
Abstract
We observed a male newborn with bilateral nystagmus and central hypothyroidism without hypoprolactinemia due to a deletion of chromosome band Xq26.1q26.2, containing FRMD7 and IGSF1. These two loss-of function mutations are known to cause, respectively, congenital nystagmus and the ensemble of central hypothyroidism, hypoprolactinemia and testicular enlargement. These latter two features may not yet be present in early life.
Similar content being viewed by others


Letter to the editor
In 1969, Schulman and Crawford reported a boy with congenital nystagmus and central hypothyroidism (“congenital, isolated TSH deficiency”) – an apparently rare and still unexplained association [1].
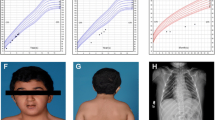
Recently, we observed a male newborn with bilateral nystagmus and central hypothyroidism. At term birth, he presented with an umbilical hernia, enlarged tongue and need for additional oxygen. On day 3, serum free T4 was only 0.52 ng/dL (normally ≥2.0 ng/dL), TSH elevation was limited (10.6 mU/L); L-thyroxine treatment was initiated.
Early gestation had been complicated by nuchal enlargement, which prompted a chorion biopsy that led to the identification of a 1.29 Mb deletion of chromosome band Xq26.1q26.2 [arr Xq26.1q26.2(129928356–131292675)x0]. The deleted region contains – besides five genes so far unassociated with disease (ENOX2, ARHGA36, OR13H1, FIRRE, MST4) – FRMD7 and IGSF1, loss-of-function mutations in which are known to cause, respectively, congenital nystagmus [2] and the ensemble of central hypothyroidism, hypoprolactinemia and testicular enlargement [3]. The latter features may not yet be present in early life since the hypothyroid newborn had elevated concentrations of circulating prolactin (266 μg/L on day 3) and normal testicular volumes (2 mL by orchidometer).
In conclusion, nearly half a century after the first report on an enigmatic association of congenital nystagmus and central hypothyroidism, we identified a male newborn with the same association and a Xq26 deletion encompassing FRMD7 and IGSF1.
References
Schulman JD, Crawford JD. Congenital nystagmus and hypothyroidism. NEJM. 1969;280:708–10.
Tarpey P, Thomas S, Sarvananthan N, Mallya U, Lisgo S, Talbot CJ, et al. Mutations in FRMD7, a newly identified member of the FERM family, cause X-linked idiopathic congenital nystagmus. Nat Genet. 2006;38:1242–4.
Sun Y, Bak B, Schoenmakers N, van Trotsenburg AS, Oostdijk W, Voshol P, et al. Loss-of-function mutations in IGSF1 cause an X-linked syndrome of central hypothyroidism and testicular enlargement. Nat Genet. 2012;44:1375–81.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Reynaert, N., Braat, E. & de Zegher, F. Congenital nystagmus and central hypothyroidism. Int J Pediatr Endocrinol 2015, 7 (2015). https://doi.org/10.1186/s13633-015-0003-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13633-015-0003-5