
Abstract
Background
Optimising hearing and vision function may be important in improving a range of outcomes for people living with dementia (PwD) and their companions. The SENSE-Cog cross-national randomised controlled trial (RCT) is evaluating the effectiveness of a sensory intervention (SI) to improve quality of life for PwD with concurrent hearing and/or vision impairment, in five European countries. To ascertain how or why the intervention will, or will not, achieve its outcomes, we have designed a process evaluation to explore potential discrepancies between expected and observed outcomes. This will also help us to understand how context may influence the outcomes. Here we describe the protocol for this process evaluation, which is embedded within the RCT.
Methods/design
We will use a mixed methods approach with a theoretical framework derived from the UK Medical Research Council’s’ guidance on process evaluations. It will include the following: (1) evaluating how key aspects of the intervention will be delivered, which will be important to scale the intervention in real world populations; (2) characterising the contextual issues, which may shape the delivery and the impact of the intervention in different countries; and (3) investigating possible causal mechanisms through analyses of potential moderators and mediators. To avoid bias, we will analyse the process data before the analysis of the main effectiveness outcomes.
Discussion
This evaluation will provide insight into how the complex SENSE-Cog SI will be tailored, enacted and received across the different European contexts, all of which have unique health and social care economies. The findings will provide insight into the causal mechanisms effecting change, and will determine whether we should implement the intervention, if effective, on a wider scale for PwD and concurrent sensory impairment.
Trial registration
ISRCTN, ISRCTN17056211. Registered on 19 February 2018.
Similar content being viewed by others


Background
There is growing evidence that people with dementia (PwD) with ageing-related hearing and vision impairment experience worse outcomes compared to PwD with optimal sensory function. These outcomes include increased disorientation, difficulties self-locating using visual or auditory cues, higher levels of distress leading to agitation and aggression and increased prevalence of hallucinations, delusions and depression [1,2,3]. Sensory impairment itself can worsen cognitive decline, as well as exacerbate the social isolation that is often associated with dementia [4]. Individuals may withdraw from social activities and hobbies and become marginalised [5,6,7,8]. Furthermore, burnout and physical exhaustion in care partners can be amplified by communication barriers [3] and greater dependency of the PwD. Thus, we designed the SENSE-Cog randomised controlled trial (RCT) to answer the research question, ‘Can a home-based, tailored ‘sensory intervention’ (SI) improve quality of life in PwD with comorbid hearing and/or visual impairment?’
The multi-component SI that the SENSE-Cog trial will evaluate comprises assessment, treatment and support of hearing and vision impairment in PwD. We developed the SI iteratively over 24 months. This involved: (1) a scoping review of the literature [9]; (2) an in-depth qualitative exploration of the support care needs of PwD with sensory impairment in three European countries [10]; (3) an international survey (n = 653); and (4) an interdisciplinary Expert Reference Group (n = 17) [11, 12]. The findings were synthesized into a draft SI that was then field tested in the UK, France and Cyprus [13,14,15], prior to development of the protocol for the full multi-site RCT [16], the SENSE-Cog trial.
The SENSE-Cog trial is a 36-week parallel-group, observer-blind, multicentre, superiority RCT comparing the individualised SI to usual care in PwD with hearing and/or visual impairment and their companion (the participant ‘dyad’). Briefly, it involves 354 randomized dyads (1:1; 177 per arm) in five European sites: Athens (Greece), Dublin (Ireland), Manchester (UK), Nice (France), and Nicosia (Cyprus). The primary outcome of the trial is quality of life in the PwD, measured at 36 weeks post-baseline using the DEMQOL [17]. The DEMQOL is a 29-item, interviewer-administered, self-report questionnaire with good psychometric properties in persons with mild to moderate dementia. Secondary outcomes include neuropsychiatric symptoms, measures of mental wellbeing, sensory and cognitive functional ability, relationships and health resource utilisation. Companion outcomes and health economic measures are also being assessed. Here we describe the protocol for a process evaluation of the RCT as per the UK Medical Research Council (MRC) recommendations [18].
‘Complex interventions’, such as the SENSE-Cog SI, are defined as those comprising multiple components interacting to produce change [18, 19]. The range of outcomes, and the degree of tailoring or flexibility required for each individual participant, is significant, thus adding to the complexity [12]. While RCTs are the soundest means of inferring causality of an intervention, they cannot ascertain how or why an intervention may or may not achieve the outcomes [20]. Thus, we have embedded a detailed process evaluation within the RCT to clarify this [18]. This evaluation, together with the outcomes of the RCT, will enable policy makers, funders and practitioners to determine whether the intervention is effective or not, and whether it should be implemented on a wider scale. This is particularly relevant for the cross-national SENSE-Cog trial, which is taking place in five European contexts. It will fill a significant evidence gap in the management of hearing and vision impairment in PwD.
The specific aims of this process evaluation are to: (1) explore the delivery, or the process through which the SI will be offered, including barriers and facilitators; (2) evaluate contextual issues and clarify factors that may affect the SI delivery, mechanisms and outcomes [21]; and (3) investigate possible causal mechanisms, using analyses of potential moderators and mediators.
Methods/design
The protocol for our process evaluation follows a systematic approach for the design and conduct of the evaluation [18].
Planning the process evaluation
Working with intervention developers and implementers
A process evaluation requires a degree of independence to appraise the intervention team’s delivery of the trial [18]. Thus, we delegated oversight of the evaluation to an expert not involved in the day-to-day conduct of the RCT but on the wider SENSE-Cog team (CA). Regular process evaluation reports will be made at Trial Steering Committee meetings [16] and specific meetings with the study chief investigator (IL), the methodologist (EF) and the process lead (CA).
Overlap of the process and outcomes and cost-effectiveness evaluations
Due to the complexity of the study, we have embedded the process evaluation within the daily conduct of the outcomes and cost-effectiveness evaluations. Thus, data for all three purposes are being collected concurrently, and some measures may be used for both process and outcome evaluations. During team training, we emphasized the multi-purposing of data and the need to maintain ‘researcher equipoise’.
Description of the intervention
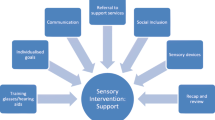
We have previously detailed the SI components and implementation [12]. In summary, the SI, which is delivered as a ten-session programme by a trained ‘sensory support therapist’ (SST) and audiologists/optometrists, is outlined in Fig. 1. It involves several components, notably: (1) identifying and correcting any vision or hearing impairment; (2) supporting adherence to the hearing and/or vision devices, through advice and training in correct use and care; (3) enhancing communication between the PwD and their companion; (4) demonstrating environmental aids and sensory devices; and (5) accessing relevant support services and social networks. The non-intervention group receives ‘care as usual’ (CAU) access to the services and interventions normally available to PwD and their companions in their respective countries and sites.

How the elements of the ‘COM-B Behaviour Change’ model and components of the sensory intervention link together. BADLs Bristol Activities of Daily Living Scale [22], Bangor The Bangor Goal-Setting interview [23], DEMQoL Dementia Quality of Life [24], FCS Family Caregiving Role Scale [25], HADS Hospital Anxiety and Depression Scale [26], HASK Hearing Aid Skills and Knowledge test [27], HHIE-25 Hearing Handicap Inventory for the Elderly [28], GHQ-12 General Health Questionnaire [29], MoCA Montreal Cognitive Assessment [30], NPI-12 Neuropsychiatric Inventory [31], RSS Relationship Satisfaction Scale [32], SF-12 Short Form Health Survey [33], VA LV-VFQ-20 Veterans Affairs Low vision Visual Functioning Questionnaire [34]
Causal assumptions about how change will be produced
To understand fully the impact of the intervention on the outcomes, and to generalise the findings in the pan-European context of SENSE-Cog, an exploration of causal mechanisms and unanticipated pathways is needed [19]. We will do this by extracting pre-specified mediating variables and qualitative data (from a sub-sample of 30 participant dyads) and evaluating adverse events and unexpected consequences of the intervention. We will also undertake semi-structured interviews with the SSTs at each of the five study sites.
The principal aim of the intervention is to improve quality of life and functional ability by improving sensory function through devices and behavioural change. Dementia-related quality of life comprises the domains of daily activities (activities of daily living and self-care), physical health and wellbeing, cognitive functioning and social relationships [35]. To influence these domains, we have adopted the COM-B component of the Behaviour Change Wheel [36] as our framework for how the intervention might work. According to this model, behavioural change (‘B’) results from: capability (‘C’), the individual’s psychological and physical capacity to engage in the activity concerned; opportunity (‘O’), the external factors that support behavioural change; and motivation (‘M’), the conscious and sub-conscious processes that direct decision making [36]. In Table 1 and Fig. 1, using a logic model, we outline how each COM-B element aligns with specific components of the SI, and how these might hypothetically lead to improvements in quality of life, our primary outcome.
Briefly, for capability, the sensory aids (i.e. hearing aids, glasses and sensory environment modification in the home) and SST adherence support will improve hearing and vision (physical capability), which will enhance sensory-cognitive function and overall functional ability and reduce neuropsychiatric symptoms [37,38,39,40,41]. The SST will train communication skills and improve knowledge of dementia and sensory impairment (psychological capability). This will increase opportunity by decreasing dependency on companions, enhancing social interactions and reducing loneliness. Adherence support for PwD with sensory devices will enhance hearing [42], vision [43] or both [15]. Furthermore, social opportunities will be enhanced through signposting outside the home, thus addressing social isolation, improving social relationships and providing respite for companions. Regarding motivation, higher sensory-cognitive function and improved neuropsychiatric symptoms will improve self-efficacy, self-esteem and mental wellbeing [44, 45]. However, motivation may be reduced in dementia, particularly if apathy is present. Thus, the SI will address this through goal setting. We will measure apathy to take account of motivation as a potential moderator, or even mediator, of the intervention’s impact. Greater independence and communication ability in the PwD will reduce companions’ burden and stress, which will also impact positively the overall wellbeing. Attitudes and knowledge training will support change maintenance and relationship quality [46].
Identification of key uncertainties and developing a framework for the process evaluation
In Table 2, we identified key uncertainties to address for each SI. We will use a mixed method approach to capture the data for the evaluation. This will involve a variety of instruments, as outlined in Table 3.
Exploration of delivery
To ascertain whether the SI is delivered (i.e. ‘how’) and enacted (i.e. ‘what’) as intended [18], we will examine the fidelity and dose (i.e. duration, number and frequency of SI visits) of the delivered intervention. Due to potential burden on participants, we have chosen not to include an external evaluation of fidelity (i.e. independent observer during sessions). Instead, we will rely on the proxy measure of ‘fidelity’ as determined by thoroughness of SST training and supervision, use of therapist manual and SST logbook recordings of sessions. We will document the nature of the support offered by the intervention, including the type of corrective devices, the environmental changes to support sensory function, the number and types of referral or signposts to extra-trial services. These data will be captured through participant diaries (the PwD and their companion) and the SST logbook.
Specifically, the PwD diaries will contain Likert style ratings [50] of acceptability and tolerability of SI visits, including measures of helpfulness, effort, fatigue, understanding and motivation; and how acceptable the corrective sensory devices are. The companions´ diaries will capture data relating to how the PwD engages with the visit, how the PwD is adapting to their sensory aids, and how confident the companion feels in supporting the PwD in using the aids. The SST logbooks will contain details of each visit, the components of the SI delivered, participant response to the intervention and skill in managing their aids. Additionally, the SST logbooks will detail how the SI is specifically tailored to the dyad.
We will assess reach through the representativeness of the sites, the recruitment process (refusal rate, attrition rate) and the representativeness of the study population according to the target population [51].
Evaluation of contextual issues
The SENSE-Cog RCT will take place in several different countries and involve three languages (English, French and Greek). Thus, contextual issues, which are external to the intervention itself, need to be carefully considered. These include differences in language, culture, access to services and the health and social care economy. Context may influence the SST’s ability to foster change in the participant dyad’s circumstances. For example, for social isolation, the SST may recommend attendance at a local lunch club; however, if transportation is not suitable for individuals with sensory and cognitive impairment, the opportunity to take up the offer will be hampered. Likewise, communication training with companions may be differently received in diverse cultural and linguistic contexts. Thus, the same intervention may have divergent outcomes according to the setting in which it is delivered [18]. The dyadic relationship (between the PwD and their companion) should also be considered because the level of support and quality of relationship may vary among dyads. To capture contextual data, we will collect information from the demographic and outcome measures, the participant dyad diaries, the SST logbook and in-depth qualitative interviews of a sub-sample of participant dyads (n = 30 dyads across the sites), as detailed in the SENSE-Cog trial protocol [16].
Sampling and timing of data collection
We will collect characteristics of each participant dyad, including gender, age and support structure at the screening visit, and at baseline, week 18 and week 36 (Tables 3 and 4). Following each SI visit (for the active arm), participant diaries and SST logbooks will be completed. The sub-sample qualitative interviews will take place within 2 weeks following the SI (details described in [16]). Training logs for the SSTs were collected prior to study start. SST supervision logs and fidelity checks of the SST logbooks are being collected throughout the trial. SST interviews will be held within 2 weeks after the last intervention visit of the last randomised dyad in each site. Briefly, these interviews will explore the experience of having received the intervention, from the perspective of each member of the dyad. The sample size for this sub-sample was selected to achieve theoretical and data saturation. The interviews from all sites will be analysed by using conventional qualitative content analysis [52] and a grounded theory approach [53].
Analysis
To avoid biased interpretation, as recommended by the MRC’s guidance, we will analyse and explore process data arising from the qualitative interviews and contextual factors before the unblinded trial outcomes are known [18]. We will use the process data to generate specific hypotheses (pre-trial explanation before trial outcomes are revealed) regarding factors that moderate and/or mediate the effect of the SI on outcomes, notably quality of life. This will minimise the risk of ‘fishing’ for relationships and falsely significant findings due to multiple testing.
Moderator analyses will be undertaken, with appropriate caution, to investigate any influence of the baseline characteristics of the dyads (e.g. age, gender, type of sensory impairment, level of cognitive impairment, type of companion) and country/site effect on the strength and/or direction of the relationship between the SI and the outcomes. We will undertake mediation analyses to assess the degree to which the impact of the SI on the stated outcomes is a direct effect, or is indirect via the hypothesised mediating factors which will be modelled as latent variables in a structural equation modelling framework.
We will conduct the moderator/mediator analysis only after the final RCT analysis has been completed and the dataset has been un-blinded. We will do this regardless of whether the SI has a significant direct impact on the primary outcome.
We will apply a regression framework, using newer methods and statistical models [54, 55] that improve on traditional approaches (e.g. [56]). These models can become complex, particularly when controlling for multiple covariates. Thus, depending upon the number and complexity of the hypotheses to be tested, we will assess whether it will be better to analyse each factor separately, or to combine sets of moderators and/or mediators into a ‘conditional process analysis’ [54]. We will conduct separate analyses for those variables available in both trial arms, and those available in the intervention group only (e.g. related to the SI). The latter analyses will help to identify process measures that are part of the SI and may moderate its efficacy (for e.g., number of SST visits, SST experience and fidelity), using appropriate techniques [57].
Discussion
The process evaluation of the SENSE-Cog RCT will appraise several important aspects of the delivery of the intervention, the context of delivery and the hypothesised causative mechanisms. These issues are key to interpreting the effectiveness outcomes of the trial and, if outcomes are positive, to assist in understanding implications for scale-up in clinical settings. The SI will have multiple interacting components: assessing and correcting hearing and vision impairment (hearing aids and/or glasses lenses), training in the use of the devices, enhancing communication within the dyad, optimising the home sensory environment and supporting engagement in health and wellbeing opportunities in the community, including social integration and external support services.
A key challenge in delivering the SENSE-Cog SI is to maintain standardisation and rigour when implementing such a complex intervention across five different European sites. The SENSE-Cog SI is ambitious in its vision in addressing three co-morbidities simultaneously—cognitive impairment, hearing loss and vision loss—and to assess the impact of a psychosocial intervention on managing these impairments. We will aim to capture the cultural, social and economic nuances of the respective European study sites whilst deriving results that can be applied in a pan-European context. To ensure that we capture the cultural differences from the qualitative interviews, we will keep translation to a minimum, as recommended by Haak et al. [58].
The theoretical model with causal relationships will be informed by the mediation analyses. The elicited data will also enable us to ‘test’ the theoretical model of the COM-B by addressing the key uncertainties listed in Table 1. This will be the first opportunity to evaluate empirically the COM-B model in a RCT setting, as demonstrated in Fig. 1.
Strengths and limitations of the study
A strength of our study protocol includes the use of a mixed method approach, including both qualitative and quantitative measures, to carefully explore the ‘how and why’ of the intervention. Another strength of our approach includes the sound theoretical framework on which the intervention was developed, and the iterative manner in which it was modified and field-tested [12, 15] before arriving at the final version of the intervention, ready for full scale effectiveness testing. A limitation (although also a potential strength) is the significant degree of variability in the study sites due to the different EU contexts in which the programme takes place, as well as the variability of the intervention offered to each participant dyad, resulting from the tailored approach.
Reporting and dissemination
We will report the results of the process evaluation described here using a combination of reporting guidance, including CONSORT [59] and COREQ (for the qualitative outcomes) [60] as well as statistical methods for mediators and moderators [61]. We will submit the findings to an open-access journal, as per the requirements of the funder. As recommended by others [51], we have described our protocol in advance to foster transparency in reporting and to help the development and evaluation of complex psychosocial interventions for PwD, an emerging area of health services research. Finally, we will link our outputs related to the SENSE-Cog trial through the SENSE-Cog programme website (www.sense-cog.eu).
Ethics approval and consent to participate
In Manchester, the study received final approval (version 3.0) by the NW Haydock ethics committee on 22 January 2018 and obtained sponsor approval on 8 March 2019. In Nicosia, the study received favourable opinion on 27 September 2016 from the Cyprus National Bioethics Committee. In Athens, the Local Ethics Committee of Health Sciences and Scientific Committee of the Eginition Hospital of the National and Kapodistrian University of Athens ethics committee granted a favourable opinion on 24 January 2018. In Dublin, the Saint James Hospital/AMNCH Research Ethics Committee gave approval on the 25 October 2018. In Nice, the “Comité de Protection des personnes Sud Est I” gave a favourable opinion on 12 July 2018. Written consent is collected from the participants eligible for the study, using procedures in accordance with the national guidance regarding informed consent and clinical research (for individuals with or without capacity to consent) in each of the participating countries (detailed in Regan et al. [16]). All researchers have been fully trained in Good Clinical Practice (GCP) and mental capacity assessment skills and follow national guidance in their respective countries, such as the Mental Capacity Act (2005) in the UK. If a person lacks capacity, a nominated consultee will be asked to deem whether it is in the PwD’s best interests to participate.
Trial status
This process evaluation is based on the SENSE-Cog RCT protocol version 4.0 of 16 November 2018. The overall SENSE-Cog research programme started in January 2016 and the SENSE-Cog RCT (Work Package 3.2) started recruitment in summer 2018. Recruitment is expected to end in December 2020. The first qualitative interviews with participants took place in November 2018. The process evaluation will start in following the last W36 assessment of the first randomized participant dyad.
Availability of data and materials
Data generated or analysed during this study will be included in the article reporting the results that will be shared through scientific articles and international conferences.
Abbreviations
- AE:
-
Adverse events
- COM-B:
-
Capability, opportunity, motivation-behavioural change wheel
- MRC:
-
Medical research council
- PwD:
-
People with dementia
- RCT:
-
Randomized controlled trial
- SI:
-
Sensory intervention
- SST:
-
Sensory support therapist
References
Fortunato S, Forli F, Guglielmi V, De Corso E, Paludetti G, Berrettini S, et al. A review of new insights on the association between hearing loss and cognitive decline in ageing. Acta Otorhinolaryngo. 2016;36(3):155–66.
Rutherford BR, Brewster K, Golub JS, Kim AH, Roose SP. Sensation and psychiatry: Linking age-related hearing loss to late-life depression and cognitive decline. Am J Psychiatry. 2018;175(3):215–24.
Lawrence V, Murray J, Banerjee S, Ffytche D. The experiences and needs of people with dementia and serious visual impairment: a qualitative study. London: Thomas Pocklington Trust; 2008.
Maharani A, Pendleton N, Leroi I. Hearing impairment, loneliness, social isolation, and cognitive function: Longitudinal analysis using English Longitudinal Study on Ageing. Am J Geriat Psychiat. 2019;27(12):1348–56.
McKeefry D, Bartlett R. Improving vision and eye health care to people with dementia. London: Thomas Pocklington Trust; 2010.
Elliott AF, McGwin G, Owsley C. Health-related quality of life and visual and cognitive impairment among nursing-home residents. Brit J Ophthalmol. 2009;93(2):240–3.
Lupsakko T, Mantyjarvi M, Kautiainen H, Sulkava R. Combined hearing and visual impairment and depression in a population aged 75 years and older. Int J Geriatr Psych. 2002;17(9):808–13.
McDonnall MC. The effects of developing a dual sensory loss on depression in older adults: a longitudinal study. J Aging Health. 2009;21(8):1179–99.
Dawes P, Wolski L, Himmelsbach I, Regan J, Leroi I. Interventions for hearing and vision impairment to improve outcomes for people with dementia: a scoping review. Int Psychogeriatr. 2019;31(2):203–21.
Leroi I, Wolski L, Charalambous AP, Constantinidou F, David R, Dawes P, Hann M, Himmelsbach I, Miah J, Payne M, Simkin Z, Thodi C, Yeung W, Yohannes AM. Support care needs of people with dementia and hearing and vision impairment: A European perspective. In: ACRM 96th Annual Conference, Progress in Rehabilitation Research. Chicago: American Congress of Rehabilitation Medicine; 2019.
Leroi I, Himmelsbach I, Wolski L, Littlejohn J, Jury F, Parker A, et al. Assessing and managing concurrent hearing, vision and cognitive impairments in older people: an international perspective from healthcare professionals. Age Ageing. 2019;48(4):580–7.
Leroi I, Pye A, Armitage CJ, Charalambous AP, Constantinidou F, Helmer C, et al. Research protocol for a complex intervention to support hearing and vision function to improve the lives of people with dementia. Pilot Feasibility Stud. 2017;3:38.
Regan J, Dawes P, Pye A, Armitage CJ, Hann M, Himmelsbach I, et al. Improving hearing and vision in dementia: protocol for a field trial of a new intervention. BMJ Open. 2017;7(11):1–12.
Hooper E, Simkin Z, Abrams H, Camacho E, Charalambous AP, Collin F, et al. Feasibility of an intervention to support hearing and vision in dementia: The SENSE-Cog field trial. J Am Geriatr Soc. 2019;67(7):1472–7.
Leroi I, Simkin Z, Hooper E, Wolski L, Abrams H, Armitage CJ, et al. Impact of an intervention to support hearing and vision in dementia: The SENSE-Cog field trial. Int J Geriatr Psych. 2019:1–10.
Regan J, Frison E, Collin F, Dawes P, Hann M, Himmelsbach I, et al. Individualised sensory intervention to improve quality of life in people with dementia and their companions (SENSE-Cog trial): study protocol for a randomised controlled trial. Trials. 2019;20:1–15.
Smith SC, Lamping DL, Banerjee S, Harwood R, Foley B, Smith P, et al. Measurement of health-related quality of life for people with dementia: development of a new instrument (DEMQOL) and an evaluation of current methodology. Health Technol Assess. 2005;9(10):1–93 iii-iv.
Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ. 2015;350:1–7.
Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. 2008;337(7676):1–6.
Barratt H, Campbell M, Moore L, Zwarenstein M, Bower P. Randomised controlled trials of complex interventions and large-scale transformation of service. In: Raine R, Fitzpatrick R, Barratt H, Bevan G, Black N, Boaden R, et al., editors. Health Services and Delivery Research; 2016. p. 19–31.
Howarth E, Devers K, Moore G, O'Cathain A, Dixon-Woods M. Contextual issue and qualitative research. In: Raine R, Fitzpatrick R, Barratt H, Bevan G, Black N, Boaden R, et al., editors. Health Services and Delivery Research; 2016. p. 205–120.
Bucks RS, Ashworth DL, Wilcock GK, Siegfried K. Assessment of activities of daily living in dementia: Development of the Bristol activities of daily living scale. Age Ageing. 1996;25(2):113–20.
Clare L, Hindle JV, Jones IR, Thom JM, Nelis SM, Hounsome B, et al. The AgeWell study of behavior change to promote health and wellbeing in later life: study protocol for a randomized controlled trial. Trials. 2012;13:1–9.
Smith SC, Lamping DL, Banerjee S, Harwood RH, Foley B, Smith P, Cook JC, Murray J, Prince M, Levin E, Mann A, Knapp M. Development of a new measure of health-related quality of life for people with dementia: DEMQOL. Psychol Med. 2006;37:737-46.
Schofield HL, Murphy B, Herrman HE, Bloch S, Singh B. Family caregiving: Measurement of emotional well-being and Various aspects of the caregiving role. Psychol Med. 1997;27(3):647–57.
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiat Scand. 1983;67(6):361–70.
Saunders GH, Morse-Fortier C, McDermott DJ, Vachhani JJ, Grush LD, Griest S, et al. Description, normative data, and utility of the hearing aid skills and knowledge test. J Am Acad Audiol. 2018;29(3):233–42.
Newman CW, Weinstein BE. Judgements of perceived hearing handicap by hearing-impaired elderly men and their spouses. J Acad Rehabilitative Audiol. 1986;19:109–15.
Goldberg DP, Blackwell B. Psychiatric illness in general practice - a detailed study using a new method of case identification. BMJ. 1970;2(5707):439.
Nasreddine ZS, Phillips NA, Bedirian V, Charbonneau S, Whitehead V, Collin I, et al. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–9.
Cummings JL. The Neuropsychiatric Inventory: assessing psychopathology in dementia patients. Neurology. 1997;48(5 Suppl 6):S10–6.
Burns D. Relationship Satisfaction Scale 1983. Ten days to self-esteem. New York: Harper Collins; 1993.
Brazier JE, Roberts J. The estimation of a preference-based measure of health from the SF-12. Med Care. 2004;42(9):851–9.
Stelmack JA, Massof RW. Using the VA LV VFQ-48 and LV VFQ-20 in low vision rehabilitation. Optom Vis Sci. 2007;84(8):705–9.
Mulhern B, Rowen D, Brazier J, Smith S, Romeo R, Tait R, et al. Development of DEMQOL-U and DEMQOL-PROXY-U: generation of preference-based indices from DEMQOL and DEMQOL-PROXY for use in economic evaluation. Health Technol Asses. 2013;17(5):1–160.
Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42.
Wong LLN, Yu JKY, Chan SS, Tong MCF. Screening of cognitive function and hearing impairment in older adults: A preliminary study. Biomed Res Int. 2014;2014:1-7.
Maharani A, Dawes P, Nazroo J, Tampubolon G, Pendleton N, Grp S-CW. Cataract surgery and age-related cognitive decline: A 13-year follow-up of the English Longitudinal Study of Ageing. Plos One. 2018;13(11):e0204833.
Ghiringhelli R, Iorio MCM. Hearing aids and recovery times: a study according to cognitive status. Braz J Otorhinolar. 2013;79(2):177–84.
Martini A, Castiglione A, Bovo R, Vallesi A, Gabelli C. Aging, cognitive load, dementia and hearing loss. Audiol Neurootol. 2014;19(Suppl 1):2–5.
Dawes P, Emsley R, Cruickshanks KJ, Moore DR, Fortnum H, Edmondson-Jones M, et al. Hearing loss and cognition: the role of hearing AIDS, social isolation and depression. PLoS One. 2015;10(3):e0119616.
Nieman CL, Marrone N, Mamo SK, Betz J, Choi JS, Contrera KJ, et al. The Baltimore HEARS Pilot Study: An affordable, accessible, Community-Delivered Hearing Care Intervention. Gerontologist. 2017;57(6):1173–86.
Acton JH, Molik B, Court H, Margrain TH. Effect of a home visit-based low vision rehabilitation intervention on visual function outcomes: An exploratory randomized controlled trial. Invest Ophth Vis Sci. 2016;57(15):6662–7.
Kreeger JL, Raulin ML, Grace J, Priest BL. Effect of hearing enhancement on mental status ratings in geriatric psychiatric-patients. Am J Psychiat. 1995;152(4):629–31.
Rogers MA, Langa KM. Untreated poor vision: a contributing factor to late-life dementia. Am J Epidemiol. 2010;171(6):728–35.
Ogden J, Hills L. Understanding sustained behavior change: the role of life crises and the process of reinvention. Health (London). 2008;12(4):419–37.
EuroQol G. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199–208.
Wimo A, Jonsson L, Zbrozek A. The resource utilization in dementia (RUD) instrument is valid for assessing informal care time in community-living patients with dementia. J Nutr Health Aging. 2010;14(8):685–90.
Gatehouse S. Glasgow Hearing Aid Benefit Profile : Derivation and Validation of a Client-centered Outcome Measure for Hearing Aid Services. J Am Acad Audiol. 1999;10:80–103.
Likert R. A technique for the measurement of attitudes. Arch Psychol. 1932;22(140):5–55.
Liu H, Lindley R, Alim M, Felix C, Gandhi DB, Verma SJ, et al. Protocol for process evaluation of a randomised controlled trial of family-led rehabilitation post stroke (ATTEND) in India. BMJ Open. 2016;6(9):e012027.
Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–88.
Charmaz K. In: Silverman D, editor. Constructing grounded theory: A practical guide through qualitative analysis. London: SAGE Publications Ltd; 2006.
Hayes AF, Rockwood NJ. Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behav Res Ther. 2017;98:39–57.
Fairchild AJ, MacKinnon DP. A general model for testing mediation and moderation effects. Prev Sci. 2009;10(2):87–99.
Baron RM, Kenny DA. The moderator mediator variable distinction in social psychological-research - conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–82.
Dunn G, Emsley R, Liu H, Landau S, Green J, White I, et al. Evaluation and validation of social and psychological markers in randomised trials of complex interventions in mental health: a methodological research programme. Health Technol Assess. 2015;19(93):1–115 v-vi.
Haak M, Himmelsbach I, Granbom M, Lofqvist C. Cross-national and multi-language qualitative research: challenges and recommendations. Brit J Occup Ther. 2013;76(7):333–6.
Moher D, Hopewell S, Schulz KF, Montori V, Gotzsche PC, Devereaux PJ, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. Int J Surg. 2012;10(1):28–55.
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–57.
Lang TA, Secic M. How to report statistics in medicine: Annotated guidelines for authors, editors, and reviewers. 2nd ed. Philadelphia: American College of Physicians; 2006.
Acknowledgements
The authors would like to acknowledge and thank the SENSE-Cog Research User Group, which consists of stakeholders with dementia and sensory impairment and their companions and is coordinated by Jahanara Miah. Their input into all stages of development of the intervention, the protocol and the study materials has been invaluable. Lynne McCrae, the University of Manchester’s Research Practice Governance Coordinator, was very helpful in providing feedback on the protocol. We also acknowledge and thank Francine Jury and Jemma Regan for support in coordination.
SENSE-Cog WP3.2: Harvey Abrams, Nathalie Chaghil-Boissière, Anna Pavlina Charalambous, Fidéline Colllin, Fofi Constantinidou, Lisa Crosby, Piers Dawes, Eric Frison, Camille Gilbert, Mark Hann, Emma Hooper, Ines Himmelsbach, Evangelia Kontogianni, Brian Lawlor, Iracema Leroi, Sarah Marie, Susana Montecelo, Antonios Politis, Otilia Postea, David Reeves, David Renaud, Zoe Simkin, Monique Termote, Chryssoula Thodi, Lucas Wolski.
7Starkey Hearing Technologies
8Bordeaux Population health Research Centre
9European University of Cyprus
10The University of Manchester, Manchester Centre for Health Psychology,
11Centre Hospitalier Universitaire de Bordeaux
12Université de Bordeaux
13National and Kapodistrian University of Athens
14St James’ Hospital, Dublin
15Essilor International
16ARTTIC Consultancy and Management
17The University of Manchester, Division of Population Health, Health Services Research & Primary Care
18French Institute of Health and Medical Research
Funding
The SENSE-Cog project has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement 668648. This process evaluation protocol comprises part of the work undertaken in Work Package 3 of the overall SENSE-Cog programme. The design of the study and collection, analysis and interpretation of data and in writing the manuscript were all undertaken independently of the funding body. The funding body had no influence on any aspect of the study.
Author information
Authors and Affiliations
Consortia
Contributions
IL, EF, FC, MH, DR, EH and ZS and LW were responsible for the overall development of an ethically sound protocol. IL, EF, MH, LW, EH, ZS and CA led the design of the process evaluation. All authors contributed to the drafting, critical revision and final approval of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
Good Reporting of A Mixed Methods Study (GRAMMS).
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Leroi, I., Armitage, C.J., Collin, F. et al. A randomised controlled trial of hearing and vision support in dementia: Protocol for a process evaluation in the SENSE-Cog trial. Trials 21, 223 (2020). https://doi.org/10.1186/s13063-020-4135-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13063-020-4135-4