
Abstract
Background
In the long term, smoking cessation can decrease the risk of cancer, stroke, and heart attacks and improve overall survival. The aim of the proposed umbrella review is to summarize existing systematic reviews that assessed the effects of pharmacological interventions for smoking cessation and to evaluate the methodological quality of previously conducted systematic reviews.
Methods
Databases such as the Cochrane Library, PubMed, MEDLINE, EMBASE, CINAHIL PsychINFO Web of Science, Conference Papers Index, Scopus, and Google Scholar will be used to retrieve reviews. Systematic reviews which included only randomized control trials will be considered in this review. The primary outcome will be prolonged abstinence from smoking for a minimum of 6 months follow-up, and the secondary outcome will be point abstinence rate from smoking of less than 6 months follow-up but more than 7 days. Methodological quality of the included reviews will be assessed using the Assessment of Multiple Systematic Reviews 2 (AMSTAR 2) tool, which contains 16 domains. Two authors will screen the titles and abstracts of all reviews obtained by the search strategy, assess the full text of selected articles for inclusion, and extract data independently. The quality appraisal will be also assessed by two authors (AM, CC) independently, and Cohen’s Kappa statistic will be used to assess inter-ratter agreement. The findings of the study will be narrated qualitatively to describe the effect of different pharmacotherapy on smoking cessation.
Discussion
The World Health Organization recommends treatment of tobacco dependence as one approach in its comprehensive tobacco control policy. To date, many trials and systematic reviews have been conducted to assess the effectiveness of pharmacotherapy for smoking cessation. Therefore, the findings of the umbrella review will improve clinical decision-making and be used as a baseline for future studies.
Systematic review registration
PROSPERO CRD42017080906
Similar content being viewed by others


Background
Globally, in 2012, the prevalence of daily tobacco smoking among men and women aged 15 and over was 31.1% and 6.2%, respectively [1]. Smoking seriously affects almost all organs in the body. Tobacco smoking can lead to many short- and long-term health effects including lung and other organ cancers, chronic bronchitis, emphysema, stroke, and heart attack [2]. Tobacco smoking is responsible for 90% of all cases of lung cancer and 90% of all deaths due to chronic obstructive pulmonary disease (COPD) [3]. According to the World Health Organization, tobacco smoking kills about six million people globally per annum [4]. Second-hand smoke contains hundreds of chemicals responsible for diseases such as respiratory disorders, cancer, and cardiovascular disease. Combustible chemicals found in tobacco smoke are responsible for disorders such as cancer, cardiovascular, and pulmonary diseases, through mechanisms that involve DNA damage, inflammation, and oxidative stress [5]. Globally, second-hand smoking affects women and children more than men [6, 7]. Tobacco-related disability-adjusted life years (DALYs) account for 4% of the global burden with the burden significantly higher for developed nations [8].
Tobacco contains about 4000 chemicals; nicotine is one of the chemicals contained in tobacco, and it is responsible for addictive behavior [9]. During smoking, the nicotine components are absorbed through the mucous membrane and enter the brain through the bloodstream. Upon entering the brain, nicotine stimulates the release of epinephrine and dopamine which in turn increases blood pressure, heartbeat, and respiration rate and produces pleasurable feelings [3, 9].
In the long term, smoking cessation can decrease the risk of cancer, stroke, and heart attacks and can also improve survival [3, 10]. Smoking cessation can also decrease the risk of respiratory infections such as pneumonia, influenza, and chronic obstructive pulmonary disease. [11]. Kahler et al. and Eddy et al. have shown that quitting smoking is associated with significant reductions in risk of COPD, myocardial infarctions, stroke, and coronary heart disease [12, 13]. Moreover, smoking cessation can improve health-related quality of life (physical, psychological, and social functioning in relation to health) [14].
A range of smoking cessation interventions is available which can be broadly categorized as motivational, behavioral/psychological, and pharmacological. The World Health Organization recommends that countries prioritize different smoking cessation strategies depending on their available resources, national health system, and political will to implement the cessation strategies [15]. Treatment of tobacco smoking, like any other forms of substance dependence, necessitates pharmacological interventions to minimize cravings and the treatment of withdrawal symptoms associated with nicotine dependence [9]. Nicotine replacement therapies (NRT) in different formulations such as inhalation, patches, gums, nasal sprays, and lozenges can be used for treatment of withdrawal symptoms after smoking cessation. Since the nicotine concentration in NRT is low compared to tobacco, it has a low addiction rate [3].
Amfebutamone (bupropion) represents the first non-nicotine drug used for the treatment of nicotine dependence. Amfebutamone works by antagonizing nicotine receptors and inhibits the reuptake of epinephrine, dopamine, and serotonin, thus reducing withdrawal symptoms [16,17,18]. Varenicline is a nicotine receptor partial agonist that blocks nicotine receptors by binding into α4β2 nicotinic acetylcholine receptors and moderately releases dopamine, thus reducing the craving and withdrawal symptoms associated with an absence of nicotine [19].
The success of smoking cessation was associated with factors such as male gender, smoking frequency, alcohol dependence, a household ban on smoking, living with a smoker, and having close friends who smoke [20, 21]. The most common adverse effects of NRT include insomnia, headache, vomiting, dizziness, palpitation, anxiety, and depression. Bupropion and varenicline are also associated with side effects like insomnia, dry mouth, agitation, and nausea [22, 23]. A systematic review identified a positive relationship between weight gain and smoking cessation [24]. Researchers have recommended the importance of weight management interventions along with smoking cessation interventions [25]. There are enzymes produced as a result of cigarette smoking responsible for the metabolism of drugs like clozapine. Therefore, smoking cessation can lead to a toxic side effect as a result of an increase in drug plasma concentration and requires monitoring and reduction in the dose of drugs [26].
Although most of the previous trials and systematic reviews confirmed the effectiveness of behavioral interventions [27, 28] for smoking cessation, the findings are not consistent for pharmacological interventions. Therefore, the proposed umbrella review will provide a summary of the evidence on the effectiveness of different types of pharmacotherapy. To date, many trials and systematic reviews have been conducted to assess the effectiveness of pharmacotherapy for smoking cessation. The proposed umbrella review of existing systematic reviews will present evidence from previous systematic reviews to help inform decision-makers and clinicians.
Objectives
The proposed umbrella review will synthesize findings of previous reviews in order to evaluate the effects of different pharmacotherapies for smoking cessation and assess consistency of conclusions among previous systematic reviews. The proposed umbrella review will summarize the effects of pharmacological interventions reported by each review of smoking cessation, specifically addressing the following objectives:
-
To summarizing existing systematic reviews that assessed the effects of pharmacological interventions for smoking cessation
-
To assess the methodological quality of previously conducted systematic reviews
Methods
Protocol registration and reporting of findings
The protocol of this review followed the guidelines of Preferred Reporting Items for Systematic Review and Meta-analysis Protocols (PRISMA-P) [29]. The PRISMA-P checklist is available as Additional file 1. The protocol was registered in PROSPERO with registration numberCRD42017080906:http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42017080906. The findings of the review will be reported in accordance with the recommendation of Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) [30]. If we intend to modify this protocol, we will give the date of each amendment, describe the change, and give the reason for the change.
Inclusion and exclusion criteria
Since the primary aim of the proposed umbrella review is to identify the effects of pharmacological interventions on smoking cessation, only reviews that included randomized control trials will be reviewed. Since tobacco cessation interventions are mostly targeted at adults aged 15 and over, in the proposed umbrella review, we will include studies of young people and adults aged 15 and over who were smokers. In the proposed umbrella review, we will consider only systematic reviews/systematic reviews with network meta-analysis that include primary studies with randomized control trial designed to assess the effect of pharmacotherapy for smoking cessation. Systematic reviews published 10 years before the last date of review will be included in the proposed review. The umbrella review will include only reviews for which full text is available. The primary outcome will be prolonged abstinence from smoking for a minimum of 6 months follow-up, and the secondary outcome will be point abstinence rate from smoking of less than 6 months follow-up but more than 7 days. We will prefer biochemical methods over self-reported verification. The control or comparison groups used will be either placebo, behavioral interventions, or pharmacotherapy. The review will include only those reviews which report pooled effects of the included studies through meta-analysis or network meta-analysis.
The umbrella review will include only studies published in English. If a review is an update of a previous review, the latest updates will be considered and the oldest versions will be excluded. Reviews which assessed combined pharmacotherapy and behavioral interventions will be excluded unless the reviews report the effect of pharmacotherapy separately, in which case, these reviews will be included. The summary of inclusion criteria based on population, intervention, comparator, outcome, and study design (PICOS) is presented in Table 1.
Information source and search strategy
To trace related reviews, databases such as the Cochrane Library, PubMed, MEDLINE, EMBASE, CINAHIL, and PsychINFO will be searched. Moreover, Web of Science, Conference Papers Index, Scopus, and Google Scholar will be used. Additional reviews will be sought using the reference lists of the retrieved articles. Additional articles will be traced from daily email alerts from MEDLINE database throughout the review process. The search strategy will be developed in consultation with a senior librarian. Different keywords/search terms will be used to access reviews from the database including “smoking cessation,” “smoking abstinence,” “Pharmacotherapy,” “Nicotine replacement therapy (NRT),” “bupropion,” “Varenicline,” “combination therapy,” “non-nicotine drug,” “nicotine receptor partial agonist,” “meta-analysis,” and “Systematic review.” The search strategy for MEDLINE is found in Additional file 2.
Data collection processes
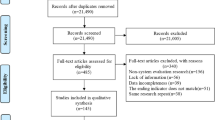
First, irrelevant studies not fulfilling the inclusion criteria for the systematic review will be excluded by reading the title and then by reading the abstract of the articles. Next, the full articles will be accessed and those articles which do not fit the objective of the review will be omitted. The excluded studies will be recorded along with the reason for exclusion at each stage. If additional information is required, the primary author of the published paper will be contacted. Cochrane data abstraction format will be used to extract information from the studies. Two authors (AM, CC) will carry out the following processes independently: screen the titles and abstracts of all publications obtained by the search strategy and assess the full text of selected articles for against inclusion criteria. Any discrepancy that arises between the two authors will be resolved through discussion. In case the authors not able to reach agreement, a third author will be consulted for assistance (LH). Cochrane data abstraction form will be used to extract data on the objectives of the study, study design, study inclusion and exclusion criteria, the number of articles and participants included, participant characteristics, intervention, control, outcome and pooled effects among others. The data extraction form is found in Additional file 3.
Assessment of methodological quality
Methodological quality of the included reviews will be assessed using the Assessment of Multiple Systematic Reviews 2 (an update of AMSTAR) tool, which contains 16 domains [31]. The tool includes 10 items from the original AMSTAR tool. Two items were created by splitting a single item from the original AMSTAR tool [32]. In total, four domains were added in AMSTAR 2 which were not found in the original tool. The response option for most domains consists of “yes” and “no” while some domains contain the third option “partial yes.” AMSTAR has been shown to have good inter-rater reliability to assess the quality of systematic reviews. From the 16 AMSTAR tool items, 7 were critical domains upon which the quality rating of individual systematic reviews depends (Table 2). Based on the overall score, the quality of each systematic review will be rated as high, moderate, low, and critically low. Table 2 presents the criteria to rate the quality of systematic review. The AMSTAR 2 checklist is found in Additional file 4. Scores for each item will be reported separately for each systematic review. The quality assessment of the included systematic review will be conducted by two independent reviewers (AM, CC), and any disagreement between the two reviewers will be resolved with discussion. In case the authors not able to reach agreement, a third author will be consulted for assistance (LH). Cohen’s Kappa statistic will be used to assess inter-rater agreement. A Kappa value below 60% indicates inadequate agreement among the raters [33]. Studies will not be excluded based on their quality, but the assessment serves to judge the strength of evidence generated by the included studies.
Data synthesis
In this review, a meta-analysis will not be conducted because data from individual studies are likely to be represented more than once across the systematic reviews, and this will likely lead to over or underestimations of the true effect size [34]. The required information will be collected using a pretested checklist adopted from the Cochrane data abstraction format, according to the objective of the review [35]. Narrative synthesis method will be employed to show the effects of different pharmacotherapies on smoking cessation. The Narrative presentation will include the overall effect size reported by systematic review authors along with statistical heterogeneity and methodological quality. Evidence will be summarized in a table which will present the types of intervention, comparators, outcome measures, number of participants, number of included primary studies, and pooled results from each review, heterogeneity, and the review author’s conclusions. To calculate the degree of overlap, we will calculate corrected covered area (CCA) by dividing the frequency of repeated occurrence of index publication in other reviews by the product of index publications and reviews less the number of index publications. The CCA will be rated as follows: CCA less than 5 will be rated as slight overlap, 6–10 moderate overlap, 11–15 high overlap, and greater than 15 as a very high overlap [36]. The degree of overlap will be stated as a limitation while interpreting the findings.
Assessing confidence in evidence
The quality of evidence reported by the systematic review authors will be reported for primary studies. If the systematic reviews fail to report the quality of evidence, we will assess the risk of bias using Grading of Recommendations Assessment, Development and Evaluation (GRADE) measures.
Discussion
Systematic reviews are considered as an important source of information for clinicians and policy makers because combining the findings from a series of studies can provide a more accurate and reliable evidence base through improved statistical power. Moreover, systematic reviews are an important tool for the development of guidelines and strategies for medical practice and suggesting directions for new research [37, 38]. Clinicians and decision-makers need to assure themselves that the basic approaches and methods used to collect and combine the findings of individual studies are relevant and sound before using the evidence for patient care and policy development [38, 39]. Review of systematic reviews help as a method to providing a higher level combination of evidence to wide public health problems [40].
The World Health Organization recommends including treatment of tobacco dependence as one strategy of its comprehensive tobacco-control policy, along with measures such as taxation and price policies, advertising restrictions, dissemination of information, and establishment of smoke-free public places [15]. Therefore, in the proposed review of reviews, we will be summarizing existing systematic reviews that assessed the effects of pharmacological interventions for smoking cessation and also conduct methodological quality of the included reviews. The findings of our review will improve clinical decision-making and will be used as a baseline for future studies.
Abbreviations
- AMSTAR:
-
Assessment of Multiple Systematic Reviews
- COPD:
-
Chronic obstructive pulmonary disease
- NRT:
-
Nicotine replacement therapy
- PRISMA:
-
Preferred Reporting Items for Systematic Review and Meta-analysis
- PROSPERO:
-
International prospective register of systematic reviews
- R-AMSTAR:
-
Revised Assessment of Multiple Systematic Reviews
References
Ng M, Freeman MK, Fleming TD, Robinson M, Dwyer-Lindgren L, Thomson B, et al. Smoking prevalence and cigarette consumption in 187 countries, 1980–2012. Jama. 2014;311(2):183–92 https://doi.org/10.1001/jama.2013.284692.
National Institute on Drug Abuse. Cigarettes and other tobacco products. 2017. https://www.drugabuse.gov/publications/drugfacts/cigarettes-other-tobacco-products. Accessed 9 Jan 2017.
US Department of Health and Human service. Are there effective treatments for tobacco addiction? National Institute of Health; 2016.
World Health Organization. WHO global report on trends in prevalence of tobacco smoking 2015: World Health Organization; 2015. http://apps.who.int/iris/bitstream/10665/156262/1/9789241564922_eng.pdf. Accessed 18 Jan 2017.
Office of the Surgeon General. How tobacco smoke causes disease: the biology and behavioural basis for smoking-attributable disease. Washington DC: US Department of Health and Human Services; 2010. https://www.ncbi.nlm.nih.gov/books/NBK53017/. Accessed 8 Jan 2017.
US Department of Health and Human Services. The health consequences of involuntary exposure to tobacco smoke: a report of the Surgeon General; 2006. https://www.barnesandnoble.com/w/the-health-consequences-of-involuntary-exposure-to-tobacco-smoke-department-of-human-services/1112109451. Accessed 12 Feb 2018.
Öberg M, Jaakkola MS, Woodward A, Peruga A, Prüss-Ustün A. Worldwide burden of disease from exposure to second-hand smoke: a retrospective analysis of data from 192 countries. The Lancet. 2011;377(9760):139–46 https://doi.org/10.1016/S0140-6736(10)61388-8.
Rehm J, Rehm J, Taylor B, Rehm J, Taylor B, Room R, et al. Global burden of disease from alcohol, illicit drugs and tobacco. Drug and alcohol review. 2006;25(6):503–13 https://doi.org/10.1080/09595230600944453.
Jiloha R. Pharmacotherapy of smoking cessation. Indian journal of psychiatry. 2014;56(1):87 https://doi.org/10.4103/0019-5545.124726.
Taylor DH Jr, Hasselblad V, Henley SJ, Thun MJ, Sloan FA. Benefits of smoking cessation for longevity. American journal of public health. 2002;92(6):990–6 https://doi.org/10.2105/AJPH.92.6.990.
U.S. Department of Health and Human Services. Reducing Tobacco Use: A Report of the Surgeon General.Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2000. https://www.cdc.gov/tobacco/data_statistics/sgr/2000/complete_report/pdfs/fullreport.pdf. Accessed 12 Dec 2017.
Kahler CW, Spillane NS, Metrik J, Leventhal AM, Monti PM. Sensation seeking as a predictor of treatment compliance and smoking cessation treatment outcomes in heavy social drinkers. Pharmacology Biochemistry and Behavior. 2009;93(3):285–90 https://doi.org/10.1016/j.pbb.2009.01.003.
Eddy DM, Peskin B, Shcheprov A, Pawlson G, Shih S, Schaaf D. Effect of smoking cessation advice on cardiovascular disease. American Journal of Medical Quality. 2009;24(3):241–9 https://doi.org/10.1177/1062860609332509.
Tomioka H, Sekiya R, Nishio C, Ishimoto G. Impact of smoking cessation therapy on health-related quality of life. BMJ open respiratory research. 2014;1(1):e000047 https://doi.org/10.1136/bmjresp-2014-000047.
Costa e Silva Vd. Tools for advancing tobacco control in the XXIst century: policy recommendations for smoking cessation and treatment of tobacco dependence: tools for public health: World Health Organization; 2003. http://www.who.int/tobacco/resources/publications/en/intro_chapter3.pdf. Accessed 9 June 2018.
Damaj MI, Slemmer J, Carroll F, Martin B. Pharmacological characterization of nicotine’s interaction with cocaine and cocaine analogs. Journal of Pharmacology and Experimental Therapeutics. 1999;289(3):1229–36. http://jpet.aspetjournals.org/content/jpet/289/3/1229.full.pdf.
Covey LS, Sullivan MA, Johnston JA, Glassman AH, Robinson MD, Adams DP. Advances in non-nicotine pharmacotherapy for smoking cessation. Drugs. 2000;59(1):17–31 https://doi.org/10.2165/00003495-200059010-00003.
Roddy E. ABC of smoking cessation: bupropion and other non-nicotine pharmacotherapies. BMJ: British Medical Journal. 2004;328(7438):509 https://doi.org/10.1136/bmj.328.7438.509.
Mihalak KB, Carroll FI, Luetje CW. Varenicline is a partial agonist at α4β2 and a full agonist at α7 neuronal nicotinic receptors. Molecular pharmacology. 2006;70(3):801–5 https://doi.org/10.1124/mol.106.025130.
Ayo-Yusuf OA, Szymanski B. Factors associated with smoking cessation in South Africa. South African Medical Journal. http://www.samj.org.za/index.php/samj/article/view/3842/2714.
Klein EG, Forster JL, Erickson DJ. Longitudinal predictors of stopping smoking in young adulthood. Journal of Adolescent Health. 2013;53(3):363–7 https://doi.org/10.1016/j.jadohealth.2013.04.012.
Hays JT, Ebbert JO. Adverse effects and tolerability of medications for the treatment of tobacco use and dependence. Drugs. 2010;70(18):2357–72 https://doi.org/10.2165/11538190-000000000-00000.
Dhippayom T, Chaiyakunapruk N, Jongchansittho T. Safety of nortriptyline at equivalent therapeutic doses for smoking cessation: a systematic review and meta-analysis. Drug safety. 2011;34(3):199–210 https://doi.org/10.2165/11585950-000000000-00000.
Tian J, Venn A, Otahal P, Gall S. The association between quitting smoking and weight gain: a systemic review and meta-analysis of prospective cohort studies. Obes Rev. 2015;16(10):883–901 https://doi.org/10.1111/obr.12448.
Dare S, Mackay DF, Pell JP. Relationship between smoking and obesity: a cross-sectional study of 499,504 middle-aged adults in the UK general population. PloS one. 2015;10(4):e0123579 https://doi.org/10.1371/journal.pone.0123579.
Lowe EJ, Ackman ML. Impact of tobacco smoking cessation on stable clozapine or olanzapine treatment. Annals of Pharmacotherapy. 2010;44(4):727–32 https://doi.org/10.1345/aph.1M398.
Mottillo S, Filion KB, Belisle P, Joseph L, Gervais A, O'Loughlin J, et al. Behavioural interventions for smoking cessation: a meta-analysis of randomized controlled trials. European heart journal. 2008;30(6):718–30 https://doi.org/10.1093/eurheartj/ehn552.
Lancaster T, Stead LF. Individual behavioural counselling for smoking cessation. Cochrane database of systematic reviews. 2017;3:CD001292 https://doi.org/10.1002/14651858.CD001292.pub3.
Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ (Clinical research ed). 2015;349:g7647 https://doi.org/10.1136/bmj.g7647.
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS med. 2009;6(7):e1000097 https://doi.org/10.1371/journal.pmed.1000097.
Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. bmj. 2017;358:j4008 https://doi.org/10.1136/bmj.j4008.
Shea BJ, Grimshaw JM, Wells GA, Boers M, Andersson N, Hamel C, et al. Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC medical research methodology. 2007;7(1):10 https://doi.org/10.1186/1471-2288-7-10.
McHugh ML. Interrater reliability: the kappa statistic. Biochemia medica. 2012;22(3):276–82. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3900052/.
Aromataris E, Fernandez R, Godfrey CM, Holly C, Khalil H, Tungpunkom P. Summarizing systematic reviews: methodological development, conduct and reporting of an umbrella review approach. International journal of evidence-based healthcare. 2015;13(3):132–40 https://doi.org/10.1097/XEB.0000000000000055.
Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration; 2011. Available from http://handbook.cochrane.org.
Pieper D, Antoine S-L, Mathes T, Neugebauer EA, Eikermann M. Systematic review finds overlapping reviews were not mentioned in every other overview. Journal of clinical epidemiology. 2014;67(4):368–75 https://doi.org/10.1016/j.jclinepi.2013.11.007.
Abbas Z, Raza S, Ejaz K. Systematic reviews and their role in evidence--informed health care. JPMA The Journal of the Pakistan Medical Association. 2008;58(10):561. http://jpma.org.pk/PdfDownload/1514.pdf.
Garg AX, Hackam D, Tonelli M. Systematic review and meta-analysis: when one study is just not enough. Clinical Journal of the American Society of Nephrology. 2008;3(1):253–60 https://doi.org/10.2215/CJN.01430307.
Pieper D, Buechter RB, Li L, Prediger B, Eikermann M. Systematic review found AMSTAR, but not R (evised)-AMSTAR. to have good measurement properties. Journal of clinical epidemiology. 2015;68(5):574–83 https://doi.org/10.1016/j.jclinepi.2014.12.009.
Baker PR, Costello JT, Dobbins M, Waters EB. The benefits and challenges of conducting an overview of systematic reviews in public health: a focus on physical activity. Journal of Public Health. 2014;36(3):517–21 https://doi.org/10.1093/pubmed/fdu050.
Acknowledgements
We would like to acknowledge the senior librarian at the University of Newcastle, Debbie Booth for the assistance in developing the search strategy.
Funding
This protocol had no funding source. The principal author received a scholarship from The University of Newcastle, Australia, to undertake his PhD study.
Availability of data and materials
Not applicable
Author information
Authors and Affiliations
Contributions
AS is the guarantor and developed the review protocol. CC, EH, and DL critically reviewed the protocol. All authors read and approved the final submission of the paper.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
PRISMA-P checklist (DOCX 66 kb)
Additional file 2:
Search strategy in Medline (DOCX 19 kb)
Additional file 3:
Data abstraction form (DOCX 23 kb)
Additional file 4:
Quality assessment tool (AMSTRA 2) (PDF 173 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Melka, A.S., Chojenta, C.L., Holliday, E.G. et al. Effectiveness of pharmacotherapy for smoking cessation: protocol for umbrella review and quality assessment of systematic reviews. Syst Rev 7, 210 (2018). https://doi.org/10.1186/s13643-018-0878-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-018-0878-3