
Abstract
Background
Head and neck cancers include malignancies of the mouth, larynx and oropharynx. Tobacco use and alcohol consumption are associated with increased risks of developing and dying from head and neck cancer. The aim of this review is to examine the effectiveness of smoking and alcohol cessation interventions on disease-related outcomes, quality of life and behavioural change in adults with head and neck cancer and oral dysplasia.
Methods
The Cochrane library, CINAHL, Embase, MEDLINE, PsycINFO and Web of Science databases will be searched for randomised controlled trials investigating the effects of smoking or alcohol interventions on patients with either head and neck cancer or oral dysplasia. The primary outcomes are disease-free survival and, for participants with oral dysplasia, malignant transformation to cancer. Secondary outcomes are disease recurrence and progression, quality of life and behavioural change. The quality of included studies will be assessed using the ‘Cochrane Collaborations tool for assessing risk of bias’. A qualitative synthesis of the results will be reported, and a meta-analysis of the outcome data conducted, where appropriate.
Discussion
This systematic review will identify the extent of the current research on smoking and alcohol cessation interventions in patients with head and neck cancer and oral epithelial dysplasia. The findings have the potential to inform which interventions have been successful and how future behavioural change interventions should be conducted within these populations.
Systematic review registration
PROSPERO CRD42016038237
Similar content being viewed by others


Background
Head and neck cancers are a heterogeneous group of malignancies which include cancers of the mouth, sinus, larynx, nasopharynx and oropharynx. The most common type of head and neck cancer is squamous cell carcinoma of the mucosal surfaces of the mouth, nose and throat [1] which accounts for 90% of cancers of the head and neck [2]. It is estimated that 11,152 new cases were diagnosed in the UK in 2012 [3], with more than 550,000 cases diagnosed annually worldwide [4]. Incidence rates vary based on cancer site and while rates of oral cavity and oropharyngeal cancers have risen over recent years, the incidence of laryngeal cancer rates has declined which may be related to the reduction in smoking rates [5]. European relative survival rates for head and neck cancer patients are estimated at 72% at 1 year and 42% at 5 years [6]. Overall 5-year survival for head and neck cancer in the UK has been estimated at 45%; however, rates also vary by cancer site [7]. In England, between 2009 and 2013, 5-year survival rates were 65.6% in oropharyngeal cancer, 56.1% in oral cavity cancer and 27.8% in hypopharyngeal cancer [8].
Oral epithelial dysplasia is a potentially pre-malignant condition that can progress to squamous cell carcinoma. Reported rates of mutation to oral cancer vary based on the degree of dysplasia (16% for sever dysplasia to <5% for mild dysplasia) [9]. Leukoplakia and erythroplakia are two of the most common clinical presentations in which dysplasia is found and rates of dysplasia vary between these lesions [10]. It is estimated that 5% of people with leukoplakia have dysplasia or cancerous cells while up to 50% of people with erythroplakia will develop cancer [11].
Tobacco use, which can include both smoking and chewing tobacco, and alcohol consumption are estimated to account for approximately 75% of cancers of the oral cavity, pharynx and larynx [12, 13]. In a pooled analysis [12] of 15 case control studies of cigarette smoking amongst study participants who never drank alcohol, smoking was associated with an increased risk of head and neck cancer (OR for ever versus never smoking = 2.13, 95% CI = 1.52 to 2.98) and a dose-response relationship was observed for the frequency and duration of cigarette smoking. The pooled analysis also reported that at least three alcoholic drinks per day amongst study participants who never smoked was associated with a 2.04 increased risk of head and neck cancer (95% CI = 1.29 to 3.21).
Conversely, the risk factors for oral dysplasia are not well understood; although, there is also evidence of links to tobacco use and alcohol consumption [14, 15].
As well as increasing risk of disease, there is also evidence to suggest that smoking and alcohol use can influence treatment outcomes [16, 17]. Smokers may be less likely to respond to treatment if they smoke, resulting in a lower rate of survival [18], and are at greater risk of experiencing treatment side effects [19], while patients who continue to consume alcohol seem to have a higher risk of recurrence and second primary tumours [20, 21].
No previous systematic reviews on smoking or alcohol interventions in patients being treated for head and neck cancer or oral dysplasia were identified through an initial scope of the literature, highlighting a need for the synthesis of intervention data in this area.
Research objective
To examine the effectiveness of smoking and alcohol cessation interventions on disease-related outcomes, quality of life and behavioural change in adults with head and neck cancer and oral dysplasia.
Methods
This protocol has been reported in accordance with the “Preferred Reporting Items for Systematic review and Meta-Analysis Protocols (PRISMA-P) 2015 checklist” [22]. A populated checklist for this review protocol has been provided in Additional file 1.
Eligibility criteria
Study design
Randomised controlled trials will be included. Quasi-randomised trials, those where randomisation is done on the basis of a pseudo-randomised sequence [23], and observational studies will be excluded.
Participants
The participants include adult patients aged at least 18, diagnosed with either oral dysplasia or head and neck cancer. For the purpose of this review, head and neck cancers that will be included are cancers of the oral cavity, larynx, hypopharynx and oropharynx as these are associated with tobacco and alcohol use.
Intervention
Interventions that will be included in the review are as follows:
-
(a)
Tobacco use reduction or cessation interventions—including both psychosocial and pharmacological interventions.
-
(b)
Alcohol use reduction or cessation interventions—including both psychosocial and pharmacological interventions.
Trials that include a combination of these interventions will also be included.
Comparison
We will include placebo or standard care as the comparison group, depending on intervention type (pharmacological or behavioural). Studies that compare multiple active intervention arms but do not include a control arm will also be included.
Outcomes
Studies will be included in the data extraction if they report on one of the following primary or secondary outcomes.
Primary outcomes
-
1.
Disease-free survival: defined as the length of time following treatment that the participant lived without recurrence or relapse of the disease.
-
2.
Malignant transformation in participants with oral dysplasia: defined as the development of oral or laryngeal cancer.
Secondary outcomes
-
1.
Disease recurrence: defined as the return of the cancer to the same primary site following treatment.
-
2.
Disease progression in people with head and neck cancer: defined as the development or progression of lymph node metastasis, the development of distant metastasis or an increase in the size of the primary tumour.
-
3.
Quality of life measured by any standardised scale: For example, including but not limited to the European Organisation for Research and Treatment of Cancer scales (including the head and neck specific scale “QLQ-H&N35”), Functional Assessment of Chronic Illness Therapy Measurement Systems, Short Form Health survey—SF36/SF12.
-
4.
Adverse events related to the interventions. These could include but are not limited to nicotine/alcohol withdrawal related adverse events and adverse events related to nicotine replacement therapy.
-
5.
Behavioural change: defined as the proportion of participants who successfully altered the behaviour of interest, measured through either self-report or biomarker methods.
-
6.
Second primary cancers if they originated at least 3 cm away from the primary site and occurred at least 3 years after the last known recurrence
-
7.
Head and neck cancer specific mortality
-
8.
All-cause mortality
Search strategy
Electronic searches
Literature searches will be performed in the following databases for relevant published articles:
-
1.
Cochrane library (from inception to present)
-
2.
PsycINFO (from 1806 to present)
-
3.
CINAHL (from 1937 to present)
-
4.
Embase (from 1974 to present)
-
5.
MEDLINE (from 1946 to present)
-
6.
Web of Science (from 1900 to present)
An example of the search strategy for use in MEDLINE is shown in Additional file 2. The same search terms will be used for each database with any changes made to the syntax as per individual database requirements. The searches will not be limited by date range or language of publication. Searches performed in Web of Science will enable conference abstracts to be yielded.
Searching other resources
Any systematic reviews found will be used to identify further studies not found in the original search. The reference lists of all included articles will be hand searched for additional studies. The search will be complemented by contacting subject experts about any unpublished or published studies that were not yielded from the original search. The NIHR Clinical Trials gateway will also be searched to identify any trials currently taking place which have not yet reached publication stage [24] and the first 20 pages of google scholar will be hand searched for any additional articles.
Data management
Endnote reference management software will be used to manage the search results. Database search results will be imported into an Endnote library and duplicates removed during the data screening process. All references to the same study will be extracted and referred to in the text of the main report.
Selection of studies
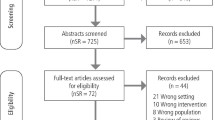
Studies for inclusion will be screened independently by two reviewers (ES, LR). Initial screening will be performed by both reviewers and compared to ensure accuracy. Any discrepancies found will be discussed with a third reviewer (RP) for resolution. Abstracts meeting the inclusion criteria will be retrieved in full for data extraction.
Data extraction
Data will be extracted by two reviewers independently, then compared for accuracy. Extraction will take place using a standardised template designed specifically for this review. This template will be piloted by both reviewers on the first five papers extracted, then discussed to ensure common use and to agree on any amendments required. Data will be extracted on the following:
-
a)
Publication information—paper title, author details, publication type, funding sources, year of study
-
b)
Sample characteristics—number of participants, demographics (age, sex, ethnicity), cancer site and staging, inclusion/exclusion criteria, sub groups included, withdrawals and exclusions
-
c)
Intervention type and design—study design, intervention description (including type, dose and duration), method of randomisation. Timing of the intervention (e.g. pre or post treatment) will also be extracted.
-
d)
Results—outcomes of interest reported (as defined in the methods section of this protocol), statistical methods used, summary statistics, means and standard deviations or medians and inter quartile ranges as appropriate, QOL scales used and resulting QOL scores, adverse events.
-
e)
Measures of methodological quality—detail provided below under assessment of risk of bias.
Any discrepancies found will be discussed with a third reviewer in order to finalise inclusion/exclusion.
Assessment of risk of bias
Risk of bias and overall methodological quality will be assessed by two reviewers independently using a table based on the Cochrane Collaboration’s tool for assessing risk of bias, which has been updated to reflect the current study’s review parameters [25]. A copy of the table of assessment criteria used for this study can be seen in Table 1. Studies will be classified as having a low, high or unclear risk of bias based on six criteria:
-
Sequence generation
-
Allocation concealment
-
Blinding of participants, personnel and outcome assessors (where practical and applicable)
-
Incomplete outcome data
-
Selective outcome reporting
-
Other potential threats to validity, e.g. differences in baseline characteristics between intervention groups and conflict of interest of researchers.
Dealing with missing data
Study authors will be approached for any missing or unreported data, as required. For the purposes of meta-analyses where missing data are still present, we will attempt to estimate these values from other results reported in the paper (e.g. if t values from t tests are reported but no standard deviations, we can calculate the standard deviations), or impute possible values using the largest values from those studies which did report the missing result (see “Sub-group and sensitivity analyses” for further details).
Data analysis
We will undertake a qualitative synthesis of all studies. Due to the diverse nature of the interventions of interest, we anticipate heterogeneity between studies and will therefore use random effects models to quantitatively synthesise all data relating to each combination of intervention type and outcome measure. For binary outcome measures (disease-free survival, progression and recurrence, cancer specific and all-cause mortality, and second primary cancers), we will pool risk ratios and will calculate or estimate risk ratios where possible from studies which do not report them. Where hazard ratios are reported, we will pool these separately and we will estimate hazard ratios from studies which report suitable outcome measures (e.g. median survival time for intervention and control arms). For continuous outcomes (quality of life), we will pool means and associated standard deviations and we will estimate mean and standard deviation values where possible (e.g. median quality of life for intervention and control arms). We will assess statistical heterogeneity by visually inspecting forest plots and with the chi-square measurement, with a cutoff of P < 0.01 for the chi-square measurement to indicate heterogeneity since it is difficult to assess when sample sizes are small. We will use the I 2 statistic to measure variation in the effect size due to heterogeneity, with values greater than 50% indicative of significant heterogeneity [19]. If the studies are considered too heterogeneous with regards to the intervention design or outcome measure used, we will not pool their effect sizes. We will test the likelihood of publication bias through visual inspection of funnel plots and using Egger’s regression test.
If a meta-analysis is undertaken, the strength of the body of evidence will be assessed using the GRADE system [23].
Interventions which include a behavioural change technique will also be coded for qualitative analysis using the BCT Taxonomy (v1) to allow for comparison of techniques employed for the intervention [26].
Sub-group and sensitivity analyses
Where possible, we will analyse intervention effects on primary and secondary outcomes within the following sub-groups: oral dysplasia compared with head and neck cancer and between tumour sites. To minimise the impact of studies at high risk of bias, we will exclude these and repeat our meta-analyses. Imputation of missing values using the largest reported value from other studies can potentially bias results towards a lack of effect [23], and therefore, as sensitivity analyses to explore the impact of this imputation method on our findings, we will repeat our meta-analyses with two modifications. Firstly, instead of replacing missing values with the largest reported values, we used the mean of the reported values. Secondly, studies which were missing data were excluded.
Discussion
Due to evidence from observational studies that suggests that those who reduce tobacco and alcohol consumption have better outcomes, lifestyle interventions aimed at cessation are of current interest. However, to our knowledge, no systematic review has been published to date that identifies the interventions tested or how successful they have been at improving clinical outcomes and quality of life. We anticipate that this review will therefore inform the design and conduct of further behavioural change interventions in this population group.
This systematic review will identify the extent of the current research on smoking and alcohol cessation interventions in patients with head and neck cancer and oral dysplasia. Through review of the current evidence, the findings will inform further research into interventions aimed at improving outcomes and quality of life in this patient group.
Abbreviations
- BCT:
-
Behavioural change technique
- GRADE:
-
Grading of Recommendations, Assessment, Development and Evaluation
- OED:
-
Oral epithelial dysplasia
- PA:
-
Physical activity
- QOL:
-
Quality of life
- RCT:
-
Randomised controlled trial
References
National Cancer Institute: Head and Neck Cancers http://www.cancer.gov/types/head-and-neck/head-neck-fact-sheet. Accessed 6 June 2016.
Macmillan: Types of Head and Neck Cancer http://www.macmillan.org.uk/cancerinformation/cancertypes/headneck/aboutheadneckcancers/typesofheadneckcancer.aspx. Accessed 6 June 2016.
Macmillan: People with Head and Neck Cancer http://www.macmillan.org.uk/documents/aboutus/research/richpictures/update/rp-people-with-head-and-neck-cancer.pdf. Accessed 6 June 2016.
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90.
Oxford Cancer Intelligence Unit (OCIU): Profile of Head and Neck Cancers in England: Incidence, Mortality and Survival. In: National Cancer Intelligence Network; 2010. http://www.ncin.org.uk/cancer_type_and_topic_specific_work/cancer_type_specific_work/head_and_neck_cancers/head_and_neck_cancer_hub/resources. Accessed 16 Mar 2016.
Grégoire V, Lefebvre J-L, Licitra L, Felip E, Group ObotEEEGW. Squamous cell carcinoma of the head and neck: EHNS–ESMO–ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010;21(suppl 5):v184–6.
Drugan C, Leary S, Mellor T, Bain C, Verne J, Ness A, Thomas S. Head and neck cancer in the south west of England, Hampshire, and the isle of Wight: trends in survival 1996–2008. Br J Oral Maxillofac Surg. 2013;51(1):19–24.
Cancer Research UK: Head and neck cancers survival statistics http://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/head-and-neck-cancers/survival#heading-Zero. Accessed 30 June 2017.
Speight PM. Update on oral epithelial dysplasia and progression to cancer. Head Neck Pathol. 2007;1(1):61–6.
Yardimci G, Kutlubay Z, Engin B, Tuzun Y. Precancerous lesions of oral mucosa. World J Clin Cases. 2014;2(12):866–72.
Cancer Research UK (CRUK): Types of mouth and oropharyngeal cancer http://www.cancerresearchuk.org/about-cancer/type/mouth-cancer/about/types-of-mouth-and-oropharyngeal-cancer#pre. Accessed 18 Mar 2016.
Hashibe M, Brennan P, Benhamou S, Castellsague X, Chen C, Curado MP, Maso LD, Daudt AW, Fabianova E, Wünsch-Filho V, et al. Alcohol drinking in never users of tobacco, cigarette smoking in never drinkers, and the risk of head and neck cancer: pooled analysis in the international head and neck cancer epidemiology consortium. J Natl Cancer Inst. 2007;99(10):777–89.
Macmillan: Risk factors and causes of head and neck cancer http://www.macmillan.org.uk/cancerinformation/cancertypes/headneck/aboutheadneckcancers/causes.aspx. Accessed 14 Apr 2016.
Jaber MA, Porter SR, Gilthorpe MS, Bedi R, Scully C. Risk factors for oral epithelial dysplasia—the role of smoking and alcohol. Oral Oncol. 1999;35(2):151–6.
Morse DE, Pendrys DG, Katz RV, Holford TR, Krutchkoff DJ, Eisenberg E, Kosis DL, Kerpel S, Freedman P, Mayne ST. Food group intake and the risk of oral epithelial dysplasia in a United States population. Cancer Causes Control. 11(8):713–20.
Duffy SA, Ronis DL, Valenstein M, Lambert MT, Fowler KE, Gregory L, Bishop C, Myers LL, Blow FC, Terrell JE. A tailored smoking, alcohol, and depression intervention for head and neck cancer patients. Cancer Epidemiol Biomark Prev. 2006;15(11):2203–8.
Dikshit RP, Boffetta P, Bouchardy C, Merletti F, Crosignani P, Cuchi T, Ardanaz E, Brennan P. Lifestyle habits as prognostic factors in survival of laryngeal and hypopharyngeal cancer: a multicentric European study. Int J Cancer. 2005;117(6):992–5.
Browman GP, Wong G, Hodson I, Sathya J, Russell R, McAlpine L, Skingley P, Levine MN. Influence of cigarette smoking on the efficacy of radiation therapy in head and neck cancer. N Engl J Med. 1993;328(3):159–63.
Zevallos JP, Mallen MJ, Lam CY, Karam-Hage M, Blalock J, Wetter DW, Garden AS, Sturgis EM, Cinciripini PM. Complications of radiotherapy in laryngopharyngeal cancer. Cancer. 2009;115(19):4636–44.
Rosenquist K, Wennerberg J, Annertz K, Schildt E-B, Göran Hansson B, Bladström A, Andersson G. Recurrence in patients with oral and oropharyngeal squamous cell carcinoma: human papillomavirus and other risk factors. Acta Otolaryngol. 2007;127(9):980–7.
Mayne ST, Cartmel B, Kirsh V, Goodwin WJ. Alcohol and tobacco use prediagnosis and postdiagnosis, and survival in a cohort of patients with early stage cancers of the oral cavity, pharynx, and larynx. Cancer Epidemiol Biomark Prev. 2009;18(12):3368–74.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339
Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, Savović J, Schulz KF, Weeks L, Sterne JAC. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343
NIHR: UK Clinical Trials Gateway https://www.ukctg.nihr.ac.uk. Accessed 28 Apr 2016.
Higgins J: Assessing risk of bias in included studies. In: Cochrane Handbook for Systematic Reviews Version 5.1.0 edn.: The Cochrane Collaboration; 2011. http://handbook.cochrane.org. Accessed 3 Aug 2017.
Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, Eccles MP, Cane J, Wood CE. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. 2013;46(1):81–95.
Acknowledgements
The authors would like to thank Cath Borwick, Information Specialist, for her contribution to the search strategy.
Funding
This systematic review is funded by the National Institute for Health Research (NIHR) Bristol Nutritional Biomedical Research Unit based at University Hospitals Bristol NHS Foundation Trust and the University of Bristol. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health. RMM is a recipient of a Cancer Research UK Programme Grant—the Integrative Cancer Epidemiology Programme (C18281/A19169).
Availability of data and materials
Not applicable—protocol manuscript only, no supporting data available.
Author information
Authors and Affiliations
Contributions
ES and LR are responsible for the design, article reviewing and manuscript writing. RP did the design of the search strategy, provided methodological advice on systematic reviews and contributed to the article reviewing and critical revision of the manuscript. CP provided methodological advice on the meta-analysis and critically revised the manuscript. RMM, ST, JAL and AN contributed to the conception, article reviewing and critical revision of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable—no individual person’s data has been included in this manuscript.
Consent for publication
Not applicable—no individual person’s data has been included in this manuscript.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
PRISMA-p checklist for the reporting of the protocol. (DOC 82 kb)
Additional file 2:
An example of the search terms used in MEDLINE. (DOCX 17 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Shingler, E., Robles, L.A., Perry, R. et al. Tobacco and alcohol cessation or reduction interventions in people with oral dysplasia and head and neck cancer: systematic review protocol. Syst Rev 6, 161 (2017). https://doi.org/10.1186/s13643-017-0555-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13643-017-0555-y