
Abstract
Background
Inadequate nutrient consumption causes protein energy malnutrition and micronutrient deficiencies and related consequences, including poor physical growth and intellectual development. However, literatures showing quantitative measurement of dietary intake of children are limited in Ethiopia. Therefore, this study investigated nutrient consumption and associated factors among school age children (7–9 years) in Dewa Cheffe District, northeast of Ethiopia.
Methods
A community based cross-sectional study was conducted from November to December, 2015 in Dewa Cheffe District. A multistage sampling technique was used to select 605 study subjects. Pre-tested and structured questionnaire was used to collect data. A 24-h dietary recall with portion size estimation method was used to assess nutrient consumption of school age children. Multivariable logistic regression analysis was fitted to identify factors associated with inadequate energy intake. adjusted odds ratio (AOR) with corresponding 95% confidence interval was computed to show the strength of association. In multivariable analysis, a P value of < 0.05 was used to declare statistically significance.
Results
A total of 600 school age children were included in the study. About 29% [95%, CI 21.9, 36.1] of study participants had inadequate energy intake. The result of multivariable analysis revealed that, children who were belonged to a female headed households [AOR = 3.65; 95% CI 1.20, 11.04] and family size of six and above [AOR = 14.42; 95% CI 4.65, 44.67] were found with increased odds of inadequate energy consumption. In contrast, decreased odds of inadequate energy consumption were observed among children whose mothers were housewives [AOR = 0.32; 95% CI 0.11, 0.52].
Conclusions
In this study, one-third of school children had inadequate energy consumption. Female headed households, being in the larger family size and housewives mother were significantly associated with inadequate energy consumption. Therefore, giving special focus to female headed households, large family and outdoor worker mothers will help to improve dietary intake of children.
Similar content being viewed by others


Background
Children are building blocks of the future generation [1] and their health, physical growth, and intellectual development fundamentally depends on adequate provision of nutrients [1,2,3,4]. Researchers also showed that school performance of children depends on their optimal nutritional status [3, 4]. On the other hand, inadequate nutrient consumption is strongly associated with protein energy malnutrition and micronutrient deficiencies [5, 6]. About 20–80% of school children in developing countries are suffering from poor nutrient consumption and undernutrition [7, 8]. In Ethiopia school-age children are affected by a wide range of nutrition related problems, mainly due to inadequate food consumption, which constrains their ability to thrive and benefit from education [9,10,11,12,13]. Undernutrition is contributed to 28% of child mortality, loss of cognitive performance, higher medical expenses and loss of 55.5 billion birr per annum [14, 15].
With due cognizant of the adverse consequences of undernutrition, the country designed and has been implemented different nutritional intervention with the major objective of ensuring optimal feeding practices so as to address the higher magnitude of undernutrition thereby mortality [16, 17]. However, the recent National Food Consumption Survey revealed that nutrient inadequacy was a major health concern and the average total calorie intake of children was below recommended intakes in all regions of the country [18]. Likewise, the study reported from the Western part Ethiopia, Nekemtie District, demonstrated that about 76.42% of school age children had inadequate energy intake, and the consumption of other nutrients was also found as less than the recommended dietary allowance (RDA) [19].
The result of different studies conducted elsewhere noted that inadequate energy and nutrient intake was associated with various factors, but mainly related to the socio-demographic and economic characteristics. Accordingly, low socioeconomic status [20,21,22], unemployment [20] and illiteracy status of the mothers [20,21,22,23], large family size [20], food insecurity [24], nuclear families type [20] and sex of children [7, 20, 25] are factors which negatively influences adequate nutrient consumption of children.
Mostly undernutrition like stunting at school age is associated with poor nutrition since early childhood and the degree of stunting tends to increase throughout the school-age years. However, children can exhibit catch-up growth if their environment improves. Therefore, interventions in school-age children can supplement efforts in preschool years to reduce levels of stunting and related effects on children’s health and education [26]. Though evidences showing the dietary consumption of school children have a decisive role to tackle the adverse and functional consequences of poor dietary intake, literatures are scarce in Ethiopia. Hence, this study estimated inadequate energy intake and associated factors among school age children (7–9 years) in Dewa Cheffe District, northeast Ethiopia.
Methods
Study setting and design
A community based cross- sectional study was conducted from November to December, 2015 in Dewa Cheffe District. Dewa Cheffe is one of the seven districts of Oromia Zone in Amhara Regional State. The district is found 325 km away from Addis Ababa, the capital of Ethiopia. The district is divided into 21 Kebeles (the smallest administration unit). Based on the 2015/2016 the district Finance and Economic Development office projection, the total population is estimated at 141,529, and school children constitute 15.7% (22, 176) of the total. Livestock and crop productions are important sources of livelihoods in the district. Sorghum, Teff, Maize, Barley and Wheat are the main crops cultivated in the setting.
Sample size and sampling procedure
A randomly selected school aged children (7–9 years) living in Dewa Chefe District were included in the study, however critically ill and those with already established Diabetes Mellitus were excluded from the study. The required sample size was determined by using single population proportion by taking into account of the following assumptions: expected prevalence of adequate energy consumption as 50% (since there was no prior study in the area), 95% level of confidence and 5% margin of error. In addition, a 5% non-response rate and design effect of 1.5 was anticipated to obtain the final sample size of 605.
A multi-stage stratified sampling followed by a systematic random sampling technique was employed to reach the study subjects. The kebeles were stratified into urban and rural kebeles. Of the total twenty-one kebeles, five (one urban and four rural) were selected by lottery method. The total number of households with school age children was accessed from the District Administration Office. The numbers of households with eligible children in the selected kebeles were determined proportionally. In addition, the sampling interval was calculated, and households with eligible children were selected using a systematic random sampling technique. For households with more than one study subject, only one was selected using lottery method. When mother–child pairs were not available at the time of data collection, two repeated visits were made.
Data collection procedures
Data was collected using pretested, structured and interviewer administered questionnaire consisted of socio-demographic and dietary related information. Dietary intake information was collected using a semi-quantitative food frequency questionnaire (FFQ) developed based on internationally recognized multiple pass method described by Gibson and Ferguson [27]. Initially, English version questionnaire was translated into Amharic and then back translated to English by language and Public Health experts to maintain its consistency. Six clinical nurses and two Health Officers were recruited as data collector and supervisor, respectively. Two days training was given for data collectors and supervisors. Prior to data collection, the questionnaire was pretested on 5% (30) of respondents in one Kebele which was not included in the sample but with similar setting to evaluated acceptability and applicability of procedures and tools.
Measurement of nutrient intake
Nutrient intake of children was collected using 24-hour recall method. Each interview considered a stepwise series of questions. In addition, commonly used household utensils, food substitutes and pictures of most frequently consumed foods in the study area were used to improve accuracy of dietary measurement and minimize recall bias. As recommended by Gibson and Ferguson [27], the dietary interviews for this survey were structured in “Four Passes Method” to enhance participants memory. In the first place mothers were asked to report all food items consumed by the child in the previous 24 h. Secondly, portion size of food was estimated and then in case of mixed dish detail information regarding the ingredients of food was obtained. Finally, verification of the collected dietary information was done. The average portion size for each type of food was determined using commonly used utensils. A digital food scale was used to measure the amount of food consumed and of ingredients used in food preparation. Moreover, the method of preparation was also considered. After calculating the child’s net consumption, the energy and nutrient contents or value of the food item was determined using the Ethiopian Food Composition Table Part IV [28]. The data were subsequently converted into the amount of energy and nutrient intake per individual per day. Finally, the nutrient consumption was compared with the estimated average requirements or Intake (EAR) or recommended dietary allowance (RDA) for National Institute of Nutrition (ICMR, 2004). Nutrient adequacy was expressed as ‘percent of adequacy’ by comparing nutrient intake of the children to RDA. ‘Adequate energy intake’ was ascertained if a child had nutrient intake of greater than or equal to estimated average requirements (EAR), whereas ‘inadequate energy intake’ was defined as nutrient intake of lower than EAR. Nutrient intake greater than or equal to Recommended Daily Allowance (RDA) was considered as ‘Adequate intake’ while nutrient intake below the RDA was classified as ‘Inadequate Intake’. Dietary diversity was estimated through classifying the reported food items into seven food groups, as starchy staples (grains, roots, and tubers); legumes, nuts and seeds; vitamin-A rich fruits and vegetables; other fruits and vegetables; egg; dairy products (milk, yoghurt, and cheese); and flesh foods (meat, fish, poultry, and organ meats) [29]. Furthermore, mothers were requested to estimate the frequency of consumption of the above food groups.
Household wealth index was computed using a composite indicator for urban and rural residents by considering the following properties; selected household assets, and size of agricultural land. Principal component analysis was performed to categorize the household wealth index into lowest, middle and highest.
Data management and analysis
Data were entered into Epi-info version 3.5.1 and exported to SPSS version 20 for analysis. Descriptive statistics using frequencies and proportions were used to summarize variables. Binary logistic regression model was fitted. Variables with P-value < 0.2 in bivariable analysis were entered into multivariable analysis. Both Crude Odds Ratio (COR) and adjusted odds ratio (AOR) with corresponding 95% confidence interval (CI) were computed to show the strength of association. In multivariable analysis, variables with P-value < 0.05 were considered as statistically significant.
Results
Socio-demographic and economic characteristics
A total of 600 mother–child pairs were interviewed with the response rate of 99.2%. About 60.2% of children were males. Majority (89.7%) of the households were headed by men. Moreover, about two-third (65.7% and 57.8%, respectively) of mothers were housewives and illiterate (Table 1).
Dietary diversity, nutrient and energy intake of children
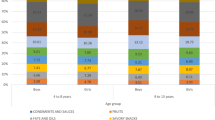
The dietary habits of children were mainly based on cereals (100%) and legumes (100%). Only few of participants consumed milk products (10.8%), meat (11.8%), and green leafy vegetables (GLV) (14%). Furthermore, none of the children ate roots and tubers (Fig. 1). Almost all (98%) and three-fourth (75%) of children consumed sugar and fruits fortnightly, respectively. However, about one-quarter (25%) and one-third (32.2%) of children didn’t consume milk and GLV over the past 1 month prior to the date of survey, respectively (Table 2).

Dietary diversity of school aged children in Dewa Cheffe District, northeast Ethiopia, 2015 (n = 600)
Almost all of children took protein (99.0%) and iron (98.5%) at the amount greater than or equal to their RDA. However, only half of the study participants were found with adequate intake of Calcium (56.0%), Niacin (50.7%) and β-carotene (44.5%) (Table 3).
In this community, there was no statistical difference in the mean energy consumption among males (1375.81 ± 211.82) and females (1366.62 ± 294.51). But, mean protein (32.32 gm versus 25.58 gm) and Calcium (381.54 mg versus 270.81 mg) intake was significantly higher in males than females at a P-value of < 0.05 (Table 4). Concerning energy consumption, about 29.0% [95%, CI 21.9, 36.1] of children had inadequate energy intake (took < of their EAR), whereas 71% of children had adequate energy consumption (took ≥ of their EAR).
Factors associated with inadequacy energy consumption
Both bivariate and multivariate logistic regressions were done; the result of multivariate analysis revealed that, children who were belonged from households headed by females [AOR = 3.65; 95% CI 1.20, 11.04] and family size of six and above [AOR = 14.42; 95% CI 4.65, 44.67] were found with increased odds of inadequate energy consumption. In contrast, decreased odds of inadequate energy consumption was observed among children whose mothers were housewives [AOR = 0.32; 95% CI 0.11, 0.52] (Table 5).
Discussions
The present study revealed that, about 29.0% of children had inadequate energy intake which slightly higher than the finding from Kenya (17.3%) [30]. However, the result is lower than the previous studies in western Ethiopia (76.42%) [19] and India (62%) [20]. The observed discrepancy may be due to the difference in the study setting, in which the current study was conducted in the rural area where most of the residents support their livelihood through agricultural production of crops. In addition, the difference could be related to seasonal variation in market availability of food. In Ethiopia, from November to December (study period) agricultural products (crops) were harvested and more available and affordable in the market which in turn positively affects the household’s per capita food availability and food intake. However, the current finding was slightly higher than the finding from Kenya (17.3%) [30].
Besides, the study revealed significant difference in energy consumption with sex of the children which was consistent with former report in the rural Bangladesh [31]. Obliviously, there is cultural bias favoring males in Ethiopia and other developing countries. Children are considered as important source of future labor on the family farm, and expected to provide economic and social security for their parents when their father is debilitated or get old or in times of distress. Consequently, males are prioritized to by parents while serving food, including the nutritious one.
The result of the adjusted analysis revealed that, the likelihood of inadequate energy consumption was higher among children who lived in households headed females and larger family size. However, decreased odds of inadequate energy consumption were common among children of housewife mothers as compared to children of the self- employed mothers. Similar findings were reported in India [20] and Ghana [23]. This might be due to housewife mothers had better time to care and feed their child as compared to outdoor worker mothers.
Being in the large family size (≥ 5) was associated with increased odds of inadequate energy consumption among school aged children compared to their counter parts who belonged from smaller family size (≤ 3). Similar finding was reported in India [20]. Large family poses additional challenges to the household to secure the per capita food availability. The condition worsens in the countries where unemployment rate is high which increases the socio-economic dependency of the household members in the country at large [14].
The odds of in adequate energy consumption were higher among children living under households headed females. This could be explained by in most of developing countries literacy rate was low among women’s, as a result they were engaged in non-professional and low income generating activities. Furthermore, they are also responsible to take care their child and the household members at large which ultimately decreases the time spent to work. This all conditions negatively affects their income and the amount of money spent for purchasing food as compared to their male counterparts.
This study quantitatively estimated nutrient and energy consumption of children. Also, a multiple pass recall method was used to enhance memory of respondents. Despite these methodological strengths, the study is not free from recall bias while qualitatively estimating dietary consumption of children.
Conclusions
This study showed that nutrient and energy inadequacy was high among children in Dawa Chefe District. Moreover, sex of household head, family size and occupational status of the mother were significantly associated with energy consumption of children. Therefore, attention has to be paid on households headed by female, outdoor worker mothers and large families to improve energy consumption of children. Also, current efforts focused on enhancing micronutrient intake of children should be strengthened.
Abbreviations
- AOR:
-
adjusted odds ratio
- CI:
-
confidence interval
- COR:
-
crude odds ratio
- EAR:
-
estimated average requirements
- FFQ:
-
Food Frequency Questionnaire
- RDA:
-
recommended dietary allowance
- GLV:
-
green leafy vegetables
- SD:
-
standard deviation
References
Buttriss J. Nutrition, health and school children. Nutr Bull. 2002;2(7):275–316.
Jomaa LH, McDonnell E, Probart C. School feeding programs in developing countries: impacts on children’s health and educational outcomes. Nutr Rev. 2011;69:83–98.
Rimaz S, Moghtaderi A, Shidfar F, Poor Malek F. Prevalence and determinants of protein-energy malnutrition among children under the age of 5 in Savojbolagh (2002–2003). Razi J Med Sci. 2005;12(48):97–105.
World Health Organization. Nutrition for health and development: a global agenda for combating malnutrition. Geneva: WHO; 2000.
Ochola S, Masibo PK. Dietary intake of schoolchildren and adolescents in developing countries. Ann Nutr Metab. 2014;64(Suppl. 2):24–40.
Handa R, Ahamad F, Kesari KK, Prasad R. Assessment of nutritional status of 7–10 years school going children of Allahabad district: a review. Middle-East J Sci Res. 2008;3(3):109–15.
Vandana S: Nutritional Assessment of Rural School-Going Children (7–9 Years) of Hisar District, Haryana. 2012.
Shivaprakash N, Joseph RB. Nutritional status of rural school going children of Mandya District, Karnataka. Int J Sci Study. 2014;2(2):39–43.
Hall A, Kassa T, Demissie T, Degefie T, Lee S. National survey of the health and nutrition of school children in Ethiopia. Trop Med Int Health. 2008;13(15181526):8.
Mekasha A, Zerfu M. Prevalence of anemia among school children in Addis Ababa. Ethiop Med J. 2009;47:129–33.
Reji P, Belay G. Intestinal parasitic infections and malnutrition amongst first-cycle primary school children in Adama, Ethiopia. Afr J Prim Health Care Fam Med. 2011;. https://doi.org/10.4102/phcfm.v3i1.198.
Mekonnen H, Tadesse T. Malnutrition and its correlates among rural primary school children of Fogera District, Northwest Ethiopia. J Nutr Disorders Ther. 2013;12:2161.
Situation Analysis on School Health and Nutrition in Ethiopia, Ministry of Education (MoE), September 2008, Addis Ababa.
Csa I. Ethiopia Demographic and Health Survey 2011. Addis Ababa: Central Statistical Agency and ICF International; 2012.
State Minister of Health. Federal Democratic Republic of Ethiopia: The Cost of Hunger in Ethiopia. Addis Ababa: The Social and Economic Impact of Child Undernutrition in Ethiopia; 2009.
Government of the Federal Democratic and Republic of Ethiopia: National School Health and Nutrition Strategy: Ministry of education, Addis Ababa; 2012.
Government of the Federal Democratic and Republic of Ethiopia: National Nutrition Program June 2013–June 2015.
Ethiopian Public Health Institute. Report on National Food Consumption survey. Addis Ababa; 2013.
Preetie R, Ghate L, Preetie RG. Food consumption patterns and malnourished Ethiopian children: is there a link? Food Policy. 2014;4(2):8–15.
Sameena S. Determinates of adequacy of nutrient consumption among rural school-aged children. Asian Pac J Health Sci. 2014;1(3):227–32.
Flores M, Macías N, Rivera M, Barquera S, Hernández L, García-Guerra A, Rivera JA. Energy and nutrient intake among Mexican school-aged children, Mexican National Health and Nutrition Survey 2006. Salud pública de México. 2009;51:S540–50.
Kulsum A, Lakshmi J, Prakash J. Food intake and energy protein adequacy of children from an urban slum in Mysore, India–a qualitative analysis. Mal J Nutr. 2008;14(2):163–72.
Doku D, Koivusilta L, Raisamo S, Rimpelä A. Socio-economic differences in adolescents’ breakfast eating, fruit and vegetable consumption and physical activity in Ghana. Public Health Nutr. 2013;16(05):864–72.
Nnakwe N, Onyemaobi G. Prevalence of food insecurity and inadequate dietary pattern among households with and without children in imo State Nigeria. Int J Sociol Anthropol. 2013;5(9):402.
Chen LC, Huq E, d’Souza S: Sex bias in the family allocation of food and health care in rural Bangladesh. Population and development review 1981:55-70.
Frongillo EAJ. Causes and etiology of stunting. Am Soc Nutr Sci J Nutr. 1999;129:529–30.
Gibson RS, Ferguson EL. An interactive 24-hour recall for assessing the adequacy of iron and zinc intakes in developing countries. (Harvest Plus, 2008).
Ethiopian Health and Nutrition Research Institute. Food composition Table for use in Ethiopia: Report part IV. Addis Ababa: Food and Agricultural Organization; 1998.
World Health Organization: Indicators for assessing infant and young child feeding practices part 3: country profiles. 2010.
Mwaniki E, Makokha A. Nutrition status and associated factors among children in public primary schools in Dagoretti, Nairobi, Kenya. Afr Health Sci. 2013;13(1):38–46.
Chen LC, Huq E, d’Souza S. Sex bias in the family allocation of food and health care in rural Bangladesh. Popul Dev Rev. 1981;38:55–70.
Authors’ contributions
Conceived and designed the experiments: ES AT LD TD MA KAG. Performed the experiments: ES. Analyzed the data: ES AT LD TD MA KAG. Wrote the paper: ES AT LD TD MA KAG. Approved the proposal with some revisions: ES AT LD TD MA KAG. All authors read and approved the final manuscript.
Acknowledgements
We are thankful to children, interviewed families, data collectors, and supervisors of this study.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
Data will be made available upon requesting the primary author.
Consent to publish
Not applicable.
Ethics approval and consent to participate
Ethical clearance was obtained from the Ethical Review Board of University of Gondar (Ref No/IPH/2679/02/08). An Official letter of permission was obtained from Dewa Cheffe District Administration Office prior to data collection. The study participants were informed about the objective, risk and benefits of the study. Written consent was obtained from mothers or caregivers of the children. Participation was on voluntary basis. The participants’ confidentiality of information was guaranteed by leaving out names and any forms of personal identification in the questionnaire.
Funding
No funding was obtained for this study.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Additional file
Additional file 1.
Questionaire.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Seid, E., Derseh, L., Derso, T. et al. Nutrient consumption and associated factors among school age children in Dewa Chefe District, northeast Ethiopia: a cross-sectional study. BMC Res Notes 11, 669 (2018). https://doi.org/10.1186/s13104-018-3773-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13104-018-3773-z