification is applied using the same criteria for supra-tentorial, infra-tentorial, posterior fossa and intramedullary gliomas, regardless of location. However, the vast majority of molecular data on gliomas were obtained from studies of tumors localized in the brain [5, 50].Some studies, however, have shown that particular molecular alterations are related to tumor location. Fusions involving the BRAF and KIAA1549 genes are found in nearly 80% of cerebellar grade I astrocytomas but only 50–55% of non-cerebellar grade I cases [24]. Similarly, the p.K27M somatic mutation in the H3F3A gene (H3K27M) [41] predominates in high-grade (HG) infiltrative astrocytomas in midline locations, mainly the brain stem, thalamus and spinal cord [44].
Only a few studies specifically addressing intramedullary gliomas are available. Intramedullary tumors are rare CNS neoplasms accounting for 2 to 4% of all CNS tumors [41, 48]. The majority of these (80%) are gliomas, which are ependymomas (60–70%) and astrocytomas (30–40%) [4].
The few available studies specific to the molecular alterations of intramedullary astrocytomas (IMAs) have been performed and have shown that the most frequent recurrent molecular alterations are fusions involving KIAA1549-BRAF and H3K27M mutations [41]. To date, very few cases with IDH mutations have been described in IMAs, and these mutations were not classic IDH1 p.R132H and IDH2 p.R172H mutations [9, 12, 41, 47, 54].
Nevertheless, while the genetic profiles of brain astrocytomas have been largely established, those of uncommon IMAs remain to be defined. The present study aimed to correlate clinical, radiological and molecular data of IMAs to improve the current knowledge about the prognosis and molecular profile of these tumors.
Materials and methods
Patient cohort
Institutional Review Board approval for a retrospective analysis of archival biobank tissue was obtained from Biobanque Hôpital Erasme-ULB (BERA), BE_NBWB1, Biothèque Wallonie Bruxelles (BWB), BBMRI-ERIC) and Biolibrary of Saint-Luc University Hospital, together with ethical agreement. For the present study, the following inclusion criteria were defined: pathological diagnosis of LG or HG astrocytoma and spine location. We excluded cases with a secondary supratentorial location at diagnosis. Pathological diagnosis was reviewed by two neuropathologists (LL and IS) according to the WHO 2016 classification [30]. According to the cIMPACT-NOW (the Consortium to Inform Molecular and Practical Approaches to CNS Tumor Taxonomy) Update 4, the presence of the KIAA1549-BRAF fusion gene led to grade I pilocytic astrocytoma diagnosis in cases for which a differential diagnosis between grade I pilocytic and grade II diffuse astrocytomas could not be made [13]. Grade III astrocytoma diagnosis was based on mitotic activity, high cellularity, nuclear atypia without features of glioblastoma (necrosis and microvascular proliferation). To note, for the three grade III astrocytomas, as surgical resection was not complete according to surgical reports, we could not exclude undersampled glioblastoma. The final cohort consisted of 61 patients with IMAs diagnosed between 1989 and 2019 from Erasme and Saint-Luc University Hospital. Twenty-six of the tumors were grade I pilocytic astrocytomas, 17 were grade II diffuse astrocytomas, 3 were grade III astrocytomas and 12 grade IV astrocytomas. Three cases were ruled LG astrocytomas because no diagnosis of grade I or grade II could be made. To compare the molecular profile of this cohort of IMAs with their brain counterparts, we used a set of 117 samples obtained from astrocytoma patients consecutively diagnosed between 2017 and 2019 that were not located in spine and that were analyzed by next-generation sequencing (NGS) in our daily practical routine diagnosis setting using gene-targeted “clinical glioma” and “KIAA1549-BRAF fusion” panels (see below). This series included 16 grade I astrocytomas, 13 grade II astrocytomas, 13 grade III astrocytomas and 75 grade IV astrocytomas.
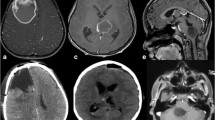
Magnetic resonance imaging (MRI) exams were reviewed for available cases (n = 34) by an expert neuroradiologist (DB). For the remaining cases, imaging features were collected from MRI reports. The imaging features assessed were location, signal T1 and T2 intensity, contrast enhancement, well-delineated vs. infiltrative pattern, cystic component and necrosis. Figure 1 illustrates representative radiological and pathological features of IMAs.

Representative radiological (sagittal MRI images) and histological (HE staining, 200×) features of intramedullary astrocytomas (IMAs) of grade I pilocytic (T2WI) (a), grade II diffuse (T2WI) (b), grade III (GdT1WI) (c) and grade IV (GdT1WI) (d) IMAs. HE, hematoxylin-eosin; MRI, magnetic resonance imaging; T2WI, T2 weighted image, GdT1WI, gadolinium enhanced T1 weighted images
Clinical variables were collected based on clinical and surgical reports: age, gender, extent of surgery (biopsy, partial or total resection), adjuvant treatments, follow-up duration and survival status. Based on MRI reports (contrast enhancement and/or tumor size increase), event-free survival (EFS) was assessed as the time until recurrence after gross total resection or disease progression after biopsy/partial resection, as defined by Pekmezci et al. [34] The median follow-up durations were 4.08 years (range: 0.1 to 27.8) and 1.92 years (range: 0.2 to 4.8) for LG and HG IMAs, respectively. For 54 cases, sufficient material from the primary resection samples was available for molecular analysis. For the remaining 7 cases, we used subsequent surgery samples to perform our molecular tests.
Next-generation sequencing (NGS) assays
Briefly, DNA and RNA from formalin-fixed paraffin-embedded (FFPE) tumor tissues were extracted using the QIAamp DNA FFPE Tissue Kit (Qiagen, Manchester, UK) and the Maxwell RSC DNA FFPE Kit (Promega Corporation, Madison, WI, USA) and were quantified using a Qubit 2.0 Fluorometer (ThermoFisher Scientific, Waltham, MA, USA). Library construction and quantification were performed using the Ion AmpliSeq Library Kit v2.0 and the Ion Library Quantitation Kit (ThermoFisher Scientific), respectively. Libraries were multiplexed and submitted for emulsion PCR using the Ion Chef System and were sequenced using the Ion GeneStudio S5 System, according to the manufacturer’s instructions (ThermoFisher Scientific).
DNA-based targeted NGS
For DNA analysis, two Ampliseq gene-targeted custom panels (“Clinical Glioma” and “Research Glioma” panels) were used to analyze a total of 33 genes commonly implicated in gliomas and the 1p and 19q regions (Supplementary Table S1) [6, 10]. Cases for which the number of mapped reads was < 100,000 and/or the average base coverage was <500x were considered non-informative.
RNA-based targeted NGS
To detect KIAA1549-BRAF fusions, we used an Ampliseq custom panel that tests 10 different fusions described in the COSMIC database (Sanger Institute Catalogue of Somatic Mutations in Cancer) (Supplementary Table S1). For each RNA sample, more than 20,000 total mapped reads were considered, as recommended by the manufacturer (ThermoFisher Scientific), with at least 5 control genes expressed over 250 reads.
Data analyses
For DNA analyses, reads were aligned against the hg19 reference genome with the Torrent Mapping Alignment Program (TMAP, ThermoFisher). After alignment, exonic nonsynonymous and splice variants were filtered to exclude those with fewer than 100 reads, present in the population with a minor allele frequency of more than 1% according to the 1000 Genomes project, with mutant allele coverage of fewer than 30 reads or with mutant allele frequency lower than 5% (except for well-known hotspot mutations). The final list of mutations was visualized with the Integrative Genomic Viewer (IGV, Broad Institute), and systematic sequencing errors or FFPE artifacts were removed. Curated information on variants was obtained from the gnomAD (genome aggregation database, https://gnomad.broadinstitute.org/), COSMIC (http://www.sanger.ac.uk/cosmic) and CbioPortal (https://www.cbioportal.org/) databases. Variants were classified as ones with pathogenic/potential clinical significance or as variants of unknown significance (VUS) following previous recommendations [29].
Ion reporter software (ThermoFisher) was used for copy number variation detection, including high-level amplification of EGFR and PDGFRA and homozygous deletion of CDKN2A. The algorithm uses normalized read coverage across amplicons to predict the copy number or ploidy state. Sample read coverage was compared to a baseline coverage constructed from 10 male control diploid DNA samples. Copy number variation (CNV) data were filtered to exclude regions with low confidence, as recommended by the manufacturer (ThermoFisher).
For RNA analyses, reads were aligned with the hg19 human reference genome, and fusions were identified by using Ion Reporter software v5.10 (ThermoFisher).
Statistical analysis
Statistical analyses were performed using Statistica software (StatSoft, Tulsa, USA).
After checking the application conditions, the chi-square test or Fisher’s exact test was used to analyze the associations between categorical variables.
Survival data were subjected to Kaplan-Meier analysis and the log-rank test. Multivariate Cox regression method was also applied. Overall survival (OS) and event-free survival (EFS) were calculated from the initial diagnosis. To include categorical variables in the multivariate models, we created dummy variables as follows. The extent of resection was introduced by means of 2 binary variables: biopsy (no/yes) and total resection (no/yes), with partial resection corresponding to the value of 0 for each of these 2 binary variables. In some cases, the total resection variable could be not included because of the problem of singular matrix decomposition for estimating model parameters. Statistical significance was defined as p < 0.05.
Results
Comparison of clinico-radiological features in low- and high-grade intramedullary astrocytomas
Table 1 details the radiological and clinical characteristics observed in our series of LG (46 cases) and HG (15 cases) IMA patients. The pediatric population (< 18 years old) consisted of 10 of 46 LG (22%) and 6 of 15 HG (40%) astrocytoma patients. Statistical tests showed that there were no significant differences between LG and HG astrocytomas in terms of age, gender, radiological features and the extension of surgical resection (Fisher test: p > 0.05). However, despite these radiological and clinical similarities, OS and EFS differed widely between patients with LG and HG tumors (Fig. 2a-b). HG astrocytoma patients presented an extremely poor prognosis, and no patient survived longer than 50 months (median OS and EFS of 23 and 6 months, respectively). In contrast, LG astrocytoma patients presented very good OS, with 90% of patients surviving after 50 months. Nevertheless, we observed frequent recurrence after gross total resection or disease progression after biopsy/partial resection among the LG IMA patients (median EFS, 67 months), although only 2 LG cases showed progression to a higher grade.

Overall survival (OS) and event-free survival (EFS) of low-grade (LG) and high-grade (HG) intramedullary astrocytomas. Kaplan-Meier curves of OS (a, c) and EFS (b, d) for all cases (a, b) and only for resected (partial and gross total resection) cases (c, d).p-values were calculated using the log-rank test
We observed heterogeneity in terms of the extent of surgical resection (Table 1). Gross total resection, partial resection and biopsy were performed in 17, 55 and 28% of patients, respectively, with no statistically significant difference between LG and HG IMAs. Therefore, given this heterogeneity, we applied multivariate Cox survival analysis to assess the potential contribution of surgery (considering the two dummy variables: biopsy and total resection) to OS and EFS, independently of tumor grade. For OS, only the biopsy variable could be added to the model (because of the problem of singular matrix decomposition), and it did not contribute to OS independently of grade (p = 0.15), whereas a highly significant contribution of grade was confirmed (p = 0.000007, Supplementary Table S2a). In contrast, biopsy is a negative prognostic variable which is independent of tumor grade for EFS (p = 0.003), and total surgical resection did not significantly contribute to better prognosis as an independent factor (p = 0.408) (Supplementary Table S2b and Fig. 2c-d).
Comparison of clinico-radiological features in grade I pilocytic and grade II diffuse intramedullary astrocytomas
Analyses of LG IMAs revealed no significant differences between grade I pilocytic and grade II diffuse astrocytomas in terms of age and gender (Table 2). Analyses of LG IMAs revealed no significant differences between grade I pilocytic and grade II diffuse astrocytomas in terms of age and gender (Table 2). We observed that 67% (12/18) of grade I pilocytic astrocytomas showed an infiltrative pattern and that only 33% (6/18) of them were well-delineated. 29% (5/17) grade II diffuse astrocytomas were well-delineated tumors and 71% (12/17) showed an infiltrative pattern. No significant difference was observed between grade I pilocytic and grade II diffuse astrocytomas in terms of infiltration. In contrast, we observed that grade I pilocytic astrocytomas were associated with contrast enhancement (96%, 25/26) significantly more often than grade II diffuse astrocytomas (59%, 10/17) (Fisher test: p = 0.004).
We observed a significant difference in terms of the proportion of patients who received surgery (total or partial resection) between grade I pilocytic and grade II diffuse astrocytomas (84%, 22/26 vs. 47%, 8/17; Fisher test: p = 0.011) (Table 2).
EFS was longer in grade I pilocytic astrocytomas (median EFS, 115 months) than in grade II diffuse astrocytomas (median EFS, 30 months) (log-rank test: p-value = 0.015) (Fig. 3a). We did not observe significant differences in EFS (p = 0.21, data not shown) for pediatric vs. adult LG patients.

Event-free survival (EFS) of grade I pilocytic and II diffuse intramedullary astrocytomas. Kaplan-Meier curves of EFS for grade I pilocytic and grade II diffuse IMAs without (a) and after (b) stratification using the extent of surgical resection: biopsy vs. (partially or totally) resected cases. p-values were calculated using the log-rank test
Among LG tumors, surgery strongly impacted EFS in both grade I pilocytic and grade II diffuse IMAs (log-rank test: p-value = 0.0025, Fig. 3b). As shown in Fig. 3b, there were no statistically significant differences in terms of EFS between grade I and II patients, either in biopsy or in resected cases (log-rank tests: p = 0.889 and p = 0.062, respectively). However, without distinguishing between grade I and II, there was a statistically significant difference in EFS between biopsy and resected LG cases (p = 0.0008, data not shown).
Multivariate Cox regression combining grade (I vs. II) and two surgery variables (biopsy and total resection) revealed that only the absence of surgery (i.e., biopsy) significantly and negatively impacted the EFS of LG astrocytomas, independently of the other variables in the model (Supplementary Table S3). Additional analyses showed that none of the other clinico-radiological variables (listed in Table 2) contributed to the prognosis independent of the biopsy variable (data not shown).
Molecular profiles of intramedullary astrocytomas
The molecular findings are summarized in Fig. 4. The most common mutations found in the cohort of IMAs studied here concerned TP53, H3F3A p.K27M and ATRX in 21% (13/61), 18% (11/61) and 13% (10/61) of cases, respectively. Pathogenic hotspot mutations were identified: BRAF p.V600E mutation (5%, 3/61), KRAS p.G12V/S and p.Q61R (5%, 3/61), IDH1 p.R132S (2%, 1/61), IDH2 p.R172M (2%, 1/61), ACVR1 p.G328V (2%, 1/61) and TERT promoter (2%, 1/61). Other variants were identified in the NF1, PDFGRA, TSC2, TSC1, MSH6, CIC, KEL, PIK3CA, PIK3R1, EGFR, TP73, LZTR1, DAXX, MET, FUBP1 and FOXR2 genes, most of them being VUS. In contrast to brain astrocytomas, no hotspot IDH1 p.R132H or IDH2 p.R172H mutations were identified, and none of our cases harbored the 1p19q codeletion. Regarding the KIAA1549-BRAF fusion, 16% of the contributive cases (10/54) were positive. The different breakpoints identified were KIAA1549(15)-BRAF(9) (8 cases), KIAA1549(16)-BRAF(9) (1 case) and KIAA1549(15)-BRAF(11) (1 case).

Molecular characterization of 61 intramedullary astrocytomas (IMAs) obtained by targeted next-generation-sequencing using research, clinical and KIAA1549-BRAF fusion panels. The figure summarizes the clinico-pathological features and molecular alterations found in the 61 IMAs. EFS, event-free survival; ND, no data available; s, second surgery sample; RGP, research glioma panel; CGP, clinical glioma panel
Alterations in genes involved in the MAP kinase signaling pathway were frequently found in LG IMAs (39%, 16/41 informative cases): BRAF alterations (mutations and fusions), KRAS and NF1 mutations were identified in 13, 2 and 1 cases, respectively. For grade I pilocytic IMAs, we observed MAP kinase signaling pathway alterations in 50% of cases (13/26). For the remaining grade I pilocytic IMAs, we did not detect any molecular alteration in 5 cases, while 8 cases presented at least one variant, including mutations of EGFR (one case), PDGFRA (one case), PIK3R1 and the TERT promoter (one case) (Fig. 4). Alterations in genes involved in the MAP kinase signaling pathway were found in 15% (2/13) of grade II diffuse IMAs, three had mutations in IDH (2 cases) and ACVR1 (1 case), and 8 grade II diffuse IMAs did not have any alterations identified with the gene-targeted strategy used here.
All HG IMA cases presented at least one mutation. The most frequent one was the H3F3A p.K27M mutation, which was found in 73% of cases (11/15) including 11 of 12 grade IV IMAs. Four of the HG IMAs did not harbor the H3F3A p.K27M mutation. Remarkably, the only grade IV IMA that did not carry this mutation was diagnosed in a Lynch syndrome context (case 63) and the others HG IMAs were grade III IMAs. The only alteration identified in 2 of these 3 grade III IMAs cases was the mutation of ATRX. ATRX mutations were identified in only 2 of 11 of the H3K27M-mutant cases (18%), while 3 of 4 HG H3K27M-wild-type IMAs harbored ATRX alterations.
Another common molecular alteration in HG IMAs was TP53 mutation (53%, 8/15), which was identified in most H3K27M-mutant tumors (64%, 7/11). In addition, the majority of NF1 mutations (3 of 4), as well as the only PIK3CA mutation identified, were found in HG IMAs. Importantly, none of the HG cases harbored KIAA1549-BRAF fusions and/or BRAF p.V600E mutations.
Molecular profile comparison of intramedullary and brain astrocytomas
We compared the molecular profiles of IMAs described above to those of their brain counterparts using a series of gliomas analyzed in the routine diagnostic setting of our laboratory. Examination of the gene-targeted “Clinical Glioma” and “KIAA1549-BRAF fusion” panels revealed that 98.2% (112/114) of brain astrocytomas had at least one molecular alteration (mutation or fusion), while only 65% (36/55) of IMAs had at least one alteration (Fisher test: p < 10− 6, Table 3).
At least one molecular alteration was found in 87.5% (14/16) and 71% (17/24) of brain and spinal grade I pilocytic astrocytoma cases, respectively (Fisher test: p = 0.27) with the KIAA1549-BRAF fusion being the most common molecular alteration found in both locations. Nevertheless, although the KIAA1549(16)-BRAF(9) fusion was most common in brain grade I pilocytic astrocytomas (64.3%, 9/14), the KIAA1549(15)-BRAF(9) fusion was the most common in spinal grade I pilocytic astrocytomas (80%, 8/10 Fisher test: p = 0.65). No other mutations were found in brain grade I pilocytic astrocytomas, while 21% (5/24) of grade I pilocytic IMAs presented mutations in the TP53 or ATRX gene (Fisher test: p = 0.071).
One hundred percent (13/13) of the brain grade II diffuse astrocytomas harbored at least one molecular alteration, compared to only 31.3% (5/16) in the spine (Fisher test: p = 0.00013). IDH1 p.R132H was the most common mutation found in brain grade II diffuse astrocytomas (54%, 7/13), while only 2 spine grade II diffuse astrocytomas cases harbored IDH mutations (12.5%, 2/16; Fisher test: p = 0.041), and these mutations were non-canonical IDH mutations. In both brain and spine tumors, TP53 and ATRX mutations were found concomitantly with IDH mutations. Among IDH-wild-type grade II diffuse astrocytomas, the TERT promoter mutation was the most common mutation found in the brain (67%, 4/6) compared to BRAF p.V600E (14%, 2/14) mutation in the spine (Fisher test: p = 0.037).
For HG astrocytomas, no comparison between grade III astrocytomas of the brain and spine was possible because of the small number of samples from the spine. However, all grade IV astrocytomas, either in the brain or in the spine, harbored at least one mutation. TERT promoter mutation was the most common molecular alteration found in grade IV astrocytomas of the brain (79%, 57/72), while the H3F3A p.K27M mutation was found in nearly all grade IV IMAs (92%, 11/12). Moreover, no IDH mutations were found in grade IV astrocytomas located in the spine, while 6.9% (5/72) of the grade IV astrocytomas were mutated in the brain (Fisher test: p = 1.0). Among IDH-wild-type grade IV brain astrocytomas, EGFR alterations (mutation and amplification) and TP53 and PTEN mutations were the most common molecular alterations after TERT promoter mutation. However, in spine grade IV astrocytomas, TP53 and ATRX mutations were the most common ones after H3F3A p.K27M mutation, and no PTEN and TERT promoter mutations were found.
Prognostic implications of molecular alterations in intramedullary astrocytomas
Among the 11 H3K27M-mutant IMA cases, 8 of 11 cases died, with a median OS of 20 months, and 7 of 11 showed recurrence after gross total resection or disease progression after biopsy/partial resection with a median EFS of 6 months. In contrast, KIAA1549-BRAF fusion was associated with good prognosis; none of the KIAA1549-BRAF-positive cases died, and only 2 of them had recurrence after gross total resection or disease progression after biopsy/partial resection after delays of 28 (case 28) and 115 months (case 10s).
Among grade I pilocytic IMAs (n = 26), the absence of the KIAA1549-BRAF fusion (n = 16) did not contribute significantly to the prognosis in terms of EFS (log rank test: p = 0.690, data not shown).
Of the 3 LG IMAs cases which died, two harbored TP53 mutations; one of these two cases harbored non-canonical (non-IDH1 p. R132H and non-IDH2 p.R172H) IDH mutation (IDH2 p.R172M) (case 21) and the other, an ACVR1 p.G328V mutation (case 50). For the third case (case 55), no molecular alterations could be identified. In the two LG IMAs cases that progressed to a higher grade, one harbored a non-canonical IDH mutation (IDH1 p.R132S) (case 31) and the other a BRAF p.V600E mutation (case 24).
Among HG IMAs (n = 15), H3K27M-wild-type cases (n = 4) seemed to have a better prognosis; only 1 case died (median follow-up of 29 months) compared to 8 cases among H3K27M-mutant cases (n = 11) (median follow-up of 20 months). Statistical analyses comparing H3K27M-mutant and H3K27M-wild-type HG IMAs could not be performed due to the small number of H3K27M-wild-type cases.
We then investigated whether molecular alterations significantly impacted patients’ survival independently of the surgical treatment. The OS-related results detailed in Supplementary Table S4a showed that only the H3K27M mutation made a significant contribution as a poor prognostic factor independent of the other variables in the model. Regarding EFS, (Supplementary Table S4b) only the biopsy and the H3K27M mutation variables contributed significantly and negatively to prognosis, independently of the other variables in the model. For EFS in grade I pilocytic and grade II diffuse IMAs (see Supplementary Table S5), no significant contribution of the molecular group indicators was found.
Discussion
Integration of some clinico-radiological criteria with histology is commonly performed for the diagnosis of brain gliomas [20, 49]. In the present study, we observed that these criteria were not helpful for IMAs. In brain gliomas, contrast enhancement is generally a common feature of HG gliomas [36, 49], although it is a non-specific finding and can also be found in grade I pilocytic astrocytoma [31, 33, 40, 49]. In our study, we did not observe a difference in contrast enhancement between LG and HG IMAs. This could be explained by the fact that 96% of grade I pilocytic IMAs included in our series showed contrast enhancement. Interestingly, similar infiltrative patterns were observed in both grade I pilocytic and grade II diffuse IMAs, while grade I pilocytic and grade II diffuse brain astrocytomas are, by definition, well-circumscribed and diffuse neoplasms, respectively. Nevertheless, in the spine, assessing the infiltrative/diffuse pattern by MRI can sometimes be challenging [2]. Our data are thus consistent with the literature and suggest that these classical radiological features are not helpful in the differential diagnosis between LG and HG IMAs.
Nevertheless, even if the histological grade can be challenging to assess in the spine [32, 41], it remains the most powerful prognostic marker [21, 52], with LG IMAs associated with better outcomes than HG IMAs [11, 21, 55]. Our study showed that the tumor grade was associated with better OS, while EFS was strongly impacted by tumor grade and surgery, with a higher rate of disease progression in cases in which only biopsy could be performed. In the literature, the impact of surgery on outcomes remains highly debated [16, 39]. It is interesting to note that although the univariate analysis showed that the EFS was longer in grade I pilocytic IMAs than in grade II diffuse IMAs, the multivariate analysis showed that when the type of surgery was taken into account, the distinction between grade I and II did not add significant prognostic value. This result was explained by the fact that, within each group of patients treated with the same type of surgery, the difference in EFS between grades I and II was not statistically significant. This result is consistent with Diaz et al., who did not find grade to be an independent prognostic factor among LG IMAs [11], and Karikari et al., who nearly reported the same rate of recurrence between grade I (41.7% recurrence) and grade II (40% recurrence) [26]. This outcome strongly contrasts with brain location, for which most grade I pilocytic astrocytomas are classically associated with better outcomes.
IMAs also appear to be molecularly distinct from brain astrocytomas. Grade I pilocytic astrocytomas were characterized by KIAA1549-BRAF fusions in both locations. However, the most frequent breakpoints found in IMAs were different than those usually found in brain grade I pilocytic astrocytomas, as also described by Faulkner et al. [14]. The impact of the presence of the KIAA1549-BRAF fusion on prognosis remains debated [14], with some studies showing associations with better outcomes for pediatric LG gliomas [22, 24]. In our study, KIAA1549-BRAF had no impact on either EFS or OS independent of surgery when considering all cases nor on EFS when considering only grade I pilocytic IMAs.
Molecular alterations of grade II diffuse astrocytomas differ according to their location. IDH mutations were found in half of the brain astrocytoma cases, but only in 2 of the 61 IMAs (with non-canonical mutations). IDH mutations are generally rare and mostly non-canonical in midline locations [35]. Previous reports of non-canonical IDH mutations in the spine are scarce and restricted to very few cases [8, 9, 12, 41, 54] with Takai et al. reporting one case with the same IDH1 p.R132S mutation that we found [47]. While for brain gliomas, IDH mutations are commonly associated with good prognosis, in our cohort of LG IMAs, the EFS of the two IDH-mutated cases was 17 and 14 months while for IDH-wild-type cases, the median EFS was 67 months. Among the 2 IDH-mutated cases, one died, and one progressed to a higher grade, as also reported by Takai et al., who described a short OS (11 months) for an IDH1 p.R132S-mutated grade II spinal cord astrocytoma [47]. This finding could suggest that rare IDH mutations could be related to more aggressive behavior in LG IMAs, but this hypothesis must be confirmed in a larger cohort.
As described recently, “adult-type” grade II diffuse astrocytomas with no IDH mutations often harbor EGFR amplification, TERT promoter mutations or combined whole chromosome 7 gain and whole chromosome 10 loss and have glioblastoma-like behavior [3]. In contrast, “pediatric-type” grade II diffuse astrocytomas, rarely exhibiting IDH mutations, were recently described to more frequently have “non-R132H IDH1” mutations in pediatric hemispheric diffuse astrocytomas [46], and they are associated with an indolent clinical behavior [13]. The molecular alterations of these “pediatric-type” grade II diffuse astrocytomas were recently described and concerned the BRAF p.V600E mutation, FGFR1 alterations or MYB or MYBL1 rearrangement [13, 37]. In our cohort of grade II diffuse IMAs, we did not observe EGFR or TERT promoter mutations. We observed BRAF p.V600E in 2 cases and found no other specific molecular alteration except for one hotspot ACVR1 p. G328V mutation, mostly described in “diffuse intrinsic pontine glioma” (DIPG) [23] and in one case of pediatric spinal glioblastoma in the literature [28]. However, FGFR1, MYB and MYBL1 were not covered by the gene-targeted NGS used in the present study. Recent studies have reported that chromosomal rearrangements in gliomas resulting in transcript fusion gene, such as NTRK 1/2/3 or FGFR1/2/3 fusions, could be therapeutic targets [15] and are implicated in clinical trials (Entrectinib [15] or Larotrectinib in pediatric patients [19]). Clinical trials involving FGFR inhibitors showed promising effects as targeted treatments for gliomas [15, 18]. Because of their potentially clinical implications, it could be interesting to test these fusion genes.
In the brain, the natural evolution of most “adult-type” grade II diffuse gliomas is to progress to a higher grade [11, 37]. Anaplastic evolution occurred in only two grade II diffuse IMAs in this cohort, in agreement with previous studies that reported only one of fifteen grade II diffuse [39] and six of thirteen grade III IMAs progressing to a higher grade [38]. This outcome could suggest a unique biological behavior of IMAs, and it raises the question of whether or not anaplastic evolution and therefore secondary grades III and IV astrocytomas in the spine occur, as rarely observed in “pediatric-type” LG gliomas [37].
In this cohort, nearly all grade IV IMAs were H3K27M mutants (92%), in line with previous reports, which described a range between 38 and 100% of H3K27M-mutant tumors among HG spinal astrocytomas [1, 8, 17, 25, 27, 32, 35, 41, 42, 44, 53]. All of the H3F3A mutations identified in our cohort consisted of the recurrent hotspot p.K27M mutation. We did not find any other mutations in genes encoding histone variants H3.1 or additional H3F3A mutations, in contrast with the recent report by Sloan et al., who reported H3F3A p.G34W in grade II and III spinal cord astrocytomas [43].We did not find TERT promoter mutations among HG IMAs, in contrast with those in the brain, and with two recent studies [1, 8]. Alvi et al. described distinct prognostic groups of HG IMAs according to the presence of TERT promoter mutations and H3K27M mutations [1]. The median OS of H3K27M-mutant IMAs in our cohort was 21 months, while Alvi et al. and Yi et al. reported a median OS of 48 months and 40 months, respectively [1, 53]. These results could suggest better OS for H3K27M-mutant IMAs than in other midline locations, for which the median OS is 12 months or less [7, 45]. Interestingly, none of the three grade III IMAs studied here showed H3K27M mutations or TERT promoter mutations, and the only alteration identified was the ATRX mutation in two of them.
No recurrent molecular alterations other than KIAA1549-BRAF fusion and H3F3A p.K27M mutations were identified in our cohort, in agreement with Shankar et al. [41] and the recent report of Zhang et al., who did not report any recurrent molecular alterations [54].
Conclusions
In conclusion, these specific clinico-radiological and molecular landscapes of IMAs suggest that diagnostic algorithms commonly used in the brain must be reviewed to be confirmed as appropriate for those in the spine. First, assessment of the imaging infiltrative/well-delineated pattern, as commonly used for the differential diagnosis of grade I pilocytic astrocytomas and diffuse grade II, III and IV astrocytomas, seems not to be useful in the spine. Moreover, classical molecular alterations such as IDH mutations, EGFR and TERT promoter mutations, associated with diagnosis and prognosis in the brain, do not seem to occur with the same frequency, have the same implications in spine or at least, deserve further study. In the brain, assessment of IDH mutations has been shown, as Ellezam et al. reported, to help to distinguish grade I pilocytic, typically IDH wild-type, from grade II diffuse astrocytomas [12]. In the spine, because of the rarity of IDH mutations, the absence of IDH mutations cannot help to distinguish grade I pilocytic astrocytoma from grade II diffuse astrocytoma. Moreover, IDH immunohistochemistry would not be useful because of the absence of classical IDH1 p.R132H in IMAs.
In addition, the prognostic implications of molecular alterations in IMAs must be well characterized since implications similar to those observed in the brain cannot be established. LG IMAs seem to have a clinical and a molecular profile more related to diffuse “pediatric-type” gliomas than those classically observed in the brain. HG IMAs are strongly related to diffuse midline H3K27M mutant gliomas, and the H3F3A p.K27M mutation is an important molecular alteration to assess because of its prognostic implications.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- CNS:
-
Central Nervous System
- CGP:
-
Clinical Glioma Panel
- CNV:
-
Copy Number Variations
- H3F3A p.K27M:
-
H3K27M
- HG:
-
High-Grade
- IMAs:
-
Intramedullary Astrocytomas
- LG:
-
Low-Grade
- MRI:
-
Magnetic Resonance Imaging
- NGS:
-
Next Generation Sequencing
- OS:
-
Overall Survival
- EFS:
-
Event-Free Survival
- RGP:
-
Research Glioma Panel
- VUS:
-
Variants of Unknown Significance
- WHO:
-
World Health Organization
References
Alvi MA, Ida CM, Paolini MA, Kerezoudis P, Meyer J, Barr Fritcher EG, Goncalves S, Meyer FB, Bydon M, Raghunathan A (2019) Spinal cord high-grade infiltrating gliomas in adults: clinico-pathological and molecular evaluation. Mod Pathol 32:1236–1243. https://doi.org/10.1038/s41379-019-0271-3
Balériaux DLF (1999) Spinal cord tumors. Eur Radiol 9:1252–1258. https://doi.org/10.1007/s003300050831
Brat DJ, Aldape K, Colman H, Holland EC, Louis DN, Jenkins RB, Kleinschmidt-DeMasters BK, Perry A, Reifenberger G, Stupp R, von Deimling A, Weller M (2018) cIMPACT-NOW update 3: recommended diagnostic criteria for “Diffuse astrocytic glioma, IDH-wildtype, with molecular features of glioblastoma, WHO grade IV.”. Acta Neuropathol (Berl) 136:805–810. https://doi.org/10.1007/s00401-018-1913-0
Bruneau M, Riva M, Brotchi J (2016) Primary intramedullary tumors. In: van de Kelft E (ed) Surgery of the spine and spinal cord: a neurosurgical approach. Springer International Publishing, Cham, pp 699–716
Cairncross JG, Wang M, Jenkins RB, Shaw EG, Giannini C, Brachman DG, Buckner JC, Fink KL, Souhami L, Laperriere NJ, Huse JT, Mehta MP, Curran WJ (2014) Benefit from procarbazine, lomustine, and vincristine in oligodendroglial tumors is associated with mutation of IDH. J Clin Oncol Off J Am Soc Clin Oncol 32:783–790. https://doi.org/10.1200/JCO.2013.49.3726
Cantero D, Rodríguez de Lope Á, Moreno de la Presa R, Sepúlveda JM, Borrás JM, Castresana JS, D’Haene N, García JF, Salmon I, Mollejo M, Rey JA, Hernández-Laín A, Meléndez B (2018) Molecular study of long-term survivors of Glioblastoma by gene-targeted next-generation sequencing. J Neuropathol Exp Neurol 77:710–716. https://doi.org/10.1093/jnen/nly048
Castel D, Philippe C, Calmon R, Le Dret L, Truffaux N, Boddaert N, Pagès M, Taylor KR, Saulnier P, Lacroix L, Mackay A, Jones C, Sainte-Rose C, Blauwblomme T, Andreiuolo F, Puget S, Grill J, Varlet P, Debily M-A (2015) Histone H3F3A and HIST1H3B K27M mutations define two subgroups of diffuse intrinsic pontine gliomas with different prognosis and phenotypes. Acta Neuropathol (Berl) 130:815–827. https://doi.org/10.1007/s00401-015-1478-0
Chai R-C, Zhang Y-W, Liu Y-Q, Chang Y-Z, Pang B, Jiang T, Jia W-Q, Wang Y-Z (2020) The molecular characteristics of spinal cord gliomas with or without H3 K27M mutation. Acta Neuropathol Commun 8:40. https://doi.org/10.1186/s40478-020-00913-w
Deng L, Xiong P, Luo Y, Bu X, Qian S, Zhong W, Lv S (2018) Association between IDH1/2 mutations and brain glioma grade. Oncol Lett. https://doi.org/10.3892/ol.2018.9317
D’Haene N, Meléndez B, Blanchard O, De Nève N, Lebrun L, Van Campenhout C, Salmon I (2019) Design and validation of a gene-targeted, Next-Generation Sequencing Panel for Routine Diagnosis in Gliomas. Cancers 11. https://doi.org/10.3390/cancers11060773
Diaz-Aguilar D, ReFaey K, Clifton W, Durcanova B, Chen SG, Deen HG, Bydon M, Trifiletti DM, Pichelmann MA, Quiñones-Hinojosa A (2019) Prognostic factors and survival in low grade gliomas of the spinal cord: a population-based analysis from 2006 to 2012. J Clin Neurosci 61:14–21. https://doi.org/10.1016/j.jocn.2018.11.025
Ellezam B, Theeler BJ, Walbert T, Mammoser AG, Horbinski C, Kleinschmidt-DeMasters BK, Perry A, Puduvalli V, Fuller GN, Bruner JM, Aldape KD (2012) Low rate of R132H IDH1 mutation in infratentorial and spinal cord grade II and III diffuse gliomas. Acta Neuropathol (Berl) 124:449–451. https://doi.org/10.1007/s00401-012-1011-7
Ellison DW, Hawkins C, Jones DTW, Onar-Thomas A, Pfister SM, Reifenberger G, Louis DN (2019) cIMPACT-NOW update 4: diffuse gliomas characterized by MYB, MYBL1, or FGFR1 alterations or BRAFV600E mutation. Acta Neuropathol (Berl) 137:683–687. https://doi.org/10.1007/s00401-019-01987-0
Faulkner C, Ellis HP, Shaw A, Penman C, Palmer A, Wragg C, Greenslade M, Haynes HR, Williams H, Lowis S, White P, Williams M, Capper D, Kurian KM (2015) BRAF fusion analysis in Pilocytic Astrocytomas: KIAA1549-BRAF 15-9 fusions are more frequent in the midline than within the cerebellum. J Neuropathol Exp Neurol 74:867–872. https://doi.org/10.1097/NEN.0000000000000226
Ferguson SD, Zhou S, Huse JT, de Groot JF, Xiu J, Subramaniam DS, Mehta S, Gatalica Z, Swensen J, Sanai N, Spetzler D, Heimberger AB (2018) Targetable gene fusions associate with the IDH wild-type Astrocytic lineage in adult Gliomas. J Neuropathol Exp Neurol 77:437–442. https://doi.org/10.1093/jnen/nly022
Garcés-Ambrossi GL, McGirt MJ, Mehta VA, Sciubba DM, Witham TF, Bydon A, Wolinksy J-P, Jallo GI, Gokaslan ZL (2009) Factors associated with progression-free survival and long-term neurological outcome after resection of intramedullary spinal cord tumors: analysis of 101 consecutive cases: clinical article. J Neurosurg Spine 11:591–599. https://doi.org/10.3171/2009.4.SPINE08159
Gessi M, Gielen GH, Dreschmann V, Waha A, Pietsch T (2015) High frequency of H3F3A K27M mutations characterizes pediatric and adult high-grade gliomas of the spinal cord. Acta Neuropathol (Berl) 130:435–437. https://doi.org/10.1007/s00401-015-1463-7
Granberg KJ, Annala M, Lehtinen B, Kesseli J, Haapasalo J, Ruusuvuori P, Yli-Harja O, Visakorpi T, Haapasalo H, Nykter M, Zhang W (2017) Strong FGFR3 staining is a marker for FGFR3 fusions in diffuse gliomas. Neuro-Oncol 19:1206–1216. https://doi.org/10.1093/neuonc/nox028
Guerreiro Stucklin AS, Ryall S, Fukuoka K, Zapotocky M, Lassaletta A, Li C, Bridge T, Kim B, Arnoldo A, Kowalski PE, Zhong Y, Johnson M, Li C, Ramani AK, Siddaway R, Nobre LF, de Antonellis P, Dunham C, Cheng S, Boué DR, Finlay JL, Coven SL, de Prada I, Perez-Somarriba M, Faria CC, Grotzer MA, Rushing E, Sumerauer D, Zamecnik J, Krskova L, Garcia Ariza M, Cruz O, Morales La Madrid A, Solano P, Terashima K, Nakano Y, Ichimura K, Nagane M, Sakamoto H, Gil-da-Costa MJ, Silva R, Johnston DL, Michaud J, Wilson B, van Landeghem FKH, Oviedo A, McNeely PD, Crooks B, Fried I, Zhukova N, Hansford JR, Nageswararao A, Garzia L, Shago M, Brudno M, Irwin MS, Bartels U, Ramaswamy V, Bouffet E, Taylor MD, Tabori U, Hawkins C (2019) Alterations in ALK/ROS1/NTRK/MET drive a group of infantile hemispheric gliomas. Nat Commun 10:4343. https://doi.org/10.1038/s41467-019-12187-5
Guillevin R, Herpe G, Verdier M, Guillevin C (2014) Low-grade gliomas: the challenges of imaging. Diagn Interv Imaging 95:957–963. https://doi.org/10.1016/j.diii.2014.07.005
Hamilton KR, Lee SS, Urquhart JC, Jonker BP (2019) A systematic review of outcome in intramedullary ependymoma and astrocytoma. J Clin Neurosci 63:168–175. https://doi.org/10.1016/j.jocn.2019.02.001
Hawkins C, Walker E, Mohamed N, Zhang C, Jacob K, Shirinian M, Alon N, Kahn D, Fried I, Scheinemann K, Tsangaris E, Dirks P, Tressler R, Bouffet E, Jabado N, Tabori U (2011) BRAF-KIAA1549 fusion predicts better clinical outcome in pediatric low-grade astrocytoma. Clin Cancer Res 17:4790–4798. https://doi.org/10.1158/1078-0432.CCR-11-0034
Hoeman CM, Cordero FJ, Hu G, Misuraca K, Romero MM, Cardona HJ, Nazarian J, Hashizume R, McLendon R, Yu P, Procissi D, Gadd S, Becher OJ (2019) ACVR1 R206H cooperates with H3.1K27M in promoting diffuse intrinsic pontine glioma pathogenesis. Nat Commun 10:1023. https://doi.org/10.1038/s41467-019-08823-9
Horbinski C (2013) To BRAF or not to BRAF : is that even a question anymore? J Neuropathol Exp Neurol 72:2–7. https://doi.org/10.1097/NEN.0b013e318279f3db
Johnson A, Severson E, Gay L, Vergilio J, Elvin J, Suh J, Daniel S, Covert M, Frampton GM, Hsu S, Lesser GJ, Stogner-Underwood K, Mott RT, Rush SZ, Stanke JJ, Dahiya S, Sun J, Reddy P, Chalmers ZR, Erlich R, Chudnovsky Y, Fabrizio D, Schrock AB, Ali S, Miller V, Stephens PJ, Ross J, Crawford JR, Ramkissoon SH (2017) Comprehensive genomic profiling of 282 pediatric low- and high-grade Gliomas reveals genomic drivers, tumor mutational burden, and Hypermutation signatures. Oncologist 22:1478–1490. https://doi.org/10.1634/theoncologist.2017-0242
Karikari IO, Nimjee SM, Hodges TR, Erin C, Hughes BD, Powers CJ, Mehta AI, Carolyn H, Bagley CA, Isaacs RE, Haglund MM, Friedman AH (2011) Impact of tumor histology on Resectability and neurological outcome in primary intramedullary spinal cord tumors: a single-center experience with 102 patients. Neurosurgery 68:188–197. https://doi.org/10.1227/NEU.0b013e3181fe3794
Karremann M, Gielen GH, Hoffmann M, Wiese M, Colditz N, Warmuth-Metz M, Bison B, Claviez A, van Vuurden DG, von Bueren AO, Gessi M, Kühnle I, Hans VH, Benesch M, Sturm D, Kortmann R-D, Waha A, Pietsch T, Kramm CM (2018) Diffuse high-grade gliomas with H3 K27M mutations carry a dismal prognosis independent of tumor location. Neuro-Oncol 20:123–131. https://doi.org/10.1093/neuonc/nox149
Kline CN, Joseph NM, Grenert JP, van Ziffle J, Talevich E, Onodera C, Aboian M, Cha S, Raleigh DR, Braunstein S, Torkildson J, Samuel D, Bloomer M, Campomanes AGde A, Banerjee A, Butowski N, Raffel C, Tihan T, Bollen AW, Phillips JJ, Korn WM, Yeh I, Bastian BC, Gupta N, Mueller S, Perry A, Nicolaides T, Solomon DA (2017) Targeted next-generation sequencing of pediatric neuro-oncology patients improves diagnosis, identifies pathogenic germline mutations, and directs targeted therapy. Neuro-Oncol 19:699–709. https://doi.org/10.1093/neuonc/now254
Li MM, Datto M, Duncavage EJ, Kulkarni S, Lindeman NI, Roy S, Tsimberidou AM, Vnencak-Jones CL, Wolff DJ, Younes A, Nikiforova MN (2017) Standards and guidelines for the interpretation and reporting of sequence variants in Cancer. J Mol Diagn JMD 19:4–23. https://doi.org/10.1016/j.jmoldx.2016.10.002
Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, Ohgaki H, Wiestler OD, Kleihues P, Ellison DW (2016) The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol (Berl) 131:803–820. https://doi.org/10.1007/s00401-016-1545-1
Minehan KJ, Brown PD, Scheithauer BW, Krauss WE, Wright MP (2009) Prognosis and treatment of spinal cord astrocytoma. Int J Radiat Oncol 73:727–733. https://doi.org/10.1016/j.ijrobp.2008.04.060
Nagaishi M, Nobusawa S, Yokoo H, Sugiura Y, Tsuda K, Tanaka Y, Suzuki K, Hyodo A (2016) Genetic mutations in high grade gliomas of the adult spinal cord. Brain Tumor Pathol 33:267–269. https://doi.org/10.1007/s10014-016-0263-7
Pallud J, Capelle L, Taillandier L, Fontaine D, Mandonnet E, Guillevin R, Bauchet L, Peruzzi P, Laigle-Donadey F, Kujas M, Guyotat J, Baron M-H, Mokhtari K, Duffau H (2009) Prognostic significance of imaging contrast enhancement for WHO grade II gliomas. Neuro-Oncol 11:176–182. https://doi.org/10.1215/15228517-2008-066
Pekmezci M, Villanueva-Meyer JE, Goode B, Van Ziffle J, Onodera C, Grenert JP, Bastian BC, Chamyan G, Maher OM, Khatib Z, Kleinschmidt-DeMasters BK, Samuel D, Mueller S, Banerjee A, Clarke JL, Cooney T, Torkildson J, Gupta N, Theodosopoulos P, Chang EF, Berger M, Bollen AW, Perry A, Tihan T, Solomon DA (2018) The genetic landscape of ganglioglioma. Acta Neuropathol Commun 6:47. https://doi.org/10.1186/s40478-018-0551-z
Picca A, Berzero G, Bielle F, Touat M, Savatovsky J, Polivka M, Trisolini E, Meunier S, Schmitt Y, Idbaih A, Hoang-Xuan K, Delattre J-Y, Mokhtari K, Di Stefano AL, Sanson M (2018) FGFR1 actionable mutations, molecular specificities, and outcome of adult midline gliomas. Neurology 90:e2086–e2094. https://doi.org/10.1212/WNL.0000000000005658
POPE WB, BRANDAL G (2018) Conventional and advanced magnetic resonance imaging in patients with high-grade glioma. Q J Nucl Med Mol Imaging 62:239–253. https://doi.org/10.23736/S1824-4785.18.03086-8
Qaddoumi I, Orisme W, Wen J, Santiago T, Gupta K, Dalton JD, Tang B, Haupfear K, Punchihewa C, Easton J, Mulder H, Boggs K, Shao Y, Rusch M, Becksfort J, Gupta P, Wang S, Lee RP, Brat D, Collins VP, Dahiya S, George D, Konomos W, Kurian KM, McFadden K, Serafini LN, Nickols H, Perry A, Shurtleff S, Gajjar A, Boop FA, Klimo PD, Mardis ER, Wilson RK, Baker SJ, Zhang J, Wu G, Downing JR, Tatevossian RG, Ellison DW (2016) Genetic alterations in uncommon low-grade neuroepithelial tumors: BRAF, FGFR1, and MYB mutations occur at high frequency and align with morphology. Acta Neuropathol (Berl) 131:833–845. https://doi.org/10.1007/s00401-016-1539-z
Santi M, Mena H, Wong K, Koeller K, Olsen C, Rushing EJ (2003) Spinal cord malignant astrocytomas: Clinicopathologic features in 36 cases. Cancer 98:554–561. https://doi.org/10.1002/cncr.11514
Seki T, Hida K, Yano S, Aoyama T, Koyanagi I, Sasamori T, Hamauch S, Houkin K (2016) Clinical factors for prognosis and treatment guidance of spinal cord astrocytoma. Asian Spine J 10:748. https://doi.org/10.4184/asj.2016.10.4.748
Seo HS, J-h K, Lee DH, Lee YH, S-i S, Kim SY, Na DG (2010) Nonenhancing intramedullary Astrocytomas and other MR imaging features: a retrospective study and systematic review. Am J Neuroradiol 31:498–503. https://doi.org/10.3174/ajnr.A1864
Shankar GM, Lelic N, Gill CM, Thorner AR, Van Hummelen P, Wisoff JH, Loeffler JS, Brastianos PK, Shin JH, Borges LF, Butler WE, Zagzag D, Brody RI, Duhaime A-C, Taylor MD, Hawkins CE, Louis DN, Cahill DP, Curry WT, Meyerson M (2016) BRAF alteration status and the histone H3F3A gene K27M mutation segregate spinal cord astrocytoma histology. Acta Neuropathol (Berl) 131:147–150. https://doi.org/10.1007/s00401-015-1492-2
Shows J, Marshall C, Perry A, Kleinschmidt-DeMasters BK (2016) Genetics of Glioblastomas in rare anatomical locations: spinal cord and optic nerve: letter to the editor. Brain Pathol 26:120–123. https://doi.org/10.1111/bpa.12327
Sloan EA, Cooney T, Oberheim Bush NA, Buerki R, Taylor J, Clarke JL, Torkildson J, Kline C, Reddy A, Mueller S, Banerjee A, Butowski N, Chang S, Mummaneni PV, Chou D, Tan L, Theodosopoulos P, McDermott M, Berger M, Raffel C, Gupta N, Sun PP, Li Y, Shah V, Cha S, Braunstein S, Raleigh DR, Samuel D, Scharnhorst D, Fata C, Guo H, Moes G, Kim JYH, Koschmann C, Van Ziffle J, Onodera C, Devine P, Grenert JP, Lee JC, Pekmezci M, Phillips JJ, Tihan T, Bollen AW, Perry A, Solomon DA (2019) Recurrent non-canonical histone H3 mutations in spinal cord diffuse gliomas. Acta Neuropathol (Berl) 138:877–881. https://doi.org/10.1007/s00401-019-02072-2
Solomon DA, Wood MD, Tihan T, Bollen AW, Gupta N, Phillips JJJ, Perry A (2016) Diffuse midline Gliomas with histone H3-K27M mutation: a series of 47 cases assessing the Spectrum of morphologic variation and associated genetic alterations: diffuse midline gliomas with histone H3-K27M mutation. Brain Pathol 26:569–580. https://doi.org/10.1111/bpa.12336
Sturm D, Witt H, Hovestadt V, Khuong-Quang D-A, Jones DTW, Konermann C, Pfaff E, Tönjes M, Sill M, Bender S, Kool M, Zapatka M, Becker N, Zucknick M, Hielscher T, Liu X-Y, Fontebasso AM, Ryzhova M, Albrecht S, Jacob K, Wolter M, Ebinger M, Schuhmann MU, van Meter T, Frühwald MC, Hauch H, Pekrun A, Radlwimmer B, Niehues T, von Komorowski G, Dürken M, Kulozik AE, Madden J, Donson A, Foreman NK, Drissi R, Fouladi M, Scheurlen W, von Deimling A, Monoranu C, Roggendorf W, Herold-Mende C, Unterberg A, Kramm CM, Felsberg J, Hartmann C, Wiestler B, Wick W, Milde T, Witt O, Lindroth AM, Schwartzentruber J, Faury D, Fleming A, Zakrzewska M, Liberski PP, Zakrzewski K, Hauser P, Garami M, Klekner A, Bognar L, Morrissy S, Cavalli F, Taylor MD, van Sluis P, Koster J, Versteeg R, Volckmann R, Mikkelsen T, Aldape K, Reifenberger G, Collins VP, Majewski J, Korshunov A, Lichter P, Plass C, Jabado N, Pfister SM (2012) Hotspot mutations in H3F3A and IDH1 define distinct epigenetic and biological subgroups of Glioblastoma. Cancer Cell 22:425–437. https://doi.org/10.1016/j.ccr.2012.08.024
Sumerauer D, Krskova L, Vicha A, Misove A, Mamatjan Y, Jencova P, Vlckova M, Slamova L, Vanova K, Liby P, Taborsky J, Koblizek M, Klubal R, Kyncl M, Zadeh G, Stary J, Zamecnik J, Ramaswamy V, Zapotocky M (2020) Rare IDH1 variants are common in pediatric hemispheric diffuse astrocytomas and frequently associated with Li-Fraumeni syndrome. Acta Neuropathol (Berl) 139:795–797. https://doi.org/10.1007/s00401-019-02118-5
Takai K, Tanaka S, Sota T, Mukasa A, Komori T, Taniguchi M (2017) Spinal cord astrocytoma with Isocitrate dehydrogenase 1 gene mutation. World Neurosurg 108:991.e13–991.e16. https://doi.org/10.1016/j.wneu.2017.08.142
Teng YD, Abd-El-Barr M, Wang L, Hajiali H, Wu L, Zafonte RD (2019) Spinal cord astrocytomas: progresses in experimental and clinical investigations for developing recovery neurobiology-based novel therapies. Exp Neurol 311:135–147. https://doi.org/10.1016/j.expneurol.2018.09.010
Upadhyay N, Waldman AD (2011) Conventional MRI evaluation of gliomas. Br J Radiol 84:S107–S111. https://doi.org/10.1259/bjr/65711810
Van den Bent MJ, Brandes AA, Taphoorn MJB, Kros JM, Kouwenhoven MCM, Delattre J-Y, Bernsen HJJA, Frenay M, Tijssen CC, Grisold W, Sipos L, Enting RH, French PJ, Dinjens WNM, Vecht CJ, Allgeier A, Lacombe D, Gorlia T, Hoang-Xuan K (2013) Adjuvant procarbazine, lomustine, and vincristine chemotherapy in newly diagnosed anaplastic oligodendroglioma: long-term follow-up of EORTC brain tumor group study 26951. J Clin Oncol Off J Am Soc Clin Oncol 31:344–350. https://doi.org/10.1200/JCO.2012.43.2229
Wood MD, Halfpenny AM, Moore SR (2019) Applications of molecular neuro-oncology - a review of diffuse glioma integrated diagnosis and emerging molecular entities. Diagn Pathol:14. https://doi.org/10.1186/s13000-019-0802-8
Xiao R, Abdullah KG, Miller JA, Lubelski D, Steinmetz MP, Shin JH, Krishnaney AA, Mroz TE, Benzel EC (2016) Molecular and clinical prognostic factors for favorable outcome following surgical resection of adult intramedullary spinal cord astrocytomas. Clin Neurol Neurosurg 144:82–87. https://doi.org/10.1016/j.clineuro.2016.03.009
Yi S, Choi S, Shin DA, Kim DS, Choi J, Ha Y, Kim KN, Suh C-O, Chang JH, Kim SH, Yoon DH (2019) Impact of H3.3 K27M Mutation on Prognosis and Survival of Grade IV Spinal Cord Glioma on the Basis of New 2016 World Health Organization classification of the central nervous system. Neurosurgery 84:1072–1081. https://doi.org/10.1093/neuros/nyy150
Zhang M, Iyer RR, Azad TD, Wang Q, Garzon-Muvdi T, Wang J, Liu A, Burger P, Eberhart C, Rodriguez FJ, Sciubba DM, Wolinsky J-P, Gokaslan Z, Groves ML, Jallo GI, Bettegowda C (2019) Genomic landscape of intramedullary spinal cord Gliomas. Sci Rep 9. https://doi.org/10.1038/s41598-019-54286-9
Zou Y, Sun J, Zhou Y, Bai HX, Huang X, Babu R, Landi A, Foong KS, Zhang Z, Woo JH, Tao Y, Li X, Tang X, Xiao B, Zhang PJ, Yang L (2018) Prognostic factors and treatment of spinal Astrocytomas: a multi-institutional cohort analysis. SPINE 43:E565–E573. https://doi.org/10.1097/BRS.0000000000002485
Acknowledgements
The authors thank Dominique Penninck, Sarah De Clercq and Cédric Balsat for their logistical help. CD was a Senior Research Associate with the F.N.R.S. (Belgian National Fund for Scientific Research). CMMI is supported by the European Regional Development Fund and the Walloon Region (Wallonia-biomed, #411132-957270, project “CMMI- ULB”).
Funding
This work was performed with the support of grants awarded by the “Fonds Erasme” for Medical Research (Brussels, Belgium) and by funding from the “Fonds Yvonne Boël” (Brussels, Belgium).
Author information
Authors and Affiliations
Contributions
L.L., M.R. and J.L. participated in selecting the samples and collecting clinical information. J.B., M.B. and O.D.W. participated in the acquisition of samples. L.L. and D.B. participated in the acquisition of clinical and radiological data. D.B. performed the radiological review. L.L., B.M., C.D., N.D. and I.S. made contributions to the conception of the study, performed the analysis and interpretation of the data and wrote the manuscript. L.L., B.M., O.B., N.D.N., N.D. and C.V.C. performed molecular analyses and participated in the interpretation of molecular data. I.S. and L.L. performed histological examinations. All of the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The present study was approved by the Ethical Committee of the Erasme University Hospital (Brussels, Belgium; ref., P2017/319). According to Belgian law, no written informed consent was required for archival material in the context of retrospective studies. The ethical committee thus waived the requirement for written informed consent from the participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1: Table S1.
List of genes, copy number variations (CNV) and KIAA1549-BRAF fusions tested.
Additional file 2: Table S2.
Prognosis Model for all cases.
Additional file 3: Table S3.
Event-Free Survival (EFS) Prognosis Model for LG cases (grade I and grade II only).
Additional file 4: Table S4.
Prognosis Model including molecular data for all cases.
Additional file 5: Table S5.
Event-free Survival (EFS) Prognosis Model including molecular data for grade I pilocytic and grade II diffuse intramedullary astrocytomas.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Lebrun, L., Meléndez, B., Blanchard, O. et al. Clinical, radiological and molecular characterization of intramedullary astrocytomas. acta neuropathol commun 8, 128 (2020). https://doi.org/10.1186/s40478-020-00962-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40478-020-00962-1