
Abstract
Checkpoint protein inhibitor antibodies (CPI), including cytotoxic T-lymphocyte-associated antigen 4 inhibitors (ipilimumab, tremelimumab) and the programmed cell death protein 1 pathway/programmed cell death protein 1 ligand inhibitors (pembrolizumab, nivolumab, durvalumab, atezolizumab), have entered routine practice for the treatment of many cancers. They improve the outcome for many cancers, and more patients will be treated with CPI in the future. Although CPI can lead to adverse events (AE) less frequently than for chemotherapy, their use can require intensive care unit admission in case of severe immune-related adverse events (IrAE). Moreover, some of these events, particularly late events, are poorly documented, so a high level of suspicion should be maintained for patients receiving CPI. Intensivists should be aware in general of the known complications and appropriate management of these AE. Nevertheless, a multidisciplinary collaboration remains essential for their diagnosis and management. This review described the most severe complications related to CPI.
Similar content being viewed by others


Introduction
Checkpoint protein inhibitor antibodies (CPI), including cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) inhibitors (ipilimumab, tremelimumab) and the programmed cell death protein 1 pathway/programmed cell death protein 1 ligand (PD-1/PDL-1) inhibitors (pembrolizumab, nivolumab, durvalumab, atezolizumab), have entered routine practice for the treatment of many cancers. In contrast to classical chemotherapy, CPIs do not target tumor cells; rather they enhance activation of immune cells, particularly T cells (Fig. 1) [1]. They have been associated with better outcomes in a number of solid and hematological malignancies [2]. Moreover, compared with chemotherapy, their tolerance seems to be higher with fewer side effects.

Checkpoint inhibitors: mode of action. a Tumor cell inhibition of the immune system: tumor cells decrease T cell activation via two pathways. Within the tumor, connection between tumor cell PDL-1 and T cell receptor PD-1 associated with MHC T cell receptor leads to inhibition of T cell function. Within the lymphoid tissue, tumor cells inhibit dendritic cells via the CTLA-4 pathway. Cancer cells increase CTLA4 expression by dendritic cells, through T reg cell stimulation. Interaction of CTLA4-Receptor on T cell, inhibits T cell function [1]. b Mode of action of CTLA-4i or PD-1/PDL-1i. PD-1/PDL-1i blocks the connection between PD-1 and PDL-1 and prevents the inhibition of T cells. T cell cytotoxicity then attacks the tumor cells. CTLA-4i blocks the connection between dendritic cells and T cells related to CTL14. CTLA-4i removes the inhibition related to dendritic cell on T cells
These new molecules are mostly prescribed for melanoma and non-small cell lung cancer (NSCLC), but also for other malignancies such as renal cell carcinoma, bladder carcinoma, squamous cell carcinoma of the head and neck, lymphoma [2]. The list of treatment indications will likely extend as the years go by, even as a first-line therapy. The number of patients treated will increase because of expanded indications and better survival [2,3,4,5]. Moreover, the optimal duration of treatment remains unknown.
CPIs are associated with immune-related adverse events (IrAE) that need to be carefully monitored and managed during and after treatment. These drugs can promote infiltration of immune cells into normal tissues, which may lead to immune-mediated disorders. Almost every organ may be affected: skin, bowels, liver, lungs, kidneys, eyes, endocrine tissues, central nervous system [6]. In up to 20% of cases, severe and even life-threatening AE can occur and lead to intensive care unit (ICU) admission [7, 8].
This review focuses on the most severe IrAE that intensivists may encounter. Maintaining a high level of suspicion is a major challenge, as some of the toxicities might be uncovered later, in patients treated for a longer period of time with prolonged survival and new indications for those CPI.
Methods
We searched Medline and PubMed for reviews and original articles on CPI for treatment of solid tumors in adults published in English between 1 January 2009 and 30 January 2018, using the terms ‘antibody, monoclonal/adverse event’ [Mesh] AND ‘ipilimumab’ [Mesh], ‘tremelimumab’ [Mesh], ‘pembrolizumab’ [Mesh], ‘nivolumab’ [Mesh], ‘durvalumab’ [Mesh], ‘atezolizumab’, [Mesh], and ‘immunotherapy’ [Mesh]. We also searched using individual terms such as ‘CTLA4 inhibitors’, ‘programmed cell death protein 1 pathways’, ‘hepatitis’, ‘pneumonitis’, ‘skin’, ‘hypophysitis’, ‘colitis’, and ‘acute kidney failure’, ‘myocarditis, ‘neurological complication’, ‘encephalopathy’, ‘anemia’. Only severe adverse events eventually associated with ICU admission were considered for this review. Most of the articles were descriptive reports or randomized studies with safety outcomes, over the last 10 years of the search period. We used only original reports when available.
Statistical analysis
Overall proportion of included study with predefined complication was reported as proportion (95% CI). Publication bias was assessed by visually inspecting the funnel plot, and summary estimates of relative risk and their 95% confidence interval were calculated using both fixed and random-effects model.
Cochran’s χ2 test and I2 test for heterogeneity were used to assess inter-study heterogeneity [9]. The χ2 test assesses whether observed differences among results are compatible with chance alone and the I2 describes the percentage of the variability in effect estimates that results from heterogeneity rather than from sampling error. An I2 test for heterogeneity above 0.25 was considered to indicate moderate heterogeneity. Statistically significant heterogeneity was considered present at χ2 p < 0.10 and I2 > 0.5. All effect sizes with a p < 0.05 were considered significant. Tests were two-sided.
All analyses were carried out with software R, version 3.4.4. The ‘meta’, the ‘metasens’ and ‘metaphor’ packages were used to produce forest plots and funnel plots.
Epidemiology: the magnitude of the problem (Fig. 2)
The severity of AE is defined for each organ by the National Cancer Institute (CTCAE_4.03_2010-06-14_QuickReference_8.5x11.pdf) (Tables 1, 2).

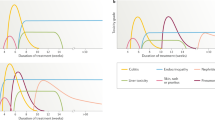
Frequency of immune-related adverse events. a Toxicity related to anti-PD-1/PDL-1i; b toxicity related to CTLA-4i. The size of the circles reflects the incidence of toxicity: blue, toxicity of any grade; red, grade III/IV toxicity. None of the circles describe toxicity related to CTLA-4i associated with PD-1/PDL-1i inhibitors (the incidence of combined treatments is higher than the toxicity of each inhibitor). Incidence data from [8] and [47]

In a meta-analysis of 21 randomized phase II/III immunotherapy trials (including 11,454 patients of whom 6528 received a CPI) conducted between 1996 and 2016, the incidence of fatal IrAE was 0.64%, mostly due to ipilimumab-induced colitis [7].
In patients receiving CPI, grade III–IV (Table 1) colitis occurred in 1.5%, grade III–IV aspartate aminotransferase (AST) elevation in 1.5%, grade III–IV rash in 1.1%, grade III–IV pneumonitis in 1.1%, hypothyroidism was observed in 0.3% of cases. Ipilimumab was associated with a higher risk of grade III–IV colitis than PD-1/PDL-1i [7]. In a recent meta-analysis, PD-1 and PDL-1i seem to be associated with grade III–IV IrAE with similar frequencies [10]. However, the incidence of these IrAE was far lower than the rate of complications from chemotherapy, particularly infections. Grade III–V toxicities were more common with CTLA-4i than with PD-1i (31% vs. 10%) [11]. IrAE leading to death were exceedingly rare for PD-1i (PDL-1i 0.1%, PD-1i 0.3%) and most often secondary to pneumonitis, whereas fatal gastrointestinal (GI) IrAE (diarrhea, colitis, colonic perforation) mostly occurred with CTLA-4i (severe events 31%) [11]. Furthermore, the safety profile of CPI varies among tumor types: melanoma has a higher risk of GI and skin IrAE and lower frequencies of pneumonitis [12, 13]. Moreover, combining two CPIs leads to more frequent severe complications in up to 55% of patients [14,15,16]. Also, the incidence of rAE and severe IrAE will probably increase in the future, with the increasing number of patients currently treated and the use of combination regimens already tested in several trials [17,18,19].
The kinetics of IrAE onset remains difficult to describe, but IrAE seem uncommon before 1 months of treatment [6, 13]. Although, in a recent report, severe IrAE can appear early during the treatment course [20] (within 40 days with Ipilimumab and anti-PD1–/PDL1 and 14.5 days with combination treatment), late complications of CPI may occur, sometimes up to 1 year after the start of the PDL1, and clinicians must remain aware of possible complications during follow-up [21]. Moreover, IrAE can occur after the CPI has been discontinued [22].
Toxicities associated with PD-1/PDL-1i agents may be slower to resolve than with ipilimumab, and long-term follow-up is therefore advised [23].
Immune-related adverse events (Table 2)
This section describes the most severe IrAE according to the frequency and severity of organ involvement (Figs. 2, 3, 4, Additional file 1: Fig. S1). In some recent studies, high-grade toxicity seems to be associated with high tumoral response rates [24, 25].

Frequencies of grade III and IV IrAEIrAE in studies. Meta-analysis of randomized control trials including CTLA4i (upper plot), CTLA4i + PD1i/PDL1i (middle plot) or PD1i/PDL1i (lower plot). The forest plots represent the frequencies of IrAEIrAE organ by organ. a Severe gastrointestinal irEA; b severe lung IrAE.

Frequencies of grade III and IV IrAEIrAE in studies. Meta-analysis of randomized control trials including CTLA4i (upper plot), CTLA4i + PD1i/PDL1i (middle plot) or PD1i/PDL1i (lower plot). The forest plots represent the frequencies of IrAEIrAE organ by organ. a Severe liver IrAE; b severe neurological IrAE.
Gastrointestinal disorders
GI disorders are the most frequent IrAE and occur particularly with CTLA-4i. Occurrence of colitis after PD-1i/PDL-1i has been reported only in few patients (< 1%) [23, 26]. At ICU admission, clinicians must distinguish diarrhea alone from colitis. Diarrhea may lead to ICU admission because of dehydration and electrolytes disturbances. Colitis is associated with abdominal pain and inflammation.
Symptoms of GI IrAE have been described in 41/137 patients, largely related to ipilimumab (CTLA4i) [27]. The symptoms can occur within the first few days following the first dose of ipilimumab or weeks after the last dose [20, 26, 27]. On admission, symptoms had been present for 5 days on average (1–64 days), mainly diarrhea (> 90%), abdominal pain (20%), nausea/vomiting (20%), fever (10–12%), anal pain (10%), bleeding (2%), and constipation (2%) [27].
Computed tomography (CT) and/or endoscopy showed evidence of colic inflammation [27]. Endoscopy found histologically confirmed colitis in more than 80% of patients with erythema and ulcerations [27].
Histological examination revealed neutrophilic (46%) and/or lymphocytic (15%) infiltrations, associated in rare cases with abscess and granuloma. These features seem similar to cryptogenic inflammatory bowel diseases [27].
Colitis was in some cases refractory to steroid treatment and led to colonic perforation [27, 28]. In a recent observational study of 21 patients, two patients had refractory colitis lasting for more than 130 days (10 to 12 times the half-life of ipilimumab). Those two patients had previously received radiotherapy. In addition, association of CPI with chemotherapy or other immune therapy may increase the risk of severe colitis [28].
Diarrhea of varying grade occurs frequently in patients treated with CTLA-4i. However, alternative diagnoses should be evaluated at ICU admission. First, an infectious etiology should be excluded, particularly Clostridium difficile (Table 2). The incidence of C. difficile in CPI-treated patients remains unknown, with only a small number of cases described [29, 30]. The diagnostic workup must include at least stool culture and screening for C. difficile and cytomegalovirus (PCR and/or colon biopsy). CT and endoscopy should be performed if possible to distinguish colitis from other possible diagnoses (bowel cancer, other inflammatory bowel disease, etc.).
Although GI adverse events related to PD-1i are rare, severe colitis has been described after long-term PD-1i treatment [26].
Lung disorders, pneumonitis/acute respiratory distress syndrome
Although pneumonitis remains rare (4% in NSCLC and 3% in melanoma), it can lead to severe acute respiratory distress syndrome (ARDS) (0.8–1% grade 3 or higher toxicity in the studies included) [31,32,33]. Rare cases of severe pneumonitis have been described in phase I trials with PD-1i and PDL-1i [34, 35]. CTLA-4i are rarely associated with pneumonitis although some cases series have shown non-severe [36] or severe pneumonitis [37]. Pneumonitis is more frequent during NSCLC treatment than melanoma treatment, particularly when other lung process is present (tobacco use, chronic obstructive pulmonary disease, etc.) or during combined treatment [33]. Pneumonitis should be distinguished from cancer relapse or infection [38]. One case report described a “flare pneumonitis” after tapering corticosteroids without new treatment with PD-1i [39]. More interestingly, in a descriptive study of 43 cases of pneumonitis related to PD-1/PDL-1i, more than half of the patients described other immune toxicity as well [40]. Common symptoms included dyspnea (53%), cough (35%), fever (12%), and chest pain (7%). ARDS occurred in rare cases [40].
PD-1i-related pneumonitis was described in 20 of 170 patients treated with PD-1i. Among them, five patients had severe pneumonitis occurring within 2.6 months after the beginning of treatment. Cough was the most frequent symptom, followed by dyspnea and fever. The most frequent CT findings were ground-glass opacities in all patients, reticular opacities (19/20 patients) and airspace consolidation (12/20 patients), with a common organizing pneumonia pattern in 13 (65%) patients (Fig. 5). Abnormal findings occurred in the lower lobes with a peripheral distribution [33, 39, 41]. Another CT pattern encountered was non-specific interstitial pneumonia. Unfortunately, none of the studies described the findings of bronchoalveolar lavage (BAL). Other causes of acute respiratory failure (infection including, Pneumocystis jirovecii pneumonia, relapsing cancer etc.) must be excluded. BAL should be performed in those cases. In one study, lung biopsy was performed in 11 patients. The histological findings were cellular interstitial pneumonitis, common organizing pneumonia, or diffuse alveolar damage. In three patients, no lesion was found [40].

Example of thoracic CT in immune-related pneumonitis. The patient had been treated for NSCLC with pembrolizumab for 2 months. He developed acute respiratory failure. CT showed the typical organizing pneumonia pattern
Pneumonitis related to ipilimumab is rare but has been reported as sarcoidosis/granulomatosis-like, rarely associated with ARDS [36, 37].
Management of patients with suspected grade III–IV pneumonitis should include clinical examination to search for other associated immune toxicities, leading to higher probability of IrAE pneumonia, and CT should be performed to define the lesions. BAL and potentially lung biopsy should be considered (Table 2).
Myocarditis and cardiac insufficiency
Myocardial complications remain rare, far below the rate of toxicities related to radiotherapy and chemotherapy. However, cases reports described grade III/IV IrAE, ranging from cardiomyopathy to acute myocarditis and cardiac arrest [42, 43]. This rare complication remains one of the most severe consequences and occurs more frequently with the combination of CTLA-4i and PD-1i or PDL-1i [44].
It may occur at the initiation of therapy or after several weeks of treatment. Cardiovascular risk factors (e.g. hypertension and tobacco use) were not always present in cases reports of cardiac toxicity [45, 46]. Interestingly, in a recent study of eight cases, five patients had already at least one other IrAE when the cardiac side effect occurred [47].
The best management of CPI-related myocarditis remains unknown. Wang et al. proposed an algorithm to detect and treat myocarditis, including pre-treatment troponin and EKG [45]. Other causes of myocardial dysfunctions should be ruled out (pulmonary embolism, ischemic myocardial dysfunction) (Table 2). Treatment may require extracorporeal membrane oxygenation, infliximab, or polyvalent intravenous immunoglobulins [44, 47, 48].
Some cases of pericardial effusion, sometimes with tamponade, have also been reported [49,50,51]. A few rare cases of pericarditis occurred that were treated with steroids. When histological examination was performed, T cell infiltrates were found with cardiomyocytes fibrosis, in some cases, [46].
Neurologic disorders: encephalopathy, Guillain–Barré syndrome, myasthenia, myelitis
Because of the severity of symptoms, neurological toxicity remains one of the most important IrAE, mostly associated with CTLA-4i [52]. Although these complications are common, the proportion of grade III/IV cases remains limited. Neurological complications may appear within 4 months after initiation of treatment, but clinicians should maintain a high level of awareness even when these drugs were recently introduced. Furthermore, they are usually prescribed for a long duration which could lead to delayed toxicity. Some cases reports describe permanent disability after neurological toxicity. Central neurotoxicity can take several forms, from headache after ipilimumab induction to chronic encephalopathy or aseptic meningitis [53, 54]. Stroke and posterior reversible encephalopathy syndrome after ipilimumab may occur and could lead to ICU admission [52]. Seizures remain rare [54,55,56], peripheral neurotoxicity occurs with Guillain–Barré syndrome or neuromyopathy, after CTLA-4i or anti-PDL-1i treatment [52, 53]. Myasthenic syndromes may occur mostly with PD1i treatment [57, 58], early after treatment initiation [59] (Table 2). Other etiologies, particularly metastases, should be ruled out with MRI and or lumbar puncture.
In an observational study of 352 patients with melanoma, 10 patients were found to have severe neurological (central and peripheral) complications (including six patients with high-grade complications). Eight of those patients showed a sustained response to steroid therapy and were alive after 8 to 35 months [53]. The high survival rate after neurological CPI justifies ICU admission, but other etiologies should be promptly ruled out as well.
Endocrine-related adverse events
Endocrine-related AE are irreversible IrAE and lead to continuous substitutive treatment. Failure to diagnose these IrAE can lead to life-threatening complications particularly hypophysitis and adrenal insufficiency. Higher incidences of endocrine-related AE were found with combination therapy and when high dose therapy was used [60].
Thyroid dysfunction
Thyroid dysfunction, isolated or associated with hypophysitis, occurred in up to 10% of cases and was severe (grade III/IV) in only 1–2% of patients [43, 61]. Thyroid dysfunction (hypothyroidism or hyperthyroidism) could be primary or secondary in origin. Associated hypophysitis should be considered particularly with CTLA-4i [61].
Although thyrotoxicosis has been described in rare cases, primary hypothyroidism is more frequent than hyperthyroidism and mostly related to PD-1i or PDL-1i treatment. Hashimoto’s disease has been described in rare cases [6]. Other associated endocrinopathies should also be considered [60].
Hypophysitis
First described with CTLA-4i, hypophysitis can also occasionally occur with PD-1i and anti-PDL-1i treatment. Intensivists must be aware of this complication, which can be life-threatening particularly when acute adrenal insufficiency is the first symptom. Hyponatremia and dehydration may lead to ICU admission. Adrenal insufficiency is much more frequent with immunotherapy than with conventional treatment [53].
Hypophysitis was investigated in 211 patients treated with CTLA4i for melanoma and developed early in the course of the treatment. Hypophysitis occurred in 19 (9%) patients within 4 months of treatment and was symptomatic in 83% of these cases. Associated hypothyroidism occurred in 11 (58%) patients, while brain magnetic resonance imaging revealed abnormal findings in only 12 (63%) patients [62]. Hypophysitis seems to be related to hypersensitivity of hypophysis cells carrying CTLA-4 receptors [63].
Other endocrine adverse events
Primary adrenal insufficiency remained rare (< 1%) [62].
Severe diabetes mellitus with ketosis was described in 0.4% of cases with PDL-1i. Diabetes was related to pancreatic disorder or to autoimmune insulin-dependent diabetes. (Table 2) [64, 65]. Ketoacidosis may require ICU admission [64].
Liver disorders
Liver dysfunction, mostly related to autoimmune-like hepatitis, has been described with CTLA-4i treatment but very rarely with PD-1i or PDL-1i treatment [66, 67]. In a case series of 11 patients receiving one to four doses of ipilimumab, the authors described acute panhepatitis with CD8 + T-lymphocyte perivenular infiltrate and endothelialitis. Some of the patients had pre-existing risk factors for chronic liver disease with nonalcoholic steatohepatitis or steatosis-associated characteristics. CT showed hepatomegaly and periportal edema. Viral hepatitis (VH), tumor progression, and autoimmune hepatitis should be excluded by biological diagnostic testing including testing for hepatitis A, B, C or E, antinuclear antibodies, smooth-muscle antibodies, and anti-mitochondrial antibodies (Table 2). No case of fulminant hepatitis has yet been described [66, 68] with CTLA-4i treatment. CMV-related hepatitis coupled with colitis has been described [69].
One case of fulminant hepatitis has been described within 34 weeks after PD-1i was started, but no liver biopsy was performed [70]. The patient improved with steroids.
The rate of PD-1i related hepatitis grade III was 0.5% during melanoma treatment and has not been described during lung cancer treatment [4, 71].
Pancreatic disorders
In a recent study of 496 patients treated for melanoma, pancreatitis disorders occurred in 9 (0.02%) patients including seven patients with grade III/IV pancreatitis, within 6 to 20 weeks after treatment initiation [6]. In earlier studies, elevated lipase was reported in less than 1% of patients [4, 71].
Some authors recently demonstrated that high lipase level was not associated with pancreatic disease in most cases and should not be automatically associated with treatment cessation [72].
Skin
Skin involvement is frequent: 50% of patients experiment rash or pruritus with CTLA-4i and 22% with PD-1i [73]. However, grade III/IV IrAE are very rare, reported in 0 to 4% of patients after ipilimumab treatment [13] and even more rarely with PD-1/PDL-1i treatment [74, 75]. Stevens–Johnson syndrome is one of the most severe complications (Table 2).
Kidney disorders
According to clinical trials, acute kidney injury (AKI) is relatively uncommon with anti-cancer immune CPI compared with other types of IrAE [76]. However, both circulating anti-double-stranded DNA antibodies and glomerular IgG and C3 deposits have been reported in mice treated with CTLA-4i [77].
During ipilimumab monotherapy, elevated creatinine was reported in 1.4% (any grade) and 0.2% (grade III or IV) of the patients. Similarly, during PD-1i monotherapy, elevated creatinine was reported in 1.7% (any grade) and 0.8% (grade III or IV) of the patients, respectively. However, during combination therapy, the incidence of AKI was higher in clinical trials, resulting in 1.7% of grade III or IV creatinine elevation.
The most accurate data were reported in the series by Cortazar et al. and Shirali et al. [78, 79]. They reported the clinical and histological features of 13 patients with CPI-related AKI (various cancers, mainly melanoma; various CPIs) who underwent kidney biopsy. The most prevalent pathologic lesion was acute tubulo-interstitial nephritis in 12 patients, including three with granulomatous features, and one case of thrombotic microangiopathy (TMA) (Table 2).
The renal prognosis remains good after discontinuing CPI and in most cases prescription of steroids (Table 2). However, the persistence of kidney failure after 3 weeks, higher age, and greater degree of interstitial fibrosis have been associated with poor prognosis [80]. In some reports, interstitial fibrosis may occur as soon as 10 to 14 days after initiation of treatment.
Hematological syndromes
Rare cases of hemolytic anemia leading to ICU admission have been described with nivolumab and ipilimumab, IgG or C3 mediated [81]. They may respond to corticosteroids, but rituximab may be required in some cases. Resumption of PD-1i/PDL-1i after resolution of anemia was not always associated with a recurrence of anemia [82, 83] (Table 2).
Management
Due to the potential reversibility with treatment, CPI-related severe toxicity should lead to ICU admission at least for a time-limited trial, in case of organ failure or for patients at risk of organ failure. Such a trial may include mechanical ventilation, vasopressors, renal replacement therapy, and even extracorporeal membrane oxygenation in selected patients.
The recommendations for managing IrAE arise from general clinical consensus, because no prospective trials have been conducted to specifically test whether one management strategy is superior to another. Early recognition and treatment of IrAE are believed to be important in mitigating their severity. For severe grade III–IV, IrAE drug should be discontinued immediately [84].
From a practical standpoint, the management of such patients requires a close collaboration between specialists (e.g. nephrologist, hepatologist, infectious diseases specialist), oncologists, and intensivists (Fig. 6).

Management of the most frequent IrAEs in the ICU. ICU intensive care unit, MV mechanical ventilation, RRT renal replacement therapy, ECLS extracorporeal life support
Although steroid treatment should be initiated as soon as possible, some other etiologies like infections or cancer progression must be ruled out. Table 2 summarizes the diagnostic work up before treatment. Most of the differential diagnoses can be ruled out quickly and work up should not delay the initiation of steroid treatment in case of severe IrAE. Systemic corticosteroids (oral or IV methylprednisolone) must be initiated at a dose of 1–2 mg/kg/day for 3 days and then reduced to 1 mg/kg/day. Corticosteroids regimen should then follow a gradual tapering over a period of at least 1 month [85]. Whenever IrAEs worsen or do not improve sufficiently after 3–5 days despite the use of adequate steroids dosage, additional immunosuppressive drugs should be considered. Although none of these treatments has been evaluated, they may include:
-
Antitumor necrosis factor alpha (anti-TNF) [86] in case of colitis or pneumonitis, but not hepatitis because of the risk of hepatotoxicity [8].
-
Mycophenolate mofetil (500–1000 mg twice a day) for hepatitis, cardiotoxicity, or pneumonitis [8, 45].
-
Antithymocyte immunoglobulins for hepatitis, cardiotoxicity, or severe neurotoxicity [8, 45].
Hypothyroidism should be managed with thyroid hormone replacement and hyperthyroidism with standard anti-thyroid pharmacotherapy and beta-blockers in symptomatic cases [8].
Long-term treatment with corticosteroids and sometimes anti-TNF drugs may be complicated by severe opportunistic infections such as fungal infection, tuberculosis, or CMV. Therefore, it is recommended to give antibiotic prophylaxis with oral trimethoprim/sulfamethoxazole (400 mg/125 mg 3 times a week) together with steroids and to test patients for tuberculosis before adding any additional immunosuppressive drug (e.g. TNF alpha inhibitors) to corticosteroids [85.].
As the pathophysiological mechanism of IrAE involves excessive activation of the immune system, leading to toxic effects potentially targeting any organ and mimicking autoimmune diseases in their clinical presentation, it may also be difficult to differentiate between the side effects of CPI and the development of autoimmune paraneoplastic syndromes. This was emphasized in a recent report of patients without previous autoimmune manifestations who developed autoimmune encephalitis during immunotherapy [55, 87].
Interestingly, the same CPI may be reintroduced after IrAEIrAE resolution in most cases of grade III IrAEIrAE (Table 2). For grade IV IrAEIrAE, resumption of CPI may be more questionable. However, restarting CPI must be considered after a close collaboration between oncologist, specialist and intensivist, while weighing the individual risk/benefit ratio, and should be shared with the patient (Table 2).
Interestingly, some studies described higher cancer response rate for patients who also experienced high-grade IrAEIrAE [13]. These results need to be confirmed.
Conclusion
Severe immune-related complications of checkpoint protein inhibitor antibodies complications remain rare, but the number of patients treated will continue to rise. Although adverse events may occur less frequently after immunotherapy than after chemotherapy, intensivists should be aware of the side effects of this new type of medication that may require ICU admission. Moreover, some immune-related complications remain unknown and will reveal themselves with the increasing use of those new therapeutic agents.
Abbreviations
- CPI:
-
checkpoint protein inhibitors
- PD-1:
-
programmed cell death protein 1
- PD-1i:
-
programmed cell death protein 1 inhibitors
- PDL-1:
-
programmed cell death protein 1 ligand
- PDL-1i:
-
programmed cell death protein 1 ligand inhibitors
- CTLA-4:
-
cytotoxic T-lymphocyte antigen 4
- CTLA-4i:
-
cytotoxic T-lymphocyte antigen 4 inhibitors
- IrAE:
-
immune-related adverse events
References
Chen DS, Mellman I. Oncology meets immunology: the cancer-immunity cycle. Immunity. 2013;39(1):1–10.
Postow MA, Sidlow R, Hellmann MD. Immune-related adverse events associated with immune checkpoint blockade. Longo DL, éditeur. N Engl J Med. 2018;378(2):15868.
Borghaei H, Paz-Ares L, Horn L, Spigel DR, Steins M, Ready NE, et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N Engl J Med. 2015;373(17):1627–39.
Robert C, Schachter J, Long GV, Arance A, Grob JJ, Mortier L, et al. Pembrolizumab versus ipilimumab in advanced melanoma. N Engl J Med. 2015;372(26):2521–32.
Brahmer J, Reckamp KL, Baas P, Crinò L, Eberhardt WEE, Poddubskaya E, et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N Engl J Med. 2015;373(2):123–35.
Hofmann L, Forschner A, Loquai C, Goldinger SM, Zimmer L, Ugurel S, et al. Cutaneous, gastrointestinal, hepatic, endocrine, and renal side-effects of anti-PD-1 therapy. Eur J Cancer. 2016;60:190–209.
De Velasco G, Je Y, Bossé D, Awad MM, Ott PA, Moreira RB, et al. Comprehensive meta-analysis of key immune-related adverse events from CTLA-4 and PD-1/PD-L1 inhibitors in cancer patients. Cancer Immunol Res. 2017;5(4):312–8.
Naidoo J, Page DB, Li BT, Connell LC, Schindler K, Lacouture ME, et al. Toxicities of the anti-PD-1 and anti-PD-L1 immune checkpoint antibodies. Ann Oncol. 2015;26(12):2375–91.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Pillai RN, Behera M, Owonikoko TK, Kamphorst AO, Pakkala S, Belani CP, et al. Comparison of the toxicity profile of PD-1 versus PD-L1 inhibitors in non-small cell lung cancer: a systematic analysis of the literature: PD-1 and PD-L1 inhibitor toxicities in NSCLC. Cancer. 2018;124(2):271–7.
Khoja L, Day D, Wei-Wu Chen T, Siu LL, Hansen AR. Tumour- and class-specific patterns of immune-related adverse events of immune checkpoint inhibitors: a systematic review. Ann Oncol. 2017;28(10):2377–85.
Michot JM, Bigenwald C, Champiat S, Collins M, Carbonnel F, Postel-Vinay S, et al. Immune-related adverse events with immune checkpoint blockade: a comprehensive review. Eur J Cancer. 2016;54:139–48.
Weber JS, Kähler KC, Hauschild A. Management of immune-related adverse events and kinetics of response with ipilimumab. J Clin Oncol. 2012;30(21):2691–7.
Boutros C, Tarhini A, Routier E, Lambotte O, Ladurie FL, Carbonnel F, et al. Safety profiles of anti-CTLA-4 and anti-PD-1 antibodies alone and in combination. Nat Rev Clin Oncol. 2016;13(8):473–86.
Pollack MH, Betof A, Dearden H, Rapazzo K, Valentine I, Brohl AS, et al. Safety of resuming anti-PD-1 in patients with immune-related adverse events (irAEs) during combined anti-CTLA-4 and anti-PD1 in metastatic melanoma. Ann Oncol. 2017;29(1):250–5.
Sznol M, Ferrucci PF, Hogg D, Atkins MB, Wolter P, Guidoboni M, et al. Pooled analysis safety profile of nivolumab and ipilimumab combination therapy in patients with advanced melanoma. J Clin Oncol. 2017;35(34):3815–22.
Antonia SJ, López-Martin JA, Bendell J, Ott PA, Taylor M, Eder JP, et al. Nivolumab alone and nivolumab plus ipilimumab in recurrent small-cell lung cancer (CheckMate 032): a multicentre, open-label, phase 1/2 trial. Lancet Oncol. 2016;17(7):883–95.
Motzer RJ, Escudier B, McDermott DF, George S, Hammers HJ, Srinivas S, et al. Nivolumab versus everolimus in advanced renal-cell carcinoma. N Engl J Med. 2015;373(19):1803–13.
Motzer RJ, Tannir NM, McDermott DF, Arén Frontera O, Melichar B, Choueiri TK, et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N Engl J Med. 2018;378(14):1277–90.
Wang DY, Salem J-E, Cohen JV, Chandra S, Menzer C, Ye F, et al. Fatal toxic effects associated with immune checkpoint inhibitors: a systematic review and meta-analysis. JAMA Oncol. 2018;4(12):1721–8.
Ernstoff MS, Gandhi S, Pandey M, Puzanov I, Grivas P, Montero A, et al. Challenges faced when identifying patients for combination immunotherapy. Future Oncol. 2017;13(18):1607–18.
Tan I, Malinzak M, Salama AKS. Delayed onset of neurosarcoidosis after concurrent ipilimumab/nivolumab therapy. J Immunother Cancer. 2018;6(1):77.
Collins M, Michot JM, Danlos FX, Mussini C, Soularue E, Mateus C, et al. Inflammatory gastrointestinal diseases associated with PD-1 blockade antibodies. Ann Oncol. 2017;28(11):2860–5.
Judd J, Zibelman M, Handorf E, O’Neill J, Ramamurthy C, Bentota S, et al. Immune-related adverse events as a biomarker in non-melanoma patients treated with programmed cell death 1 inhibitors. Oncologist. 2017;22(10):1232–7.
Lisberg A, Tucker DA, Goldman JW, Wolf B, Carroll J, Hardy A, et al. Treatment-related adverse events predict improved clinical outcome in NSCLC patients on KEYNOTE-001 at a single center. Cancer Immunol Res. 2018;6(3):288–94.
Yasuda Y, Urata Y, Tohnai R, Ito S, Kawa Y, Kono Y, et al. Immune-related colitis induced by the long-term use of nivolumab in a patient with non-small cell lung cancer. Intern Med. 2018;57(9):1269–72.
Beck KE, Blansfield JA, Tran KQ, Feldman AL, Hughes MS, Royal RE, et al. Enterocolitis in patients with cancer after antibody blockade of cytotoxic T-lymphocyte-associated antigen 4. J Clin Oncol. 2006;24(15):2283–9.
Lord JD, Hackman RC, Moklebust A, Thompson JA, Higano CS, Chielens D, et al. Refractory colitis following anti-CTLA4 antibody therapy: analysis of mucosal FOXP3 + T Cells. Dig Dis Sci. 2010;55(5):1396–405.
Du-Thanh A, Pallure V, Girard C, Dereure O, Guillot B. Clostridium difficile infection may loom behind ipilimumab-induced auto-immune colitis. Eur J Dermatol. 2015;7–8(4):344.
Gupta A, Khanna S. Ipilimumab-associated colitis or refractory Clostridium difficile infection? BMJ Case Rep. 2015. https://doi.org/10.1136/bcr-2015-211160.
Possick JD. Pulmonary toxicities from checkpoint immunotherapy for malignancy. Clin Chest Med. 2017;38(2):223–32.
Nishino M, Sholl LM, Hatabu H, Ramaiya NH, Hodi FS. Anti-PD-1-related pneumonitis during cancer immunotherapy. N Engl J Med. 2015;373(3):288–90.
Nishino M, Giobbie-Hurder A, Hatabu H, Ramaiya NH, Hodi FS. Incidence of programmed cell death 1 inhibitor-related pneumonitis in patients with advanced cancer: a systematic review and meta-analysis. JAMA Oncol. 2016;2(12):1607.
Garon EB, Rizvi NA, Hui R, Leighl N, Balmanoukian AS, Eder JP, et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N Engl J Med. 2015;372(21):2018–28.
Topalian SL, Hodi FS, Brahmer JR, Gettinger SN, Smith DC, McDermott DF, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med. 2012;366(26):2443–54.
Franzen D, Schad K, Kowalski B, Clarenbach CF, Stupp R, Dummer R, et al. Ipilimumab and early signs of pulmonary toxicity in patients with metastastic melanoma: a prospective observational study. Cancer Immunol Immunother. 2018;67(1):127–34.
Franzen D, Schad K, Dummer R, Russi EW. Severe acute respiratory distress syndrome due to ipilimumab. Eur Respir J. 2013;42(3):866–8.
Mahjoubi L, Gazzah A, Marabelle A, Le Roy Ladurie F, Lambotte O, Caramella C, et al. Late-occurring nivolumab-induced cryptogenic organising pneumonia mimicking lung progression in a patient with metastatic non-small cell lung cancer. Eur J Cancer. 2017;85:155–7.
Nishino M, Chambers ES, Chong CR, Ramaiya NH, Gray SW, Marcoux JP, et al. Anti-PD-1 inhibitor-related pneumonitis in non-small cell lung cancer. Cancer Immunol Res. 2016;4(4):289–93.
Naidoo J, Wang X, Woo KM, Iyriboz T, Halpenny D, Cunningham J, et al. Pneumonitis in patients treated with anti-programmed death-1/programmed death ligand 1 therapy. J Clin Oncol. 2017;35(7):709–17.
Delaunay M, Cadranel J, Lusque A, Meyer N, Gounaut V, Moro-Sibilot D, et al. Immune-checkpoint inhibitors associated with interstitial lung disease in cancer patients. Eur Respir J. 2017;50(2):1700050.
Frigeri M, Meyer P, Banfi C, Giraud R, Hachulla A-L, Spoerl D, et al. Immune checkpoint inhibitor-associated myocarditis: a new challenge for cardiologists. Can J Cardiol. 2018;34(1):92.e1–3.
Goldinger SM. A review of serious adverse effects under treatment with checkpoint inhibitors. Curr Opin Oncol. 2017;29(2):136–44.
Johnson DB, Balko JM, Compton ML, Chalkias S, Gorham J, Xu Y, et al. Fulminant myocarditis with combination immune checkpoint blockade. N Engl J Med. 2016;375(18):1749–55.
Wang DY, Okoye GD, Neilan TG, Johnson DB, Moslehi JJ. Cardiovascular toxicities associated with cancer immunotherapies. Curr Cardiol Rep. 2017;19(3):21.
Varricchi G, Galdiero MR, Marone G, Criscuolo G, Triassi M, Bonaduce D, et al. Cardiotoxicity of immune checkpoint inhibitors. ESMO Open. 2017;2(4):e000247.
Heinzerling L, Ott PA, Hodi FS, Husain AN, Tajmir-Riahi A, Tawbi H, et al. Cardiotoxicity associated with CTLA4 and PD1 blocking immunotherapy. J Immunother Cancer. 2016;4:50.
Mahmood SS, Fradley MG, Cohen JV, Nohria A, Reynolds KL, Heinzerling LM, et al. Myocarditis in patients treated with immune checkpoint inhibitors. J Am Coll Cardiol. 2018;71(16):1755–64.
Dasanu CA, Jen T, Skulski R. Late-onset pericardial tamponade, bilateral pleural effusions and recurrent immune monoarthritis induced by ipilimumab use for metastatic melanoma. J Oncol Pharm Pract. 2017;23(3):231–4.
Kushnir I, Wolf I. Nivolumab-induced pericardial tamponade: a case report and discussion. Cardiology. 2017;136(1):49–51.
Yun S, Vincelette ND, Mansour I, Hariri D, Motamed S. Late onset ipilimumab-induced pericarditis and pericardial effusion: a rare but life threatening complication. Case Rep Oncol Med. 2015;2015:1–5.
Wick W, Hertenstein A, Platten M. Neurological sequelae of cancer immunotherapies and targeted therapies. Lancet Oncol. 2016;17(12):e529–41.
Spain L, Walls G, Julve M, O’Meara K, Schmid T, Kalaitzaki E, et al. Neurotoxicity from immune-checkpoint inhibition in the treatment of melanoma: a single centre experience and review of the literature. Ann Oncol. 2017;28(2):377–85.
Kao JC, Liao B, Markovic SN, Klein CJ, Naddaf E, Staff NP, et al. Neurological complications associated with anti-programmed death 1 (PD-1) antibodies. JAMA Neurol. 2017;74(10):1216.
Williams TJ, Benavides DR, Patrice K-A, Dalmau JO, de Ávila ALR, Le DT, et al. Association of autoimmune encephalitis with combined immune checkpoint inhibitor treatment for metastatic cancer. JAMA Neurol. 2016;73(8):928.
Mancone S, Lycan T, Ahmed T, Topaloglu U, Dothard A, Petty WJ, et al. Severe neurologic complications of immune checkpoint inhibitors: a single-center review. J Neurol. 2018;265:1636–42.
Zimmer L, Goldinger SM, Hofmann L, Loquai C, Ugurel S, Thomas I, et al. Neurological, respiratory, musculoskeletal, cardiac and ocular side-effects of anti-PD-1 therapy. Eur J Cancer. 2016;60:210–25.
Makarious D, Horwood K, Coward JIG. Myasthenia gravis: an emerging toxicity of immune checkpoint inhibitors. Eur J Cancer. 2017;82:128–36.
Gonzalez NL, Puwanant A, Lu A, Marks SM, Živković SA. Myasthenia triggered by immune checkpoint inhibitors: new case and literature review. Neuromuscul Disord. 2017;27(3):266–8.
Sznol M, Postow MA, Davies MJ, Pavlick AC, Plimack ER, Shaheen M, et al. Endocrine-related adverse events associated with immune checkpoint blockade and expert insights on their management. Cancer Treat Rev. 2017;58:70–6.
Cukier P, Santini FC, Scaranti M, Hoff AO. Endocrine side effects of cancer immunotherapy. Endocr Relat Cancer. 2017;24(12):T331–47.
Ryder M, Callahan M, Postow MA, Wolchok J, Fagin JA. Endocrine-related adverse events following ipilimumab in patients with advanced melanoma: a comprehensive retrospective review from a single institution. Endocr Relat Cancer. 2014;21(2):371–81.
Caturegli P, Di Dalmazi G, Lombardi M, Grosso F, Larman HB, Larman T, et al. Hypophysitis secondary to cytotoxic T-lymphocyte-associated protein 4 blockade: insights into pathogenesis from an autopsy series. Am J Pathol. 2016;186(12):3225–35.
Kapke J, Shaheen Z, Kilari D, Knudson P, Wong S. Immune checkpoint inhibitor-associated type 1 diabetes mellitus: case series, review of the literature, and optimal management. Case Rep Oncol. 2017;10:897–909.
Martin-Liberal J, Furness AJ, Joshi K, Peggs KS, Quezada SA, Larkin J. Anti-programmed cell death-1 therapy and insulin-dependent diabetes: a case report. Cancer Immunol Immunother. 2015;64(6):765–7.
Johncilla M, Misdraji J, Pratt DS, Agoston AT, Lauwers GY, Srivastava A, et al. Ipilimumab-associated Hepatitis: clinicopathologic characterization in a series of 11 cases. Am J Surg Pathol. 2015;39(8):1075–84.
Kim KW, Ramaiya NH, Krajewski KM, Jagannathan JP, Tirumani SH, Srivastava A, et al. Ipilimumab associated hepatitis: imaging and clinicopathologic findings. Invest New Drugs. 2013;31(4):1071–7.
De Martin E, Michot J-M, Papouin B, Champiat S, Mateus C, Lambotte O, et al. Characterization of liver injury induced by cancer immunotherapy using immune checkpoint inhibitors. J Hepatol. 2018;68(6):1181–90.
Uslu U, Agaimy A, Hundorfean G, Harrer T, Schuler G, Heinzerling L. Autoimmune colitis and subsequent CMV-induced hepatitis after treatment with ipilimumab. J Immunother Hagerstown Md 1997. 2015;38(5):212–5.
Imafuku K, Yoshino K, Yamaguchi K, Tsuboi S, Ohara K, Hata H. Successful treatment of sudden hepatitis induced by long-term Nivolumab administration. Case Rep Oncol. 2017;10(1):368–71.
Postow MA, Chesney J, Pavlick AC, Robert C, Grossmann K, McDermott D, et al. Nivolumab and ipilimumab versus ipilimumab in untreated melanoma. N Engl J Med. 2015;372(21):2006–17.
Michot J-M, Ragou P, Carbonnel F, Champiat S, Voisin A-L, Mateus C, et al. Significance of immune-related lipase increase induced by antiprogrammed death-1 or death ligand-1 antibodies: a brief communication. J Immunother Hagerstown Md 1997. 2017;41(2):84–5.
Goldinger SM, Stieger P, Meier B, Micaletto S, Contassot E, French LE, et al. Cytotoxic cutaneous adverse drug reactions during anti-PD-1 therapy. Clin Cancer Res. 2016;22(16):4023–9.
Carlos G, Anforth R, Chou S, Clements A, Fernandez-Peñas P. A case of bullous pemphigoid in a patient with metastatic melanoma treated with pembrolizumab. Melanoma Res. 2015;25(3):265–8.
Naidoo J, Schindler K, Querfeld C, Busam K, Cunningham J, Page DB, et al. Autoimmune bullous skin disorders with immune checkpoint inhibitors targeting PD-1 and PD-L1. Cancer Immunol Res. 2016;4(5):383–9.
Murakami N, Motwani S, Riella LV. Renal complications of immune checkpoint blockade. Curr Probl Cancer. 2017;41(2):100–10.
Lute KD. Human CTLA4 knock-in mice unravel the quantitative link between tumor immunity and autoimmunity induced by anti-CTLA-4 antibodies. Blood. 2005;106(9):3127–33.
Cortazar FB, Marrone KA, Troxell ML, Ralto KM, Hoenig MP, Brahmer JR, et al. Clinicopathological features of acute kidney injury associated with immune checkpoint inhibitors. Kidney Int. 2016;90(3):638–47.
Shirali AC, Perazella MA, Gettinger S. Association of acute interstitial nephritis with programmed cell death 1 inhibitor therapy in lung cancer patients. Am J Kidney Dis. 2016;68(2):287–91.
Izzedine H, Gueutin V, Gharbi C, Mateus C, Robert C, Routier E, et al. Kidney injuries related to ipilimumab. Invest New Drugs. 2014;32(4):769–73.
Khan U, Ali F, Khurram MS, Zaka A, Hadid T. Immunotherapy-associated autoimmune hemolytic anemia. J Immunother Cancer. 2017;5:15.
Tardy MP, Gastaud L, Boscagli A, Peyrade F, Gallamini A, Thyss A. Autoimmune hemolytic anemia after nivolumab treatment in Hodgkin lymphoma responsive to immunosuppressive treatment. A case report. Hematol Oncol. 2017;35(4):875–7.
Palla AR, Kennedy D, Mosharraf H, Doll D. Autoimmune hemolytic anemia as a complication of nivolumab therapy. Case Rep Oncol. 2016;9(3):691–7.
Brahmer JR, Lacchetti C, Schneider BJ, Atkins MB, Brassil KJ, Caterino JM, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol. 2018;36(17):1714–68.
Champiat S, Lambotte O, Barreau E, Belkhir R, Berdelou A, Carbonnel F, et al. Management of immune checkpoint blockade dysimmune toxicities: a collaborative position paper. Ann Oncol. 2016;27(4):559–74.
Cramer P, Bresalier RS. Gastrointestinal and hepatic complications of immune checkpoint inhibitors. Curr Gastroenterol Rep. 2017;19(1):3.
Kimura T, Fukushima S, Miyashita A, Aoi J, Jinnin M, Kosaka T, et al. Myasthenic crisis and polymyositis induced by one dose of nivolumab. Cancer Sci. 2016;107(7):1055–8.
Abdel-Wahab N, Shah M, Suarez-Almazor ME. Adverse events associated with immune checkpoint blockade in patients with cancer: a systematic review of case reports. Nishikawa H, éditeur. PLoS ONE. 2016;11(7):e0160221.
Bellmunt J, de Wit R, Vaughn DJ, Fradet Y, Lee J-L, Fong L, et al. Pembrolizumab as second-line therapy for advanced urothelial carcinoma. N Engl J Med. 2017;376(11):1015–26.
Carbone DP, Reck M, Paz-Ares L, Creelan B, Horn L, Steins M, et al. First-line Nivolumab in stage IV or recurrent non-small-cell lung cancer. N Engl J Med. 2017;376(25):2415–26.
Eggermont AMM, Blank CU, Mandala M, Long GV, Atkinson V, Dalle S, et al. Adjuvant pembrolizumab versus placebo in resected stage III melanoma. N Engl J Med. 2018;378(19):1789–801.
Ferris RL, Blumenschein G, Fayette J, Guigay J, Colevas AD, Licitra L, et al. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N Engl J Med. 2016;375(19):1856–67.
Hellmann MD, Ciuleanu T-E, Pluzanski A, Lee JS, Otterson GA, Audigier-Valette C, et al. Nivolumab plus ipilimumab in lung cancer with a high tumor mutational burden. N Engl J Med. 2018;378(22):2093–104.
Long GV, Weber JS, Larkin J, Atkinson V, Grob J-J, Schadendorf D, et al. Nivolumab for patients with advanced melanoma treated beyond progression: analysis of 2 phase 3 clinical trials. JAMA Oncol. 2017;3(11):1511.
Wolchok JD, Chiarion-Sileni V, Gonzalez R, Rutkowski P, Grob J-J, Cowey CL, et al. Overall survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. 2017;377(14):1345–56.
Authors’ contributions
VL, APM, FV wrote the manuscript; MD performed statistical tests; EA, AVD and PRB review the manuscript and proposed substantial modifications. All authors read and approved the final manuscript.
Acknowledgements
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
Not applicable.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Not applicable.
Funding
No source of funding.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional file
Additional file 1: Fig. S1.
Frequencies of grade III and IV IrAE in studies: meta-analysis of randomized control trials including CTLA4i (upper plot), CTLA4i + PD1i/PDL1i (middle plot), or PD1i/PDL1i (lower plot). The forest plots represent the frequencies of IrAE organ by organ. a Severe dermatologic IrAE; b severe endocrine IrAE; c severe myocardiac IrAE; d severe hematological IrAE; e severe renal IrAE; f severe peripheral neuropathic IrAE. References: [3,4,5, 13, 16,17,18, 24, 33, 34, 40, 60, 71, 75, 88,89,90,91,92,93,94,95].
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Lemiale, V., Meert, AP., Vincent, F. et al. Severe toxicity from checkpoint protein inhibitors: What intensive care physicians need to know?. Ann. Intensive Care 9, 25 (2019). https://doi.org/10.1186/s13613-019-0487-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13613-019-0487-x