
Abstract
Background
In order to correctly assess the effect of intervention from stratified cluster randomized trials (CRTs), it is necessary to adjust for both clustering and stratification, as failure to do so leads to misleading conclusions about the intervention effect. We have conducted a systematic survey to examine the current practices about analysis and reporting of stratified CRTs.
Method
We used the search terms to identify the stratified CRTs from MEDLINE since the inception to July 2019. In phase 1, we screened the title and abstract for English-only studies and selected, including the main results paper of the identified protocols, for the next phase. In phase 2, we screened the full text and selected studies for data abstraction. The data abstraction form was piloted and developed using the REDCap. We abstracted data on multiple design and methodological aspects of the study including whether the primary method adjusted for both clustering and stratification, reporting of sample size, randomization, and results.
Results
We screened 2686 studies in the phase 1 and selected 286 studies for phase 2—among them 185 studies were selected for data abstraction. Most of the selected studies were two-arm 140/185 (76%) and parallel-group 165/185 (89%) trials. Among these 185 studies, 27 (15%) of them did not provide any sample size or power calculation, while 105 (57%) studies did not mention any method used for randomization within each stratum. Further, 43 (23%) and 150 (81%) of 185 studies did not provide the definition of all the strata, while more than 60% of the studies did not include all the stratification variable(s) in the flow chart or baseline characteristics table. More than half 114/185 (62%) of the studies did not adjust the primary method for both clustering and stratification.
Conclusion
Stratification helps to achieve the balance among intervention groups. However, to correctly assess the intervention effect from stratified CRTs, it is important to adjust the primary analysis for both stratification and clustering. There are significant deficiencies in the reporting of methodological aspects of stratified CRTs, which require substantial improvements in several areas including definition of strata, inclusion of stratification variable(s) in the flow chart or baseline characteristics table, and reporting the stratum-specific number of clusters and individuals in the intervention groups.
Similar content being viewed by others


Background
The random allocation of intact group of subjects—termed as clusters—into intervention groups is commonly known as cluster randomized trials (CRTs) [1]. The number of adopting CRTs to assess the effect of intervention is increasing [2]. The type of clusters can be diverse such as geographical areas [3], healthcare districts [4], and schools [5]. There are several types of experimental designs that are used to allocate clusters into intervention arms, including completely randomized, stratified, and matched-pair design. Clusters are randomly allocated to intervention groups within each stratum in a stratified design, which is suitable for small number of clusters [6].
The potential degree of similarity among the outcomes from the same cluster, measured through intra-cluster correlation coefficient (ICC), should be taken into account to assess the intervention effect from cluster randomized trials [1]. The failure to account for this correlation may yield a false positive result [1, 7]. Scientists have developed and recommended statistical methods that can be used to examine the intervention effect, while taking the clustering [1] into account. In addition, in the case of a stratified design, the statistical methods need to adjust for stratification [1]. It has been shown in the literature that variables used in the randomization process should be adjusted for in the analysis [8,9,10,11,12,13]. The absence of such adjustment in the analysis can yield large p values and wider confidence intervals, which could potentially lead to a misleading conclusion that the intervention has no effect [14]. Borhan et al. [15] empirically compared the methods for analyzing continuous data from stratified CRTs and reported that confidence intervals were wider when not adjusted for stratification, compared to when adjusted for stratification for the corresponding method.
Thus, to correctly assess the effect of intervention, it is important to adjust for stratification variables as it will yield correct p values and confidence intervals. Kahan and Morris [14] conducted a small-scale review on randomized trials on individuals and reported that only 26% of the studies adjusted for the balancing factors in their primary analysis. On the other hand, systematic reviews of CRTs demonstrated that there are significant deficiencies in the design, analysis, and reporting of CRTs [2, 16,17,18,19,20,21,22,23,24,25]. For example, in their systematic review of CRTs in primary healthcare, Eldridge et al. [21] found that 20% of the studies adjusted for clustering in sample size calculation, while 59% adjusted the analyses for clustering. Others have argued that inclusion of statistician in the research team can significantly improve the quality of reporting and analysis of CRTs [24]. Further, CONSORT statement has been extended for CRTs to guide the researchers about reporting of CRTs [26]. However, we have limited or no knowledge of how often the assessment of intervention effect from the stratified CRTs adjusted for clustering and stratification occurred.
In this study, we conducted a systematic survey to examine the analysis and reporting of stratified CRTs, which covered several methodological and reporting aspects including how often the primary method to examine the effect of intervention adjusted for both clustering and stratification, as well as whether the reporting of sample size calculations, randomization, and stratification was adequate.
Method
In this systematic survey, we identified the stratified cluster randomized trials and abstracted data on multiple study characteristics, including sample size estimation, randomization, analysis, and reporting.
Search strategy and study selection
We added the term “strati*” with the search terms (Table 1) suggested by Taljaard et al. [27] to identify the stratified cluster randomized trials from MEDLINE since the inception to July 2019. First, we performed title and abstract screening and selected the English-only studies, including the main results paper of the identified protocols. In the second phase, we screened the full text of the papers selected in the first phase and selected the studies for data abstraction. We used the protocol papers to identify the published main study results and included those in the study. In the case of multiple articles from the same trial, we included only the main study results. Selection of studies was performed using EndNote X8. PRISMA checklist [28] (Additional file 1) was used for reporting.
Data abstraction
A data abstraction form was piloted and developed using REDCap. Data abstraction form includes data on many study characteristics, including country, clinical area, setting of the study, sample size calculation, randomization, analysis of primary outcome, and reporting.
Outcome and analysis
We abstracted data on several methodological and reporting areas related to stratified CRTs, and descriptive summary, such as n (%) or mean (standard deviation [SD]) or median (first quartile [Q1], third quartile [Q3]), was used to analyze the outcomes. There were several outcomes related to the reporting of sample size or power calculation, including whether the sample size or power calculation reported, level of significance and desired power reported, and whether the sample size adjusted for the lost to follow-up. Similarly, we abstracted data on several issues related to randomization, including randomization unit, number and type of stratification variables and strata, and method used for randomization within each stratum. Several outcomes from the method of primary outcome analysis were analyzed, including type of primary outcome, unit of analysis, type of primary analysis, whether the primary method adjusted for stratification or clustering or both, how the primary method adjusted for stratification variables, whether missing data were imputed or sensitivity analysis was performed, and statistical significance of intervention effect (only for 2-arm trials). Moreover, we abstracted data on several outcomes related to reporting, including whether study flow chart or baseline characteristics table included stratification variable(s), numbers of clusters or individuals for each stratum were provided, and the estimated ICC was reported. See the “Results” section for details about the outcomes. All analyses were performed using R.
Results
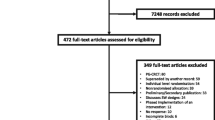
Our search produced 2686 published reports, and after initial screening followed by assessment of full text, 185 papers (all reporting 185 unique CRTs) were selected for analysis (Fig. 1).

Flow chart of study selection
The results of some basic characteristics of the selected studies are provided in Table 2. About 80% of the studies were from 2010 to 2019, while only 7 (4%) studies were from before 2000. Almost half of the studies, 48%, were one centered, and most of the studies (31%) were conducted in the USA or UK (Table 2). Among these studies, 36 (19%) and 27 (15%) of them were focused on interventions related to child development or primary care/general practices, respectively. Also, there were 36 and 38 studies that were school- or general practice-based, respectively (Table 2). In addition, the majority—140 (76%) and 165 (89%)—of the studies were 2-arm and parallel-group trials, respectively (Table 2).
One hundred and fifty-eight (85%) out of 185 studies provided sample size or power calculations, while 66% of the studies adjusted for clustering (Fig. 2). While more than 80% of the studies reported the level of significance or desired power in sample size or power calculations, only 10% of the studies reported the method used, and 28% of the studies adjusted for lost to follow-up in sample size calculations (Fig. 2). Akin to the setting of the study, almost similar numbers of studies used school or primary care/general practice as the randomization unit (Fig. 3). Almost half of the studies had one stratification variable, while only 2% of the studies had 4 or more stratification variables. In total, there were 298 stratification variables used across all included trials. About 35% (103/298) stratification variables were based on geographical location, while 17% (51/298) and 15% (46/298) were based on epidemiologic/prognostic factors and cluster size, respectively. More than half of the studies (57%; 105/185) did not provide the method used for randomization, while 23% (43/185) of the studies specified all the strata (Fig. 3).

Results of outcomes related to sample size or power calculation among all the studies (n = 185)

Results of outcomes related to randomization among all the studies (n = 185) except type of stratification variables. *NA, not available
The results of outcomes related to the primary method of analysis are provided in Table 3. The primary outcome of 83% (152/185) of the studies was continuous or binary. One hundred and forty-three (77%) studies performed individual-level analysis. More than half (52%) of the studies used an intention-to-treat approach as their primary analysis approach, while 43% of the studies did not mention their primary analysis approach (Table 3). Seventy-one (38%) studies reported primary method/effect estimate adjusted for both clustering and stratification. Among the studies that adjusted for stratification, 90% (66/73) of the studies adjusted for stratification by using them as the covariate(s) (Table 3). Thirty-eight (46%; 38/82) of the studies reported their statistically significant intervention effect, among the 2-arm studies that did not adjust their primary method for both clustering and stratification (Table 3).
The results of outcomes pertaining to reporting of outcomes are provided in Fig. 4. Only 19% (35/185) and 31% (58/185) of the studies included stratification variables in the flow chart or baseline characteristics table. Only 10% (18/185) of the studies reported stratum-specific effect estimate.

Results of reporting outcomes among all the included studies (n = 185)
Discussion
In this systematic survey, we selected 185 stratified cluster randomized trials from MEDLINE since the inception to July 2019, and found that there were significant deficiencies in the reporting of methodological aspects of stratified CRTs, and only 38% of the studies adjusted the primary method for both clustering and stratification. This result is similar to the findings of Kahan and Morris [14], as they reported 26% of the studies adjusted for balancing or stratification factors.
In order to correctly assess the effect of intervention, it is important to adjust the primary method for stratification variable(s) as well as clustering [14], which was also established from the empirical study of Borhan et al. [15]. From this systematic review, it is evident that this type of adjustment is still scarce as more than half of the studies did not adjust for both stratification variable(s) and clustering. Moreover, almost half of the studies adjusted the primary method for clustering only, while this number varies from 37 to 92% in the previous studies on the review of CRTs [2, 16,17,18,19,20,21,22,23,24].
Along with performing the adjusted analyses, we also need to focus on other areas of stratified cluster randomization trials including sample size calculation and randomization. Similar to the randomized controlled trials on individuals, it is necessary to report all the information used to calculate the sample size, including detectable difference, level of significance, and desirable power. Most importantly, sample size calculation needs to account for the clustering. In this survey, we have found 62% of the studies reported the ICC/CV used to calculate the sample size or power. This number varies from 0 to 71% in the previous reviews on CRTs [2, 16,17,18,19,20,21,22,23,24]. Furthermore, it is also necessary to report the randomization method used to allocate clusters to intervention groups within each stratum—which was not reported by more than half of the studies in this survey.
There were significant deficiencies in reporting the results from the stratified CRT. Reporting on the following areas, at minimum, would better represent and help the audience to better understand the stratified nature of this type of studies: (1) only a few studies provided the reasoning for stratification. Reporting the reasoning for stratified design and choosing the stratification variable(s) would be helpful; (2) more than 20% of the studies did not provide the definition of all the strata. For a stratified design, it is essential to report how all the strata are defined; (3) almost all the studies provided the study flow chart, while only 19% and 31% of the studies included stratification variables/strata in the flow chart or in baseline characteristics table, respectively. Inclusion of stratification variables in the flow chart or baseline characteristics table would provide the clear depiction of the design; (4) only 20% and 11% of the studies reported the stratum-specific number of clusters and individuals in the intervention groups, respectively. Thus, more attention is needed to report these numbers; (5) reporting the stratum-specific, if possible, would help the readers to know the intervention effect in each stratum.
The major strength of this study was that we used the search terms recommended by Taljaard et al. [27] to select the stratified cluster randomized trials from one of the largest database MEDLINE. Also, we included the published main trial results of the protocols selected in title and abstract screening. Furthermore, this survey was based on the time period from 1946 to 2019. The major limitation of this study is that only one reviewer conducted this survey. Despite multiple checking or best effort, it is possible that the reviewer may have failed to include some of the eligible studies.
A well-designed large-scale systematic review would depict a more complete picture about the analysis and reporting status of stratified cluster randomized trials. Following the CONSORT extension for CRTs [26] or inclusion of a statistician [24] in the study will significantly improve the quality of reporting and analysis of stratified CRTs. Furthermore, CONSORT statements for CRTs can be extended for stratified CRTs, incorporating the recommendations we made in this manuscript. This type of extension would be helpful for the researchers as it will guide them about the analysis and reporting of stratified cluster randomized trials.
Conclusion
In this systematic survey, we assessed the current practice about reporting and analysis of stratified cluster randomized trials. We found that there were substantial deficiencies in the reporting of methodological aspects of stratified cluster randomized trials. Furthermore, majority of the studies did not adjust their primary method of analysis for both clustering and stratification—which were important to assess the intervention effect for stratified cluster randomized trials. Moreover, stratified cluster randomized trials require substantial improvement in reporting such as details about sample size calculation and randomization, definition of all strata, inclusion of stratification variable(s)/strata in study flow chart or baseline characteristics table, and stratum-specific number of clusters and individuals in the intervention groups. A guideline would be helpful for researchers to enhance the transparent reporting and analysis of stratified cluster randomized trials.
References
Donner A, Klar N. Design and analysis of cluster randomization trials in health research. London: Arnold; 2000.
Bland J. Cluster randomised trials in the medical literature: two bibliometric surveys. BMC Med Res Methodol. 2004;4:21–7.
Kroeger A, Avila EV, Morison L. Insecticide impregnated curtains to control domestic transmission of cutaneous leishmaniasis in Venezuela: cluster randomized trial. Br Med J. 2002;325(7368):810–3.
Jordhoy M, Fayers P, Saltnes T, Ahlner-Elmqvist M, Jannert M, Kaasa S. A palliative-care intervention and death at home: a cluster randomized trial. Lancet. 2000;356(9233):888–93.
Mallick R, Kathard H, Borhan ASM, Pillay M, Thabane L. A cluster randomised trial of a classroom communication resource program to change peer attitudes towards children who stutter among grade 7 students. Trials. 2018;19:664.
Klar N, Donner A. The merits of matching in community intervention trials: a cautionary tale. Stat Med. 1997;16:1753–64.
Murray D, Varnell S, Blitstein J. Design and analysis of group-randomized trials: a review of recent methodological developments. Am J Public Health. 2004;94:423–32.
ICH Harmonised Tripartite Guideline. Statistical principles for clinical trials. International Conference on Harmonisation E9 Expert Working Group. Stat Med. 1999;18:1905–42.
Kahan BC, Morris TP. Improper analysis of trials randomised using stratified blocks or minimisation. Stat Med. 2012;31:328–40.
Kernan WN, Viscoli CM, Makuch RW, Brass LM, Horwitz RI. Stratified randomization for clinical trials. J Clin Epidemiol. 1999;52:19–26.
Parzen M, Lipsitz SR, Dear KBG. Does clustering affect the usual test statistics of no treatment effect in a randomized clinical trial? Biom J. 1998;40:385–402.
Raab GM, Day S, Sales J. How to select covariates to include in the analysis of a clinical trial. Control Clin Trials. 2000;21:330–42.
Scott NW, McPherson GC, Ramsay CR, Campbell MK. The method of minimization for allocation to clinical trials: a review. Control Clin Trials. 2002;23:662–74.
Kahan B, Morris T. Reporting and analysis of trials using stratified randomisation in leading medical journals: review and reanalysis. BMJ. 2012;345:e5840.
Borhan S, Mallick R, Pillay M, Kathard H, Thabane L. Sensitivity of methods for analyzing continuous outcome from stratified cluster randomized trials – an empirical comparison study. Contemp Clin Trial Commun. 2019;15:100405.
Puffer S, Torgerson D, Watson J. Evidence for risk of bias in cluster randomised trials: review of recent trials published in three general medical journals. BMJ. 2003;327(7418):785–9.
Eldridge S, Ashby D, Bennett C, Wakelin M, Feder G. Internal and external validity of cluster randomised trials: systematic review of recent trials. BMJ. 2008;336(7649):876–80.
Donner A, Brown KS, Brasher P. A methodological review of non-therapeutic intervention trials employing cluster randomization, 1979–1989. Int J Epidemiol. 1990;19(4):795–800.
Simpson JM, Klar N, Donnor A. Accounting for cluster randomization: a review of primary prevention trials, 1990 through 1993. Am J Public Health. 1995;85(10):1378–83.
Isaakidis P, Ioannidis JP. Evaluation of cluster randomized controlled trials in sub-Saharan Africa. Am J Epidemiol. 2003;158(9):921–6.
Eldridge SM, Ashby D, Feder GS, Rudnicka AR, Ukoumunne OC. Lessons for cluster randomized trials in the twenty-first century: a systematic review of trials in primary care. Clin Trials. 2004;1(1):80–90.
Bowater RJ, Abdelmalik SM, Lilford RJ. The methodological quality of cluster randomised controlled trials for managing tropical parasitic disease: a review of trials published from 1998 to 2007. Trans R Soc Trop Med Hyg. 2009;103(5):429–36.
Ivers NM, Taljaard M, Dixon S, Bennett C, McRae A, Taleban J, Skea Z, Brehaut JC, Boruch RF, Eccles MP, et al. Impact of CONSORT extension for cluster randomised trials on quality of reporting and study methodology: review of random sample of 300 trials, 2000–8. BMJ. 2011;343:d5886.
Diaz-Ordaz K, Froud R, Sheehan B, Eldridge S. A systematic review of cluster randomised trials in residential facilities for older people suggests how to improve quality. BMC Med Res Methodol. 2013;13:127.
Tokolahi E, Hocking C, Kersten P, Vandal AC. Quality and reporting of cluster randomized controlled trials evaluating occupational therapy interventions: a systematic review. OTJR (Thorofare N J). 2016;36(1):14–24.
Campbell MK, Piaggio G, Elbourne DR, Altman DG, for the CONSORT Group. Consort 2010 statement: extension to cluster randomised trials. BMJ. 2012;345:e5661.
Taljaard M, et al. Electronic search strategies to identify reports of cluster randomized trials in MEDLINE: low precision will improve with adherence to reporting standards. BMC Med Res Methodol. 2010;10:15.
Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred Reporting Items for Systematic Reviews and MetaAnalyses: the PRISMA statement. PLoS Med. 2009. https://doi.org/10.1371/journal.pmed1000097.
Funding
There was no funding for this study.
Author information
Authors and Affiliations
Contributions
SB and LT conceptualized, developed, and designed this study. SB was involved with screening, study selection, data abstraction, and preparing the results and wrote the first draft of this manuscript. All authors contributed equally to further improve this manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declared no competing interests for this study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PRISMA 2009 Checklist.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Borhan, S., Papaioannou, A., Ma, J. et al. Analysis and reporting of stratified cluster randomized trials—a systematic survey. Trials 21, 930 (2020). https://doi.org/10.1186/s13063-020-04850-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13063-020-04850-w