
Abstract
Background
Cardiovascular disease is the cause of more than 50% of mortalities globally, and this rate has grown by 8.6% since the 60 s. One of the risk factors associated with cardiovascular disease and its resulting mortality rate is the metabolic syndrome. Different studies have reported inconsistent rates for the metabolic syndrome. However, no comprehensive study has been conducted to combine the results of existing studies. Thus, the present study was performed with the aim of determining the prevalence of metabolic syndrome among cardiovascular patients in Iran through a systematic review and meta-analysis.
Method
: In this review study, the Scientific Information Database, Google Scholar, Science Direct, Scopus, PubMed, and Web of Science (ISI), databases were searched from January 2005 and until May 2020, to identify and extract related articles. To conduct the analysis, a random effects model was used, and the heterogeneity of the studies was examined using the I2 index. Data analysis was performed within Comprehensive Meta-Analysis (version 2) software.
Results
The prevalence of metabolic syndrome in cardiovascular patients in Iran in the 27 papers examined with a sample size of 44,735 patients was 34.2% (95% CI: 26.8–42.6%). A sensitivity analysis was performed to ensure the stability of the results, these results show that by omitting the prevalence from each study, the overall prevalence (34.2%) does not change significantly. the highest prevalence of metabolic syndrome in studies conducted in the period between 2015 and 2020, and this was reported as 55.3 (95% CI: 47.9–62.3) and the highest prevalence of metabolic syndrome in studies conducted in the methods of diagnosis IDF, and the rate was reported as 48 (95% CI: 36.5–59.8). based on meta-regression as the year of research increased, the prevalence of metabolic syndrome in cardiovascular patients in Iran also increased. However, with the increase in sample size, this prevalence decreased (p < 0.05).
Conclusions
The results of this study indicate that metabolic syndrome is high in cardiovascular patients in Iran. Accordingly, by understanding its etiology and supervision at all levels, suitable solutions could be offered by providing feedback to hospitals.
Similar content being viewed by others


Background
Cardiovascular disease generally refers to conditions that involve narrowed or blocked blood vessels that can lead to a heart attack, chest pain (angina) or stroke. Other heart conditions, such as those that affect your heart’s muscle, valves or rhythm, also are considered forms of heart disease [1,2,3,4].
Cardiovascular disease is the cause of more than 50% of mortalities in world, and this figure has grown by 8.6% since the 60 s [1, 2]. The mortality caused by cardiovascular disease in the US is higher than that resulting from cancer, accidents, and diabetes [3]. This disease affects the elderly more than the other age groups, such that 83% of those who die because of cardiovascular disease are above 65 years of age [2]. The World Health Organization (WHO) has predicted that, over the upcoming two decades, the mortality caused by cardiovascular disease may grow to 137% and 120% in men and women, respectively [4].
One of the risk factors associated with cardiovascular disease and its resulting mortality rate is metabolic syndrome [5, 6]. The individuals suffering metabolic syndrome are 3–5 times more likely to develop cardiovascular disease and die as a result, compared to non-affected individuals [7, 8]. Metabolic syndrome was initially referred to as hypertension, diabetes, and gout according to Reaven study in 1988; Gans study in 2006 also reported insulin resistance as the central characteristic of this disorder and called it the X syndrome [9, 10]. Metabolic syndrome increases the risk of cardiovascular disease in patients at any level of LDL [6,7,8,9].
The definitions proposed for metabolic syndrome are different in terms of execution as well as the boundary of their diagnosis. Nevertheless, abdominal obesity, hypertension, elevated glucose levels, and dyslipidemia exist in all definitions of the syndrome. Two definitions were previously proposed by the Adult Treatment Panel (ATPIII) [10, 11]. Recently, the International Diabetes Federation has presented a new definition for metabolic syndrome. In this definition, the waist circumference, which is different for various races, has been used as a major factor [12].
On the other hand, the dangerous role of metabolic syndrome in the incidence of coronary heart diseases (CHD) is increasing [13], which has developed into a major health problem in human societies [14]. Patients with cardiovascular disease need to pay close attention to their risk of catching other diseases, given the dangerous side effects of the disease, many of which are fatal. The most significant of these diseases is metabolic syndrome, which can double the effects of cardiovascular disease and increase its incidence [13,14,15].
CHD has been known as one of the major causes of mortality [15]. Nevertheless, the information around the relationship between metabolic syndrome based on different definitions and CHD [16], especially in developing countries is still unclear [17]. There is sparse information available about the relationship between each of the definitions of metabolic syndrome and the risk of incidence of CHD. For instance, for Europeans [18, 19], as well as American Hindus [20], metabolic syndrome based on the WHO and ATPIII definitions, has widely predicted the incidence of CHD.
In Iran, a high prevalence of metabolic syndrome has been reported [21]. The prevalence of metabolic syndrome in patients with cardiovascular disease in Isfahan was 1.9% [23], in Tehran 36.5% [24], and in the city of Arak, this rate was reported 7.5% [25].
Considering the effect of different factors on the prevalence of metabolic syndrome in cardiovascular patients and the lack of general statistics in this regard across Iran, we intended to perform our review study on the existing studies, and approximate the overall prevalence using suitable meta-analysis techniques. The goal was to achieve general statistics about the prevalence of metabolic syndrome in cardiovascular patients in Iran.
Method
The study population in this study are cardiovascular patients, and, we were looking for the prevalence of metabolic syndrome reported as an outcome.
In this systematic review and meta-analysis study, the prevalence of metabolic syndrome in cardiovascular patients in Iran was examined based on the studies published between January 2005 and May 2020. For this purpose, the papers published in national and international databases of Scientific Information Database, Google scholar, Science Direct, Scopus, PubMed, and Web of Science were searched through English or the Persian equivalents of the following keywords: prevalence, metabolic syndrome, cardiovascular, and Iran.
Cross-sectional studies were included, yet review papers, case-controls, cohort, and interventional studies were excluded from the list of articles. Duplicate publications and multiple publications from the same population were removed from the list of articles that had been prepared within the EndNote (version X7, for Windows, Thomson Reuters) reference management software.
Study selection
Initially, all papers that assessed the prevalence of metabolic syndrome in cardiovascular patients in Iran were collected. Then, the studies were examined, based on the inclusion and exclusion criteria. The exclusion criteria were irrelevant topics, case reports, interventional studies, duplicate studies, unclear methods, and lack of access to the full text of the paper. In order to reduce the bias, the search of the papers was performed independently by two reviewers (for the search process, examination of titles and abstracts, full-text assessment, data extraction, and Quality assessment); in case of disagreement between the two reviewers, that paper was examined by the head of the group. A total of 35 studies were included in the third stage, i.e. quality evaluation.
Quality evaluation of studies
The quality of the papers was assessed based on the selected and relevant items of a 22-item STROBE checklist. The fields of the checklist were study design, background and review of texts, place and time of study, outcomes, inclusion criteria, sample size, and statistical analysis. The papers that had fulfilled 6–7 items of the criteria were considered as high-quality papers, while those not satisfying two or 3–5 of the seven items were considered as low or medium-quality papers (methodological quality) articles respectively Accordingly, the maximum quality score that could be obtained from the checklist was 32; papers with a score of less than 14 were considered as low quality, and were therefore excluded from the study. [22]. In the present study, 27 papers were included in the systematic review and meta-analysis as medium or high quality articles, while eight studies which were assessed as low quality were removed.
Data extraction
All of the final papers introduced into the meta-analysis process were prepared for extraction using a different pre-prepared checklist. The checklist included: title of paper, name of first author, year of publication, place of study, sample size, prevalence of metabolic syndrome, and methodology.
Statistical analysis
Since the prevalence has a binomial distribution, the variance of prevalence was calculated using a binomial distribution variance formula. Additionally, to combine the value of prevalence across different studies, weighted average was used. To assess the heterogeneity of the selected studies, the I2 index test was used. To examine the publication bias, considering the large sample size of the studies included, the Begg’s (Begg and Mazumdar) test at the significance level of 0.1 was used, and the corresponding Funnel plots were constructed. To inspect the extent of effect of every individual study on the final outcome, sensitivity analysis test was utilized. Data analysis was performed within the Comprehensive Meta-Analysis (version 2) software.
Results
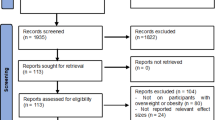
In this study, all of the studies conducted on the prevalence of metabolic syndrome in cardiovascular patients in Iran, published between January 2005 and until May 2020, were examined in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. In the preliminary research of the SID, PubMed, ScienceDirect, Scopus and ISI databases, 1440 papers were included. Articles satisfying the initial inclusion criteria were 105, after the elimination of 1335 duplicate articles. With detailed assessments of the articles and exclusion of further 8 studies (6 with unrelated outcomes, and 2 with unavailable data), finally, 27 articles entered the meta-analysis process (Fig. 1).

Flow diagram of study selection
The publication bias using the funnel plot and Begg and Mazumdar test at the significance level of 0.1, highlighting no publication bias in the present study (P = 0.297) (Fig. 2).

Funnel plot of the results related to the prevalence of metabolic syndrome cardiovascular patients in Iran
Based on the results obtained from the test (I2:99) and considering the heterogeneity of the selected studies, a random effects model was used for combining the studies and for the overall estimation of the prevalence.
The total number of participants selected in the meta-analysis was 4473. The characteristics of the studies included in the systematic review are shown in Table 1. The maximum and minimum prevalence of metabolic syndrome in cardiovascular patients were related to the studies by Anvari et al. 33.9% [29] and Aalami Harandi et al. 1.9% [23]. Based on the results of the study, the overall prevalence of metabolic syndrome in cardiovascular patients in Iran is 34.2% (95% CI: 26.8–42.6%) (Fig. 3).

Prevalence of metabolic syndrome in cardiovascular patients and confidence interval 95% in Iran
Sensitivity analysis
A sensitivity analysis was perfumed to ensure the stability of the results, after removing each study results and observing no change (Fig. 4).

Results of sensitivity analysis
The relationship between the year of conducting studies (P = 0.000), sample size (P = 0.000) and the prevalence of metabolic syndrome in Iranian cardiovascular patients was investigated using the meta-regression analysis. A significant difference was observed between the prevalence of metabolic syndrome and each of the two mentioned variables. As the year of research increased, the prevalence of metabolic syndrome in cardiovascular patients in Iran also increased. However, with the increase in sample size, this prevalence decreased (Figs. 5 and 6).

Meta-regression of the relationship between the sample size and prevalence of metabolic syndrome in cardiovascular patients in Iran

Meta-regression of the relationship between the year of the study and prevalence of metabolic syndrome in cardiovascular patients in Iran
Subgroup analysis based on year of study and methods of diagnosis of metabolic syndrome
Considering the results of Table 2 and the subgroup analysis based on year of study, the highest prevalence of metabolic syndrome in studies conducted in the period between 2015 to 2020, and this was reported as 55.3 (95% CI: 47.9–62.3)’ considering the subgroup analysis and based on the methods of diagnosis of metabolic syndrome, the highest prevalence of metabolic syndrome in studies conducted in the methods of diagnosis IDF, and the rate was reported as 48 (95% CI: 36.5–59.8).
Discussion
The present research was conducted with the aim of determining the prevalence of metabolic syndrome in cardiovascular patients in Iran. In the present systematic review, a total of 27 selected studies with a sample size of 43,735 subjects were investigated. For meta-analysis, using a random effects model, the total prevalence of metabolic syndrome in cardiovascular patients is found as 34.2% (95% CI: 26.8–42.6%). The high prevalence of metabolic syndrome in cardiovascular patients in Iran, as obtained in the present study, confirms the strong relationship between this syndrome and cardiovascular diseases. Based on the results of the present study, the maximum prevalence of metabolic syndrome in cardiovascular patients was associated with cardiac ischemic disease patients.
The prevalence was obtained as 73.2% by Rashidi among patients with type II diabetes [44]. Furthermore, in a research conducted by Aguilar et al. in 2003–2012 in the US, the total prevalence of metabolic syndrome was reported as 33% [45]; the figure obtained in Iran is higher than other countries which requires relevant attention.
The results of our study can follow prospective studies revealing that metabolic syndrome based on ATPIII definition and whether it is a predictor for CHD after modifying the variables of age, serum LDL, smoking, and history of premature CHD [43,44,45,46,47,48]. In NHANES III cross-sectional study on the American population above 50 years of age, metabolic syndrome based on ATPIII, in the presence of its components, did not present better prediction of CHD [49,50,51,52,53,54,55]. In contrast, in another study, metabolic syndrome based on ATPIII (and not WHO) was known as an independent risk factor for CHD after modifying the components of syndrome and cardiovascular risk factors [48]. Eventually, Ford, in a review study, found that metabolic syndrome based on ATPIII and WHO only plays an average role in predicting CHD (with relative risk of 1.7–1.9%) [56].
With regards to the effect of year of study and the prevalence of metabolic syndrome in cardiovascular patients in Iran, it was observed that this prevalence has an ascending trend among Iranian patients. Thus, interventions should be put in place. These interventions should result in a change of lifestyle, regularly controlling blood sugar and lipid levels of patients to prevent the disease and its associated complications. In addition to this, as metabolic syndrome is preventable in the first place, and, and to prevent or control complications, cardiovascular patients should receive complete training on the disease and the ways for preventing its complications. Moreover, it is important to note that through early diagnosis of complications, the disease can be treated and controlled.
When assessing the findings of this study, the current limitations should also be mentioned. The most important limitation of this study was that its papers were cross-sectional; prospective studies are required to investigate the relationship between different definitions of metabolic syndrome and CHD. Secondly, considering the high prevalence of diabetes [57] and obesity [58,59,60] in our Country, it seems that the reported prevalence of metabolic syndrome and CHD has been underestimated in this study [23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42]. One of the major strengths of this work was the usage of a large sample size of patients with cardiovascular disease in Iran, thus enhancing the generalizability of our findings.
Considering the high prevalence of metabolic syndrome in cardiovascular patients in Iran, it is suggested that physicians should pay more attention to the symptoms of this disease. Additionally, training should be offered through relevant platforms and media to raise the awareness of individuals, to promote early diagnosis of the condition. Furthermore, considering the prevalence of metabolic syndrome in cardiovascular patients in other parts of the world, further studies should be conducted in order to identify the prevalence of this condition worldwide.
Limitations
One of the most important limitations of the present study is the lack of access to the full text of some studies due to their low quality and high heterogeneity of studies.
Conclusions
The results of this study suggest that the prevalence of metabolic syndrome in cardiovascular patients in Iran is high. Accordingly, to improve this situation, to find the etiology, and for supervision at all levels, suitable solutions should be offered by giving feedback to hospitals.
Availability of data and materials
Datasets are available through the corresponding author upon reasonable request.
Abbreviations
- SID:
-
Scientific Information Database.
- WHO:
-
World Health Organization.
- ATPIII:
-
Adult Treatment Panel III.
- IDF:
-
International Diabetic Federation.
- STROBE:
-
Strengthening the Reporting of Observational Studies in Epidemiology.
- LDL:
-
Low-Density Lipoprotein.
- NHANES III:
-
The Third National Health and Nutrition Examination Survey.
- CHD:
-
Coronary Heart Diseases.
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
References
Dastoorpoor M, Sekhavatpour Z, Masoumi K, Mohammadi MJ, Aghababaeian H, Khanjani N, Hashemzadeh B, Vahedian M. Air pollution and hospital admissions for cardiovascular diseases in Ahvaz, Iran. Sci Total Environ. 2019;652:1318–30.
Sicard P, Omidi Khaniabadi Y, Perez S, Gualtieri M, De Marco A. Effect of O 3, PM 10 and PM 2.5 on cardiovascular and respiratory diseases in cities of France, Iran and Italy. Environ Sci Pollut Res Int. 2019;26(31):32645–65.
Cortes-Bergoderi M, Thomas RJ, Albuquerque FN, Batsis JA, Burdiat G, Perez-Terzic C, Trejo-Gutierrez J, Lopez-Jimenez F. Validity of cardiovascular risk prediction models in Latin America and among Hispanics in the United States of America: a systematic review. Revista Panamericana de Salud Pública. 2012;32(2):131–9.
Thrift AG, Thayabaranathan TH, Howard G, Howard VJ, Rothwell PM, Feigin VL, Norrving B, Donnan GA, Cadilhac DA. Global stroke statistics. 2017;12(1):13–32.
Jahangiry L, Abbasalizad Farhangi M, Rezaei F. Framingham risk score for estimation of 10-years of cardiovascular diseases risk in patients with metabolic syndrome. J Health Popul Nutr. 2017;36(1):36.
Julibert A, Del Mar Bibiloni M, Bouzas C, Martínez-González MA, Salas-Salvadó J. and et al. Association with Components of the Metabolic Syndrome in a Mediterranean Population at High Cardiovascular Risk. Nutrients. 2019;11(7):1493.
Kothiwala SK, Khanna N, Tandon N, Naik N, Sharma VK, Sharma S, Sreenivas V. Prevalence of metabolic syndrome and cardiovascular changes in patients with chronic plaque psoriasis and their correlation with disease severity: A hospital-based cross-sectional study. Indian J Dermatol Venereol Leprol. 2016;82(5):510–8.
Teresa Timóteo A, Mota Carmo M, Soares C, Cruz Ferreira R. Is metabolic syndrome a prognostic marker in patients at high cardiovascular risk? A long-term cohort study. Rev Port Cardiol. 2019;38(5):325–32.
Gans RO. The metabolic syndrome, depression, and cardiovascular disease: interrelated conditions that share pathophysiologic mechanisms. Medical Clinics. 2006;90(4):573–91.
Bertoni AG, Bonds DE, Steffes S, Jackson E, Crago L, Balasubramanyam A, Chen H, Goff DC Jr. Quality of cholesterol screening and management with respect to the National Cholesterol Education’s Third Adult Treatment Panel (ATPIII) guideline in primary care practices in North Carolina. Am Heart J. 2006;152(4):785–92.
Saely CH, Koch L, Schmid F, Marte T, Aczel S, Langer P, Hoefle G, Drexel H. Adult Treatment Panel III 2001 but not International Diabetes Federation 2005 criteria of the metabolic syndrome predict clinical cardiovascular events in subjects who underwent coronary angiography. Diabetes Care. 2006;29(4):901–7.
Alberti KG. IDF Epidemiology Task Force Consensus Group. The metabolic syndrome: a new worldwide definition. Lancet. 2005;366:1059–62.
Isomaa BP, Almgren T, Tuomi B, Forsén K, Lahti M, Nissen MR, Taskinen L. Groop Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabetes Care. 2001;24(4):683–9.
Mohammadi M, Vaisi Raiegani AA, Jalali R, Ghobadi A, Salari N. The prevalence of retinopathy among type 2 diabetic patients in Iran: A systematic review and meta-analysis. Rev Endocr Metab Disord. 2019;20(1):79-88.
Fanning E, O’Shea D. Genetics and the metabolic syndrome. Clin Dermatol. 2018;36(1):9–13.
McNeill AM, Rosamond WD, Girman CJ, Golden SH, Schmidt MI, East HE, Ballantyne CM, Heiss G. The metabolic syndrome and 11-year risk of incident cardiovascular disease in the atherosclerosis risk in communities study. Diabetes Care. 2000;28(2):385–90.
He YB, Jiang J, Wang K, Feng Q, Chang L, Fan X,. Hu FB. Prevalence of the metabolic syndrome and its relation to cardiovascular disease in an elderly Chinese population. J Am Coll Cardiol. 2006;47(8):1588–94.
Bonora E, Kiechl S, Willeit J, Oberhollenzer F, Egger G,. Bonadonna RC, Muggeo M. Carotid atherosclerosis and coronary heart disease in the metabolic syndrome: prospective data from the Bruneck study. Diabetes Care. 2003;26(4):1251–7.
Ridker PM, Buring JE, Cook NR, Rifai N. C-reactive protein, the metabolic syndrome, and risk of incident cardiovascular events: an 8-year follow-up of 14 719 initially healthy American women. Circulation. 2003;107(3):391–7.
Resnick HE, Jones K, Ruotolo G, Jain AK, Henderson J, Lu W, Howard BV. Insulin resistance, the metabolic syndrome, and risk of incident cardiovascular disease in nondiabetic American Indians: the Strong Heart Study. Diabetes Care. 2000;26(3):861–7.
Zabetian A, Hadaegh F, Azizi F. Prevalence of metabolic syndrome in Iranian adult population, concordance between the IDF with the ATPIII and the WHO definitions. Diabetes Res Clin Pract. 2007;77(2):251–7.
Rahmanian E, Salari N, Mohammadi M, Jalali R. Evaluation of sexual dysfunction and female sexual dysfunction indicators in women with type 2 diabetes: a systematic review and meta-analysis. Diabetol Metab Syndr. 2019;11:73.
Harandi SA, Sarrafzadegan N, Sadeghi M, Talaei M, Dianatkhah M, Oveisgharan S, Pourmoghaddas A, Salehi A, Sedighifard Z. Do cardiometabolic risk factors relative risks differ for the occurrence of ischemic heart disease and stroke? Res Cardiovasc Med. 2016;5(1):e30619.
Hadaiegh F, Zabetian A, Tohidi M, Azizi F. The Relationship between Metabolic Syndrome and its Components with Coronary Heart Disease in Iranian Men and Women: Tehran Lipid and Glucose Study. Journal of Tehran University of Medical Sciences. 2008;66(8):590–59.
Ansari R, Kahbazi M, Abdar M. Frequency of Metabolic Syndrome Phenotypes in Patients with Hypertension in Isfahan and Markazi Province, Isfahan Healthy Heart Project. Arak University of Medical Sciences Journal. 2005;10(1):1–9.
Shojaei V, Lazari N, Ghalenoi M, Salehabadi S. Relationship between metabolic syndrome in elderly with cardiovascular disease. Iranian Journal of Nursing. 2014;27(92):65–72.
Mohagheghi A, Panahi AR, Hedaiat K, Ghorbani B. Correlation of left main coronary artery stenosis with metabolic syndrome in ischemic heart patients: a two-year study. Journal of Tehran University of Medical Sciences. 2011;69(9):571–5.
Ashari FE, Pirdehghan A, Khoshabi AS, Gharakhani M, Jiryaee N. Prevalence of Metabolic Syndrome in Patients Admitted to the Cardiology Ward of Farshchian Hospital in Hamadan City, Iran. Avicenna J Clin Med. 2018;25(3):177–84.
Anvari MS, Boroumand MA, Pourgholi L, Sheikhfathollahi M, Rouhzendeh M, Rabbani S, Goodarzynejad H. Potential link of microalbuminuria with metabolic syndrome in patients undergoing coronary angiography. Arch Med Res. 2009;40(5):399–405.
Ardeshiri M, Faritus Z, Ojaghi-Haghighi Z, Bakhshandeh H, Kargar F, Aghili R. Impact of metabolic syndrome on mortality and morbidity after coronary artery bypass grafting surgery. Research in cardiovascular medicine. 2014;3(3):e20270.
Dehghani MR, Rezaei Y, Fakour S, Arjmand N. White blood cell count to mean platelet volume ratio is a prognostic factor in patients with non-ST elevation acute coronary syndrome with or without metabolic syndrome. Korean circulation journal. 2016;46(2):229–38.
Ebrahimi M, Kazemi-Bajestani SMR, Ghayour-Mobarhan M, Moohebati M, Paydar R, Azimi-Nezhad M, Esmaily HO, Ferns GA. Metabolic syndrome may not be a good predictor of coronary artery disease in the Iranian population: population-specific definitions are required. The Scientific World Journal. 2009;9:86–96.
Firouzi A, Tohidnia S, Shakerian F, Sanaati H, Hashem A, Vagheei Tabar R. Comparison of prevalence of metabolic syndrome between idiopathic and secondary deep vein thrombosis. Iranian Heart Journal. 2012;13(1):23–8.
Gharipour M, Jazi MH, Nilforoush P, Batvandi A, Mohammadi R, Najafi R. Metabolic syndrome and its association with left ventricular dysfunction in patients with left bundle branch block. Acta Bio Medica Atenei Parmensis. 2015;86(2):157–61.
Hadaegh F, Khalili D, Ghasemi A, Tohidi M, Sheikholeslami F, Azizi F. Triglyceride/HDL-cholesterol ratio is an independent predictor for coronary heart disease in a population of Iranian men. Nutrition Metabolism Cardiovascular Diseases. 2019;19(6):401–8.
Hadaegh F, Zabetian A, Tohidi M, Ghasemi A, Sheikholeslami F, Azizi F. Prevalence of metabolic syndrome by the Adult Treatment Panel III, International Diabetes Federation, and World Health Organization definitions and their association with coronary heart disease in an elderly Iranian population. Annals Academy of Medicine Singapore. 2009;38(2):142–51.
Kelishadi R, Derakhshan R, Sabet B, Sarraf-Zadegan N, Kahbazi M, Sadri G, Tavasoli A, Heidari S, Khosravi A. Amani A.The metabolic syndrome in hypertensive and normotensive subjects: the Isfahan Healthy Heart Programme. Ann Acad Med Singapore. 2005;34(3):243–9.
Lankarani KB, Ghaffarpasand F, Mahmoodi M, Dehghankhalili M, Honarvar B, Lotfi M, Zamiri N, Heydari ST, Fallahzadeh MK. MaharloueiN. Predictors of common carotid artery intima-media thickness and atherosclerosis in a sample of Iranian general population. Shiraz E-Medical Journal. 2015;16(5):421–32.
Montazerifar F, Bolouri A, Mozaffar MM, Karajibani M. The prevalence of metabolic syndrome in coronary artery disease patients. Cardiology research. 2016;7(6):202–11.
Sadeghian S, Darvish S, Salimi S, Esfehani FA, Fallah N, Mahmoodian M, Salarifar M, Karimi A. Metabolic syndrome: stronger association with coronary artery disease in young men in comparison with higher prevalence in young women. Coron Artery Dis. 2007;18(3):163–8.
Zabetian A, Hadaegh F, Azizi F. Relationship between metabolic syndrome and its components with coronary heart disease in Iranian men and women. Exp Clin Endocrinol Diabetes. 2008;116(09):525–31.
Kazemi T, Sharifzadeh G, Zarban A, Fesharakinia A. Comparison of components of metabolic syndrome in premature myocardial infarction in an Iranian population: a case-control study. International journal of preventive medicine. 2013;4(1):110–21.
Saadatian V, Ghareh S, Shakeri M, Emadzadeh M, Taraz Jamshidi S, Emadzadeh A. The frequency of metabolic syndrome among female patients admitted in psychiatry ward. Med J Mashhad Univ Med Sci. 2011;54(4):230–7.
Rashidi H, Fardad F, Ghaderian B, Shahbazian HB, Latifi M, Karandish M, et al. Prevalence of metabolic syndrome and its predicting factors in type 2 diabetic patients in Ahvaz. Jundishapur Sci Med J. 2012;11(1):163–75.
Aguilar M, Bhuket T, Torres S, Liu B, Wong RJ. Prevalence of the metabolic syndrome in the United States, 2003–2012. Jama. 2015;313(19):1973–4.
Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults: findings from the third National Health and Nutrition Examination Survey. Jama. 2002;287(3):356–9.
Cankurtaran M, Halil M, Yavuz BB, Dagli N, Oyan B, Ariogul S. Prevalence and correlates of metabolic syndrome (MS) in older adults. Arch Gerontol Geriatr. 2006;42(1):35–45.
Scuteri A, Najjar SS, Morrell CH, Lakatta EG. The metabolic syndrome in older individuals: prevalence and prediction of cardiovascular events: the Cardiovascular Health Study. Diabetes Care. 2005;28(4):882–7.
He Y, Jiang B, Wang J, Feng K, Chang Q, Fan L, Li X,. Hu FB. Prevalence of the metabolic syndrome and its relation to cardiovascular disease in an elderly Chinese population. J Am Coll Cardiol. 2006;47(8):1588–94.
Sattar N, Gaw A, Scherbakova O, et al. Metabolic syndrome with and without Creactive protein as a predictor of coronary heart disease and diabetes in the West of Scotland Coronary Prevention Study. Circulation. 2003;108:414–9.
Lakka HM, Laaksonen DE, Lakka TA, Niskanen LK, Kumpusalo E, Tuomilehto J, Salonen JT. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. Jama. 2002;288(21):2709–16.
McNeill AM, Katz R, Girman CJ, Rosamond WD, Wagenknecht LE, Barzilay JI, Tracy RP, Savage PJ, Jackson SA. Metabolic syndrome and cardiovascular disease in older people: the cardiovascular health study. J Am Geriatr Soc. 2006;54(9):1317–24.
Festa A, D’Agostino R Jr, Howard G, Mykkanen L, Tracy RP, Haffner SM. Chronic subclinical inflammation as part of the insulin resistance syndrome: the Insulin Resistance Atherosclerosis Study (IRAS). Circulation. 2000;102(1):42–7.
Grundy SM, Brewer HB Jr, Cleeman JI, Smith SC, Lenfant C. Definition of metabolic syndrome: report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation. 2004;109(3):433–8.
Alexander CM. Third National Health and Nutrition Examination Survey (NHANES III); National Cholesterol Education Program (NCEP). NCEP-defined metabolic syndrome, diabetes, and prevalence of coronary heart disease among NHANES III participants age 50 years and older. Diabetes. 2003;52:1210–4.
Ford ES. Risks for all-cause mortality, cardiovascular disease, and diabetes associated with the metabolic syndrome: a summary of the evidence. Diabetes care. 2005;28(7):1769–78.
Hadaegh F, Zabetian A, Harati H, Azizi F. The prospective association of general and central obesity variables with incident type 2 diabetes in adults, Tehran lipid and glucose study. Diabetes Res Clin Pract. 2007;76(3):449–54.
Azizi F, Azadbakht L, Mirmiran P. Trends in overweight, obesity and central fat accumulation among Tehranian adults between 1998–1999 and 2001–2002: Tehran lipid and glucose study. Annals of nutrition metabolism. 2005;49(1):3–8.
Azadbakht L, Mirmiran P, Shiva N, Azizi F. General obesity and central adiposity in a representative sample of Tehranian adults: prevalence and determinants. International journal for vitamin nutrition research. 2005;75(4):297–304.
Rashidi A, Mohammadpour-Ahranjani B, Vafa MR, Karandish M. Prevalence of obesity in Iran. Obes Rev. 2005;6:191–2.
Acknowledgements
The authors thank the By Student Research Committee of Kermanshah University of Medical Sciences, Iran.
Funding
By Student Research Committee of Kermanshah University of Medical Sciences, Deputy for Research and Technology, Kermanshah University of Medical Sciences (IR) (30090000). The deputy of research and technology –Kermanshah University of Medical Sciences had no role in the design of the study and collection, analysis, and interpretation of data and in writing of the manuscript.
Author information
Authors and Affiliations
Contributions
KD and NR contributed to the design, MM and RJ statistical analysis, participated in most of the study steps. AD and AVR and AA and NS prepared the manuscript. MK and PKJ assisted in designing the study, and helped in the, interpretation of the study. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not declared.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Salari, N., Doulatyari, P.K., Daneshkhah, A. et al. The prevalence of metabolic syndrome in cardiovascular patients in Iran: a systematic review and meta-analysis. Diabetol Metab Syndr 12, 96 (2020). https://doi.org/10.1186/s13098-020-00605-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13098-020-00605-4