
Abstract
Background
Surgical site infection (SSI) is a common post-operative complication causing significant morbidity and mortality. Many SSI occur after discharge from hospital. Post-discharge SSI surveillance in low and middle income countries needs to be improved.
Methodology
We conducted an observational cohort study in Dodoma, Tanzania to examine the sensitivity and specificity of telephone calls to detect SSI after discharge from hospital in comparison to a gold standard of clinician review. Women undergoing caesarean section were enrolled and followed up for 30 days. Women providing a telephone number were interviewed using a structured questionnaire at approximately days 5, 12 and 28 post-surgery. Women were then invited for out-patient review by a clinician blinded to the findings of telephone interview.
Results
A total of 374 women were enrolled and an overall SSI rate of 12% (n = 45) was observed. Three hundred and sixteen (84%) women provided a telephone number, of which 202 had at least one telephone interview followed by a clinical review within 48 h, generating a total of 484 paired observations. From the clinical reviews, 25 SSI were diagnosed, of which telephone interview had correctly identified 18 infections; telephone calls did not incorrectly identify SSI in any patients. The overall sensitivity and specificity of telephone interviews as compared to clinician evaluation was 72 and 100%, respectively.
Conclusion
The use of telephone interview as a diagnostic tool for post-discharge surveillance of SSI had moderate sensitivity and high specificity in Tanzania. Telephone-based detection may be a useful method for SSI surveillance in low-income settings with high penetration of mobile telephones.
Similar content being viewed by others


Introduction
Surgical site infection (SSI) is one of the most common healthcare-associated infections (HAI) [1, 2], especially in low and middle-income countries (LMIC) [3,4,5]. Caesarean section (CS) is among the most frequent surgical interventions in women worldwide [6, 7]. However, CS increases the risk of post-partum infections by 5 to 20-fold compared to vaginal delivery [8, 9]. Despite modern surgical techniques and antibiotic prophylaxis, SSI is still contributing significantly to morbidity, mortality and healthcare-associated costs [6, 10, 11]. Data from Tanzania report SSI incidences of 10.9, 24% and as high as 48% [6, 12, 13]. Many SSI occur after discharge from hospital, typically occurring between 5 and 10 days post-operatively. The burden of SSI is therefore liable to be underestimated by any HAI surveillance system that does not capture information after discharge from hospital [14, 15].
There is no scientific consensus on an ideal method of detecting SSI after discharge from hospital and different approaches have been employed in different settings [16,17,18,19]. However, there is emerging evidence that patients are able to diagnose and report their own SSI with an acceptable accuracy if prompted with the appropriate questions via telephone calls [14,15,16, 20]. Evaluations of such telephone-based methods in LMIC including comparison to a “gold-standard” reference diagnosis is very limited so substantial uncertainty remains about the reliability of these methods [21].
The aim of this study was to examine the feasibility, sensitivity and specificity of the use of a structured questionnaire administered through telephone interview as a method for detecting post-discharge SSI after CS. The survey was conducted at a tertiary hospital in Tanzania. We also sought to estimate the overall risk of SSI occurring in a 30-day post-operative period in this population.
Methodology
Study design
Prospective observational cohort study.
Study site
Obstetrics and Gynaecology Department of the Dodoma Regional Referral Hospital (DRRH), Dodoma, Tanzania. The average number of women delivering at DRRH is around 1000 per month, with CS accounting for around 20% of deliveries.
Period of study
Two month enrollment period from May to June 2015.
Study population
All women admitted at DRRH labour ward who underwent CS were enrolled within 24 h of surgery and were followed up for 30 days for development of SSI, in accordance with the United States Centers for Disease Control and Prevention (CDC) criteria for diagnosis of SSI [20].
Data collection and follow up
Data were retrieved from the patients using a structured questionnaire and through medical records. All women were asked to provide one or more mobile telephone numbers, either a personal phone and/or that of a relative for communication after discharge. Before discharge, women were educated on proper wound care at home and were asked to attend Makole Health Centre (MHC) for wound inspection, dressing and consultation with medical doctors at day 7 post-CS. Before this scheduled visit, all women who provided a mobile number were contacted on day 5 or 6 post-CS and a brief structured interview regarding the status of the wound was conducted. The telephone interview questions were related to signs and symptoms of infection including history of fever, pus discharge from the wound, pain or redness at the surgical wound, use of antibiotics or any drugs to support wound healing and presence of obvious gaping of the wound or protrusion of internal structures. Patients were also reminded to attend MHC within 48 h of the phone interview. The phone call was performed by a clinically-trained investigator or a registered nurse who had received appropriate training on the telephone interview questionnaire. The diagnosis of SSI was made using an algorithm based on the CDC classification system [22]. At the MHC follow-up clinic, patients were evaluated by different clinicians who were trained on the CDC criteria for diagnosis of SSI and unaware of the findings of the telephone interview. Phone call interviews were also performed on days 12 and 28 post-CS prior to additional scheduled visits on days 14 and 30 post-CS, respectively. Patients did not receive any kind of incentives or fare reimbursements to attend the clinic during the study.
Data analysis
Data were analysed using STATA software (Version 12.0, STATA Corp, College Station, Texas, USA). To determine the sensitivity and specificity of phone calls, an analysis was performed using all paired observations of telephone call interview and clinician review (which was considered as the gold standard) that occurred within 48 h of each other. We performed the analysis using the paired observations at each separate time-point and at all the three time-points combined.
Results
A total of 374 women who underwent CS during the study period were enrolled. Patients’ characteristics are shown in Table 1.
Use of telephone calls in detection of SSIs
Three hundred and sixteen (84%) enrolled women provided a telephone number. Phone calls were successfully made on at least one occasion to 274 patients, representing 87% (274/316) of patients with a telephone number. Forty-two (13%) patients were not reachable after at least two attempts. Among the 274 successfully interviewed patients, 202 attended for a clinician review within 48 h of the interview at least once during the study. A total of 484 paired observations (telephone call interviews and clinician reviews) within 48 h of each other were generated across the three time-points. From all observation pairs, 18 telephone interviews identified an SSI, all sub-classified as “superficial”. In clinical review, 25 SSI were diagnosed corresponding to an SSI rate of 12.3%, including all 18 Superficial SSI identified by telephone interview, plus 7 further infections (4 Superficial, 2 Deep and 1 Organ/Space). When considering just single time-points, similar proportions of patient with SSI were identified at the day 7 and day 14 time-points, but no patients with SSI were identified at the day 30 time-point, either by telephone call or clinical review as shown in Table 2.
Using this combined set of all paired observations, the sensitivity and specificity of telephone interviews against a clinical review gold-standard were 72% (95% CI 50.6–87.9) and 100% (95% CI 99.2–100), respectively while positive predictive value (PPV) and negative predictive value (NPV) were 100% (95% CI 81.5–100) and 95.9% (95% CI 96.9–99.4), respectively as presented in Table 2. Logistically, each telephone call interview required between 3 and 5 min and the direct cost was approximately US$0.50.
Risk of SSI, based on different follow-up strategies
Out of 374 women, an overall SSI rate of 12.0% (n = 45) was observed and confirmed by clinical review. All SSI occurred after initial discharge from hospital which was typically within 10 days after CS. The median interval from surgery to clinical diagnosis was 8 days (IQR 7–11 days). Sixty eight percent (n = 254) of enrolled women attended the outpatient clinic at least once within 30 days post-CS, with complete loss to clinical follow-up occurring in 120 (32%) women. According to the CDC classification of SSI, 42/45 (93%) were Superficial, 2 (4.4%) were Deep and 1 (2.2%) was an Organ/Space infection. As shown in Table 3, we retrospectively determined what SSI risk might have been found by using partial elements of the telephone-based SSI surveillance. Based on these data, we find that combination of two phone calls at day 7 and day 14 would have detected almost 90% of SSI cases.
Discussion
The overall sensitivity and specificity of telephone call interview to detect SSI in comparison to direct clinical evaluation was 72 and 100%, based on 484 paired observations. The sensitivity was not statistically different at day 7 (79%) and day 14 (64%). No infections were detected by telephone call interviews or clinical reviews to detect SSI at day 30 post-surgery, suggesting that there is limited value for reviews, either clinical or telephone-based at this time-point.
Our estimates of the sensitivity and specificity of this method might have been affected by the 48 h interval between telephone interview and review by clinicians, since some infections may have become symptomatic at this time. This might lead to underestimation of the sensitivity. A substantial number of patients were not reachable by mobile phones, which means that the use of phone calls as a stand-alone tool would be unlikely to detect all SSI.
Some other studies have described a role for telephone call interviews for SSI surveillance in LMIC [13, 16, 21, 23]. Our study is, to our knowledge, the largest-ever direct evaluation of the role of telephone interview in SSI surveillance in an African country. The results from our study are similar to a smaller-scale research conducted in Kenya, which also observed moderate sensitivity and high specificity of phone calls as a stand-alone test for SSI [14]. However, telephone interview did not detect the “Deep” and “Organ/Space”” SSI that were detected in this study, which is potentially a cause for concern as these represent the most serious forms of SSI.
As in many other SSI studies [21, 24, 25], the post-discharge surveillance was affected by significant loss to follow up. The failure to attend the clinic might be related to the difficulty, distance and cost for women to reach the clinic. For clinical review-based methods of SSI surveillance, this means that an operating centre is liable to miss the occurrence of post-operative complication and hence underestimate local SSI risks. However, if SSI surveillance systems made greater use of telephone call-based methods, more accurate estimates might be obtained.
In Tanzania, as in many LMICs, there is now relatively high penetration of mobile phones for communication and other uses including electronic money transfers. This technology represents a significant opportunity for public health and disease surveillance systems. Amongst women of child-bearing age in Dodoma, 85% were able to provide a mobile phone number. However, there are also barriers to contacting by phone beyond ownership, which is reflected by our finding that only 87% of those providing a phone number were successfully contacted. As in other studies, the telephone call interviews were well received by both the patients and the healthcare workers].
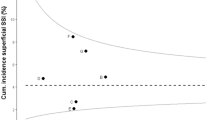
The cumulative incidence of post-CS SSI in this study was 12% which is substantially reduced from an incidence of 48% described at DRRH in 2013 in a previous study [26]. Given the substantial loss to follow-up, this value may underestimate the true occurrence of post-operative risk of infection. This SSI rate is lower than typically reported in Tanzania, however is comparable to other studies conducted in LMICs but it is significantly higher than those typically reported in high-income countries (6,10,12,26)]. As observed in other similar studies, the commonest type of infection was Superficial [6, 10, 12, 27]. According to our data, the majority of SSIs were detected within ten days post-CS, indicating that contamination in the operating theatre is liable to be a significant underlying causal factor [6, 28].
Conclusion
The occurrence of SSI represents a substantial risk after surgery in LMICs and appropriate detection of these events is difficult when patients have to travel a long distance to reach healthcare facilities. Case ascertainment of SSI can be achieved by a variety of methods and a combined approach can be considered. Potentially, the use of a structured questionnaire administered through telephone calls for post-operative surveillance might reduce loss to follow-up and improve the quality of surveillance data. However, although we found the specificity to be very high, further work is needed to explore how the sensitivity of telephone-based diagnosis and ability to make contact with patients by telephone could be further improved, especially in settings where few patients are able to attend for clinical review.
Abbreviations
- CDC:
-
Centres for diseases control and prevention
- CS:
-
Caesarean section
- DRRH:
-
Dodoma Regional Referral Hospital
- HAI:
-
Healthcare-associated infections
- IQR:
-
Inter quartile range
- LMIC:
-
Lower and middle-income country
- MHC:
-
Makole Health Centre
- NPV:
-
Negative predictive value
- PPV:
-
Positive predictive value
- SSI:
-
Surgical site infection
References
Bagnall NM, Vig S, Trivedi P. Surgical-site infection. Surgery. 2009;27(10):426–30.
Smyth ET. Emmerson a M. Surgical site infection surveillance. J Hosp Infect. 2000;45(3):173–84.
Nejad SB, Allegranzi B, Syed S, Ellis B, Pittet D. Health-care-associated infection in Africa: a systematic review. Bull World Health Organ. 2011;89(10):757–65.
Allegranzi B, Nejad SB, Combescure C, Graafmans W, Attar H, Donaldson L, et al. Burden of endemic health-care-associated infection in developing countries : systematic review and meta-analysis. Lancet. 2011;377(9761):228–41.
Rothe C, Schlaich C, Thompson S. Healthcare-associated infections in sub-Saharan Africa. J Hosp Infect. 2013;85(4):257–67.
Mpogoro FJ, Mshana SE, Mirambo MM, Kidenya BR, Gumodoka B, Imirzalioglu C. Incidence and predictors of surgical site infections following caesarean sections at Bugando medical Centre, Mwanza, Tanzania. Antimicrob Resist Infect Control. 2014;3:25.
Hadiati DR, Hakimi M, Nurdiati DS. Skin preparation for preventing infection following caesarean section. Cochrane Database of Systematic Reviews. 2012;(9). Art. No: CD007462. doi:10.1002/14651858.CD007462.pub2.
Conroy K, Koenig AF, Yu Y, Courtney A, Lee HJ, Norwitz ER. Delivery: 10 strategies to reduce risk. Rev Obstet Gynecol. 2012;5(2):69–77.
Lyimo FM, Massinde AN, Kidenya BR, Konje E, Mshana SE. Efficacy of single dose of gentamicin in combination with metronidazole versus multiple doses for prevention of post-caesarean infection: study protocol for a randomized controlled trial. Trials. 2012;13:89.
Amenu D, Belachew T, Araya F. Surgical site infection rate and risk factors among obstetric cases of jimma university specialized hospital, southwest ethiopia. Ethiop J Health Sci. 2011;21(2):91–100.
Brown J, Thompson M, Sinnya S, Jeffery A, de Costa C, Woods C, et al. Pre-incision antibiotic prophylaxis reduces the incidence of post-caesarean surgical site infection. J Hosp Infect. 2013;83(1):68–70.
Fehr J, Hatz C, Soka I, Kibatala P, Urassa H, Smith T, et al. Risk factors for surgical site infection in a Tanzanian district hospital: a challenge for the traditional National Nosocomial Infections Surveillance system index. Infect Control Hosp Epidemiol. 2006;27(12):1401–4.
Cardoso Del Monte MC, Pinto Neto AM. Postdischarge surveillance following cesarean section: the incidence of surgical site infection and associated factors. Am J Infect Control. 2010;38(6):467–72.
Aiken AM, Wanyoro AK, Mwangi J, Mulingwa P, Wanjohi J, Njoroge J, et al. Evaluation of surveillance for surgical site infections in Thika hospital. Kenya J Hosp Infect. 2013;83(2):140–5.
Petherick ES, Dalton JE, Moore PJ, Cullum N. Methods for identifying surgical wound infection after discharge from hospital: A systematic review. BMC Infect Dis. 2006;6:170.
Halwani MA, Turnbull AE, Harris M, Witter F, Perl TM. Postdischarge surveillance for infection following cesarean section: a prospective cohort study comparing methodologies. Am J Infect Control. 2016:455–7.
Koek MB, Wille JC, Isken MR, Voss A, Van Benthem BH. Post-discharge surveillance ( PDS ) for surgical site infections : a good method is more important than a long duration. 2015;
Ng W, Brown A, Alexander D, Ho MF, Kerr B, Amato M, et al. A multifaceted prevention program to reduce infection after cesarean section: interventions assessed using an intensive postdischarge surveillance system. Am J Infect Control. 2015;43(8):805–9.
Staszewicz W, Eisenring M-C, Bettschart V, Harbarth S, Troillet N. Thirteen years of surgical site infection surveillance in Swiss hospitals. J Hosp Infect. 2014;88(1):40–7.
Leonne J, Almeida D De, Cristina H, Souza D, Clemente WT, Maia R, et al. American journal of infection control surveillance of surgical site infection after cesarean section and time of notification. AJIC Am J Infect Control 2016;44(3):273–277.
Petrosillo N, Drapeau CMJ, Nicastri E, Martini L, Ippolito G, Moro ML. Surgical site infections in Italian hospitals: a prospective multicenter study. BMC Infect Dis. 2008;8:34.
Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36(5):309–32.
Srun S, Sinath Y, Seng AT, Chea M, Borin M, Nhem S, et al. Surveillance of post-caesarean surgical site infections in a hospital with limited resources. Cambodia J Infect Dev Ctries. 2013;7(8):579–85.
Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection. Infect Control Hosp Epidemiol. 1999;20(4):247–78.
Eriksen HM, Chugulu S, Kondo S, Lingaas E. Surgical-site infections at Kilimanjaro Christian medical center. J Hosp Infect. 2003;55(1):14–20.
De Nardo P, Gentilotti E, Nguhuni B, Vairo F, Chaula Z, Nicastri E, et al. Post-caesarean section surgical site infections at a Tanzanian tertiary hospital: a prospective observational study. J Hosp Infect. 2016;93(4):355–9.
Wloch C, Wilson J, Lamagni T, Harrington P, Charlett A, Sheridan E. Risk factors for surgical site infection following caesarean section in England: results from a multicentre cohort study. BJOG. 2012;119(11):1324–33.
Farret TCF, Dallé J, da Silva MV, Riche CVW, Antonello VS. Risk factors for surgical site infection following cesarean section in a Brazilian Women’s hospital: a case–control study. Brazilian J Infect Dis. 2015;19(2):113–7.
Acknowledgements
We thank all the patients who participated in the study and the staff working at the Obstetrics and Gynaecology Department of the Dodoma Regional Referral Hospital and post-natal care of the Makole Health Centre.
Funding
This survey was supported by grants from the Italian Development Cooperation - Ministry of Foreign Affairs AID9562 and ‘Ricerca Corrente’ of the Italian Ministry of Health.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Authors’ contributions
AMA, PDN, BN, and EG designed the study. BN performed the phone calls. Patients were clinically reviewed by PDN, EG, CD, and PM. FV and AF performed the statistical analysis. EN, ZC, AP were involved in drafting the manuscript and reviewing the literature. GI revised the final paper. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
This study was approved by the Hospital Management of DRRH, Tanzanian National Institute for Medical Research and the London School of Hygiene and Tropical Medicine. All women participating in the study read and signed an informed consent form.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Nguhuni, B., De Nardo, P., Gentilotti, E. et al. Reliability and validity of using telephone calls for post-discharge surveillance of surgical site infection following caesarean section at a tertiary hospital in Tanzania. Antimicrob Resist Infect Control 6, 43 (2017). https://doi.org/10.1186/s13756-017-0205-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13756-017-0205-0