
Abstract
Background
High-flow nasal oxygen therapy (HFOT) is a promising first-line therapy for acute respiratory failure. However, its weaning has never been investigated and could lead to unnecessary prolonged intensive-care unit (ICU) stay. The aim of this study is to assess predictors of successful separation from HFOT in critically ill patients. We performed a retrospective monocenter observational study over a 2-year period including all patients treated with HFOT for acute respiratory failure in the ICU. Those who died or were intubated without prior HFOT separation attempt, who were treated with non-invasive ventilation at the time of HFOT separation, or who received HFOT as a preventive treatment during the post-extubation period were excluded.
Results
From the 190 patients analyzed, 168 (88%) were successfully separated from HFOT at the first attempt. Patients who failed separation from HFOT at the first attempt had longer ICU length of stay than those who succeeded: 10 days (7–12) vs. 5 (4–8), p < 0.0001. Fraction of inspired oxygen (FiO2) ≤ 40% and a respiratory rate-oxygenation (ROX) index (calculated as the ratio of SpO2/FiO2 to the respiratory rate) ≥ 9.2 predicted successful separation from HFOT with sensitivity of 85% and 84%, respectively.
Conclusions
FiO2 ≤ 40% and ROX index ≥ 9.2 were two predictors of successful separation from HFOT at the bedside. Prospective multicenter studies are needed to confirm these results.
Similar content being viewed by others

Background
High-flow nasal oxygen therapy (HFOT) is increasingly used in the management of acute respiratory failure [1]. As compared to standard oxygen, it enables improved oxygenation, alveolar ventilation, comfort, and decreased work of breathing, in hypoxemic as well as in hypercapnic respiratory failure [2, 3]. Several large randomized-controlled trials have shown similar or better outcomes with HFOT than with standard oxygen therapy [4, 5] or with non-invasive ventilation [6, 7] in preventing or treating acute respiratory failure in intensive-care unit (ICU). However, during the recovery phase of acute respiratory failure, factors associated with successful separation from HFOT have never been assessed, i.e., the bridge from HFOT to standard oxygen therapy. As the continuation of HFOT might lead to unnecessarily prolonged ICU stay, we aimed at identifying predictors of successful HFOT separation.
Methods
We performed a retrospective observational monocenter study over a 2-year period (from January, 1st 2016 to December, 31th 2017). The study was approved by the local ethics committee, and given its non-interventional nature, informed consent was waived (CHU86-R2018-10-07).
Weaning from HFOT encompasses the reduction of FiO2 and flow to achieve a minimal support, and the separation attempt from HFOT per se. Given the design of the study, the reduction of HFOT support could not be assessed. Therefore, our primary outcome was to identify clinical variables associated with successful separation from HFOT.
All patients treated with HFOT for acute respiratory failure were included. Patients who died or were intubated without prior HFOT separation attempt, those who were treated with non-invasive ventilation at the time of HFOT separation, or who received HFOT as a preventive treatment during the post-extubation period (defined as the use of HFOT immediately after extubation for less than 48 h in the absence of clinical sign of respiratory failure) were excluded.
All patients were monitored until intubation, death, or successful separation from HFOT defined as discontinuation of HFOT for more than 48 h or until ICU discharge. In our unit, HFOT weaning was supervised by the attending physician and its separation usually considered when SpO2 was ≥ 92% with FiO2 ≤ 60%, independently from gas flow. HFOT separation failure was defined by respiratory failure requiring HFOT resumption, NIV initiation, intubation, or death within the first 48 h after switch from HFOT to standard oxygen.
Demographic data, ventilatory settings, and vital parameters under HFOT were collected before each separation attempt, and then under standard oxygen therapy after the separation from HFOT. For patients who failed at the first separation attempt from HFOT, these data were collected after HFOT resumption. Comorbidities, such as chronic cardiac failure (including coronary artery disease, severe valvulopathy, chronic atrial fibrillation, and heart failure of any cause) [8], chronic respiratory failure (defined as pulmonary function test alterations), and immunosuppression [9] were collected. The pulse oximetry to fraction of inspired oxygen ratio (SpO2/FiO2) and the respiratory rate-oxygenation (ROX) index (SpO2/FiO2 to respiratory rate) were calculated under HFOT before each separation attempt [10]. When available, last arterial blood gases under HFOT before each separation attempt were collected.
Continuous variables were expressed in mean ± standard deviation or median (interquartile range) according to their distribution and compared using the Mann–Whitney or the t test as appropriate. Categorical variables were expressed in number (percentage) and compared using the Fisher’s or Chi-square test as appropriate. Univariate analysis was performed to identify variables associated with successful separation from HFOT. For continuous variables, receiver-operating curves were plotted and the best threshold associated with successful separation from HFOT was assessed using the Youden’s index. A p value < 0.05 was considered significant.
Results
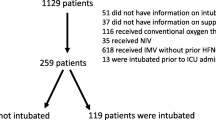
Among the 1494 patients admitted to our ICU over the study period, 421 were treated with HFOT. Of them, 231 were excluded for the following reasons: 92 patients had never undergone a separation attempt from HFOT (79 failed HFOT and 13 were transferred to a step-down intermediate-care unit under HFOT), 70 were under non-invasive ventilation while separation from HFOT, 61 received HFOT as a preventive treatment during the post-extubation period, and 8 had missing data (Fig. 1). As illustrated in Table 1, the 79 patients who failed HFOT (i.e., who were intubated after HFOT failure or who died after a do-not-intubate order) were older and had higher severity score upon ICU admission than the 190 who underwent at least one HFOT separation attempt.

Flow chart of patients included over the study period
At the first attempt, 168 out of the 190 patients (88%) retained in the analysis were successfully separated from HFOT, whereas 22 (12%) failed. Their characteristics are displayed in Table 2. Comorbidities were not different according to the outcome of the first HFOT separation attempt. Likewise, main reason for acute respiratory failure was not different according to the outcome of the first HFOT separation attempt, except for a higher proportion of pneumonia in the failed than in the successful HFOT separation group. Maximal gas flow and FiO2 set under HFOT were 50 ± 3 L/min and 75 ± 21%, respectively, and did not differ between the two groups (Table 2).
Patients who were successfully separated from HFOT at the first attempt required less oxygen and were more likely to have FiO2 ≤ 40% (85% vs. 59%, p = 0.007, Table 2 and Fig. 2) than those who failed. A FiO2 ≤ 40% predicted successful separation from HFOT at the first attempt with sensitivity of 85%, specificity of 41%, positive predictive value of 92%, negative predictive value of 26%, and accuracy of 80%. Likewise, the ROX index was higher in patients who were successfully separated from HFOT at the first attempt than in those who failed (12.7 vs. 10.2, p = 0.002) (Table 2 and Fig. 2). An ROX index ≥ 9.2 predicted successful separation from HFOT at the first attempt with sensitivity of 84%, specificity of 50%, positive predictive value of 93%, negative predictive value of 30%, and accuracy of 80%.

Last physiological parameters recorded at the bedside under high-flow nasal oxygen therapy before the first separation attempt. a Box-plot of FiO2 according to the success or failure of the first separation attempt (p = 0.02). b Box-plot of the ROX index according to the success or failure of the first separation attempt (p = 0.002)
ICU length of stay was significantly longer among patients who failed separation from HFOT at the first attempt than in those who succeeded: 10 days [7–12] vs. 5 [4–8], respectively (p < 0.0001). HFOT was resumed after 13 h [5–26] under standard oxygen. The main reason for HFOT separation failure at the first attempt was hypoxemia in 95% of cases (21/22). After HFOT resumption, SpO2/FiO2, ROX index, and PaO2/FiO2 under HFOT were lower than the last values measured under HFOT before the first separation attempt (Table 3). Interestingly, HFOT was resumed at higher flow than before the first separation attempt, whereas FiO2 was comparable between the two time periods. There was no difference in the last characteristics under HFOT before the first separation attempt according to the main reason for respiratory failure (Additional file 1: Table S1). After separation failure at the first attempt, 86% (19 out of 22) of patients were eventually separated successfully from HFOT. Their characteristics did not change between the HFOT separation success and the prior HFOT separation failure, except for higher ROX index at the time of the separation success than the separation failure, 12.4 ± 3.8 vs. 10.1 ± 3.1, p = 0.04.
Discussion
This study assessed predictors of successful separation from HFOT initiated for management of acute respiratory failure in the ICU. Our main findings are that only two bedside criteria, namely FiO2 and the ROX index calculated under HFOT, were different between patients who failed and those who succeeded in the first HFOT separation attempt.
FiO2 ≤ 40% was a predictor of separation success from HFOT with sensitivity reaching 85%, whereas this was not the case for HFOT flow. Therefore, this finding might suggest hastening the reduction of FiO2 rather than flow when weaning from HFOT. It is interesting to note that weaning from mechanical ventilation is recommended starting from a FiO2 ≤ 40%, illustrating the importance of decreasing oxygen requirements before separation from oxygenation support. Moreover, FiO2 of 45% is theoretically achievable under standard oxygen therapy with a flow of 5 L/min as a bridge to HFOT separation [11]. Therefore, separation from HFOT is more likely to be successful if a same range of FiO2 can be reached under standard oxygen therapy than under HFOT.
The ROX index was higher in patients successfully separated from HFOT. This score was initially built to predict the success of HFOT in patients with severe pneumonia with more accuracy than each of its components independently [10]. The best ROX index threshold predicting successful separation of HFOT was 9.2 using the Youden index. However, this threshold had poor specificity of only 50%, suggesting that half of patients who failed had ROX index higher than 9.2. To limit the risk related to HFOT separation failure, we identified the best positive predictive value for the ROX index.
Patients who failed the first HFOT separation attempt had lower oxygenation indices (SpO2/FiO2, ROX index, and PaO2/FiO2) after HFOT resumption than before HFOT separation, whereas FiO2 was not different between the two time periods. This difference in oxygenation could have been explained by HFOT flow-dependent lung recruitment. Indeed, increasing HFOT flow can increase end-expiratory lung volume and consequently improve oxygenation without changes in FiO2 [12]. Whether the assessment of end-expiratory lung impedance using electrical impedance tomography (a surrogate of end-expiratory lung volume) during HFOT flow reduction could help identifying patients who will fail HFOT separation is unknown [13]. Importantly, there were no differences between patients who failed according to the main reason for respiratory failure.
Our study has some limitations. First, this is a retrospective monocenter study which may limit the external validity of our results. However, our center is an expert in this technique, as illustrated by the high case volume of patients treated with HFOT. Second, there is no recommendation for the weaning of HFOT and it is possible that the first separation attempt occurred late, explaining the low rate of separation failure observed. There is an urgent need for studies assessing the reduction of HFOT settings to reach minimal support. Indeed, whether a reduction of FiO2 or flow would be the most suitable option to reach minimal support before the separation attempt is unknown and could not be tested given the design of our study. Finally, the clinical relevance of separation failure from HFOT is debatable. Indeed, its consequences are probably less severe than weaning failure from invasive ventilation, which is associated with a twofold increase in mortality [14]. However, patients who failed at the first attempt of separation from HFOT had significantly longer ICU stay than those who succeeded. Moreover, HFOT usually requires close monitoring in ICU or in intermediate-care unit, which represents a non-negligible cost. The economic impact of a weaning protocol is likely to be considered in further studies.
Conclusion
In this retrospective monocenter study, predictors of successful separation from HFOT at the bedside were FiO2 ≤ 40% and ROX index ≥ 9.2. The most interesting indicator might be FiO2, since its performance is similar to the ROX index and does not require any calculation at the bedside. A multicenter prospective study is mandatory to confirm the usefulness of these two easy-to-assess parameters with the aim of predicting successful separation from HFOT. Moreover, studies are needed to assess the most efficient way to reach minimal HFOT support.
Availability of data and materials
All data generated or analyzed during this study are included in this published article [and its additional information files].
Abbreviations
- HFOT:
-
high-flow nasal oxygen therapy
- ICU:
-
intensive-care unit
- FiO2 :
-
fraction of inspired oxygen
- SpO2 :
-
oxygen saturation
- ROX:
-
respiratory rate oxygenation
- SAPS II:
-
simplified acute physiology score II
- SOFA:
-
sequential organ failure assessment
References
Rochwerg B, Brochard L, Elliott MW, et al. Official ERS/ATS clinical practice guidelines: noninvasive ventilation for acute respiratory failure. Eur Respir J. 2017;50:1602426.
Mauri T, Turrini C, Eronia N, et al. Physiologic effects of high-flow nasal cannula in acute hypoxemic respiratory failure. Am J Respir Crit Care Med. 2017;195:1207–15.
Longhini F, Pisani L, Lungu R, et al. High-flow oxygen therapy after noninvasive ventilation interruption in patients recovering from hypercapnic acute respiratory failure: a physiological crossover trial. Crit Care Med. 2019;47:e506–11.
Frat J-P, Thille AW, Mercat A, et al. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med. 2015;372:2185–96.
Hernández G, Vaquero C, González P, et al. Effect of postextubation high-flow nasal cannula vs. conventional oxygen therapy on reintubation in low-risk patients: a randomized clinical trial. JAMA. 2016;315:1354.
Hernandez G, Vaquero C, Colinas L, et al. Effect of postextubation high-flow nasal cannula vs noninvasive ventilation on reintubation and postextubation respiratory failure in high-risk patients: a randomized clinical trial. JAMA. 2016;316:1565–74.
Stephan F, Barrucand B, Petit P, et al. High-flow nasal oxygen vs noninvasive positive airway pressure in hypoxemic patients after cardiothoracic surgery: a randomized clinical trial. JAMA. 2015;313:2331–9.
Thille AW, Harrois A, Schortgen F, et al. Outcomes of extubation failure in medical intensive care unit patients. Crit Care Med. 2011;39:2612–8.
Rubin LG, Levin MJ, Ljungman P, et al. 2013 IDSA clinical practice guideline for vaccination of the immunocompromised host. Clin Infect Dis. 2014;58:e44–100.
Roca O, Caralt B, Messika J, et al. An index combining respiratory rate and oxygenation to predict outcome of nasal high flow therapy. Am J Respir Crit Care Med. 2019;199:1368–76.
Wettstein RB, Shelledy DC, Peters JI. Delivered oxygen concentrations using low-flow and high-flow nasal cannulas. Respir Care. 2005;50:604–9.
Mauri T, Alban L, Turrini C, et al. Optimum support by high-flow nasal cannula in acute hypoxemic respiratory failure: effects of increasing flow rates. Intensive Care Med. 2017;43:1453–63.
Eronia N, Mauri T, Maffezzini E, et al. Bedside selection of positive end-expiratory pressure by electrical impedance tomography in hypoxemic patients: a feasibility study. Ann Intensive Care. 2017;7:76.
Thille AW, Cortés-Puch I, Esteban A. Weaning from the ventilator and extubation in ICU. Curr Opin Crit Care. 2013;19:57–64.
Acknowledgements
We gratefully thank Jeffrey Arsham, a native American speaker, for editing the original manuscript.
Funding
None.
Author information
Authors and Affiliations
Contributions
MR, AWT, JPF, and RC designed the study. MR collected data. RC performed the statistical analysis. MR, AWT, JPF, and RC interpreted results and drafted the manuscript. All authors enrolled patients in the study, and revised the manuscript critically for important intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the local ethics committee and given its non-interventional nature, informed consent was waived (CHU86-R2018-10-07).
Consent for publication
Not applicable.
Competing interests
AWT reports travel expenses to attend scientific meetings by Fisher and Paykel, Covidien, General Electrics, and Maquet-Getinge. J-PF reports consulting fees from Fisher and Paykel. RC reports travel expenses to attend scientific meetings by MSD and Fisher and Paykel. MR, FB, AV, SLP, and RR report no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1: Table S1.
Clinical and biological parameters collected under high-flow nasal oxygen therapy before the first separation attempt according to the reason for acute respiratory failure among the 22 patients who failed the separation attempt.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Rodriguez, M., Thille, A.W., Boissier, F. et al. Predictors of successful separation from high-flow nasal oxygen therapy in patients with acute respiratory failure: a retrospective monocenter study. Ann. Intensive Care 9, 101 (2019). https://doi.org/10.1186/s13613-019-0578-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13613-019-0578-8