
Abstract
Background
Patients with Alzheimer’s disease frequently elicit neuropsychiatric symptoms as well as cognitive deficits. Above all, depression is one of the most common neuropsychiatric symptoms in Alzheimer’s disease but antidepressant drugs have not shown significant beneficial effects on it. Moreover, electroconvulsive therapy has not ensured its safety for potential severe adverse events although it does show beneficial clinical effect. Transcranial direct current stimulation can be the safe alternative of neuromodulation, which applies weak direct electrical current to the brain. Although transcranial direct current stimulation has plausible evidence for its effect on depression in young adult patients, no study has explored it in older subjects with depression in Alzheimer’s disease. Therefore, we present a study protocol designed to evaluate the safety and clinical effect of transcranial direct current stimulation on depression in Alzheimer’s disease in subjects aged over 65 years.
Method
This is a two-arm, parallel-design, randomized controlled trial, in which patients and assessors will be blinded. Subjects will be randomized to either an active or a sham transcranial direct current stimulation group. Participants in both groups will be evaluated at baseline, immediately, and 2 weeks after the intervention.
Discussion
This study investigates the safety and effect of transcranial direct current stimulation that may bring a significant impact on both depression and cognition in patients with Alzheimer’s disease, and may be useful to enhance their quality of life.
Trial registration
ClinicalTrials.gov, NCT02351388. Registered on 27 January 2015. Last updated on 30 May 2016.
Similar content being viewed by others


Background
Dementia is a disorder that is characterized by a decline in cognition in one or more cognitive domains such as learning and memory, language, executive function, complex attention, perceptual-motor, and social cognition [1]. According to the World Alzheimer Report 2015, 36 million people were living with dementia in 2010, nearly doubling every 20 years to 66 million by 2030 and to 115 million by 2050 [2]. Alzheimer’s disease (AD), the most common form of dementia in older people, is increasingly prevalent with advancing age, and the overall burden of it is substantial worldwide [3,4,5,6,7,8]. Cognitive dysfunction in AD reduces the quality of life (QOL) of patients and caregivers [9]. At the same time, neuropsychiatric symptoms (NPS) in AD compromise their QOL [10]. Depressive mood is one of the most common NPS in AD as well as agitation and apathy [11]. The prevalence rate of depression in AD is from 36.7 [12] to 47.8% [11].
However, antidepressant drugs have not shown significant beneficial effect on depression in AD. A meta-analysis demonstrated that selective serotonin reuptake inhibitors and serotonin and norepinephrine reuptake inhibitors did not show significant beneficial effect on depression in AD [13]. In addition, a randomized controlled trial (RCT) with large sample, revealed that neither sertraline nor mirtazapine showed superiority to placebo, and concluded that antidepressants should not be used first for depression in AD [14].
Electroconvulsive therapy (ECT) is one of the most promising nonpharmacological treatments for depression [15, 16]. A review article suggested that ECT does show beneficial effect in both older patients over 65 years, and in patients with dementia, but it did not conclude that ECT is a safe treatment for them [17]. A case series showed that ECT did not induce long-term cognitive deficits in older patients, but the result was not easily generalized because of confounders [18]. A chart review demonstrated that ECT produced delirium in 49% of patients with AD [19]. Moreover, a secondary analysis of data collected from a large prospective cohort study suggested that delirium can accelerate the trajectory of cognitive decline in patients with AD [20].
Transcranial direct current stimulation (tDCS) is a simple, cheap, and safe method of neuromodulation, based on the application of weak, direct electrical current to the brain through relatively large electrodes. Two electrodes are placed over the scalp, in which anodal and cathodal stimulation increases and decreases cortical excitability, respectively [21]. One RCT, in which the anodal electrode was placed over the left dorsolateral prefrontal cortex (DLPFC), showed significant effect of tDCS on the Montgomery-Asberg Depression Rating Scale (MADRS) in major depressive disorder [22]. Furthermore, another RCT, using a factorial design to sertraline/placebo and active/sham tDCS to the left DLPFC, verified that there was a significant difference in MADRS scores when comparing the combined treatment group (sertraline/active tDCS) versus sertraline only, and tDCS only versus placebo/sham tDCS [23]. In addition, a meta-analysis of individual patient data concluded that the effect size of tDCS is comparable with those reported for repetitive transcranial magnetic stimulation and antidepressant drug treatment in primary care [24]. The antidepressant effects of tDCS are based on the finding that the left DLPFC is hypoactive in depression and, hence, anodal tDCS would possibly restore prefrontal activity by increasing activity in this area [25]. One RCT demonstrated that in the motor cortex of healthy volunteers, tDCS altered cortical excitability more effectively when given daily rather than on alternate days over a 5-day period [26].
However, no study has evaluated the safety and effect of tDCS on depression in AD although one RCT assessed the effect of tDCS on apathy in AD, which did not show significant effect, possibly because of a small number of interventions (six sessions of tDCS in 2 weeks) [27]. Therefore, we present a study protocol designed to evaluate the safety and effect of tDCS on depression in AD patients over 65 years.
Method
Study design
This protocol is presented in accordance with the 2013 SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) Statement (See Additional file 1 for the populated SPIRIT Checklist and Fig. 1 for the trial schedule of enrollment, interventions, and assessments in accordance with recommended SPIRIT figure) which was developed to provide guidance in the form of a checklist of recommended items to include in a clinical trial protocol to help improve its content and quality [28]. This is a single-center trial, which will be conducted at the National Center of Neurology and Psychiatry, Tokyo, Japan. This is a two-arm, parallel-design, double-blind RCT in which patients and assessors will be blinded. Subjects will be randomized with a 1:1 ratio to either the active or the sham tDCS group with a computer-generated sequence. The superiority of active tDCS to sham tDCS will be investigated. Allocation concealment will be maintained with sealed opaque envelopes. Subjects will receive 15 consecutive 30-min applications of active/sham tDCS from Monday to Friday for 3 weeks. A participant’s allocated intervention during the trial will be revealed by the principle investigator after the study endpoint. The trial results will be communicated by the study coordinators when requested.

Schedule of enrollment, interventions, and assessments. tDCS transcranial direct current stimulation, CDR Clinical Dementia Rating, MMSE Mini Mental State Examination, GDS Geriatric Depression Scale, CSDD Cornell Scale for Depression in Dementia, NPI Neuropsychiatric Inventory, SAS Starkstein Apathy Scale, QOL-AD Quality of Life-Alzheimer’ disease, ZBI Zarit Burden Interview, ADCS-ADL Alzheimer’s Disease Cooperative Study Activities of Daily Living, CGI Clinical Global Impression
Participants
Patients enrolled in the study must follow all of the inclusion criteria below:
-
1.
Participants who meet the criteria of probable AD defined by National Institute of Neurological and Communicative Diseases and Stroke-Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) research criteria [29]
-
2.
Participants who meet the criteria of depression in AD defined by National Institute of Mental Health (NIMH) criteria [30]
-
3.
Participants who have been on a fixed dose (including participants without any prescription) of antidepressants for at least 2 weeks on the screening visit
-
4.
Participants who have been on a fixed dose (including participants not prescribed) of antidementia drugs (donepezil, rivastigmine, galantamine, and memantine) for at least 4 weeks on the screening visit
-
5.
Ambulatory participants with or without any aiding device
-
6.
Participants who have a study partner, who lives with them for at least 10 h a week to report their behavior
-
7.
Participants who sign and give consent, or whose family member provides consent on their behalf
-
8.
Participants who are community dwelling
-
9.
Participants who are over 65 years old
Patients with any of the following criteria will be excluded from the study:
-
1.
People whose cognitive deficits are better explained by another disease such as cerebral infarction, Parkinson disease, multiple sclerosis, and normotensive hydrocephalus
-
2.
A history of epilepsy
-
3.
Current treatment of antipsychotic medication
-
4.
An urgent risk of suicide or severe depression and need to be hospitalized to psychiatric units
-
5.
A history of ineffectiveness with ECT or tDCS
-
6.
People who are clinically contraindicated to receive ECT or tDCS such as having a tattoo or metal embedded in their scalp or brain
-
7.
Current treatment with benzodiazepines or antiepileptic drugs
-
8.
People who scored less than 10 on the Mini Mental State Examination (MMSE) [31] or who scored 3 or more on the Clinical Dementia Rating Scale (CDR) [32]
-
9.
People who scored less than 6 on the 15-item Geriatric Depression Scale (GDS) [33] at baseline
-
10.
People who are unable to undergo a video recording on the evaluation interview
-
11.
People who are diagnosed with concurrent delirium by clinicians.
Interventions
Direct current will be transferred by 35-cm2 saline-soaked sponge electrodes and delivered by Soterix Medical 1 x 1 Transcranial Direct Current Low-Intensity Stimulator Model 1300A. For each session, the tDCS montage will comprise placement of the anode over the left DLPFC and the cathode over the contralateral supraorbital area which corresponds to the F3 and FP2 areas, according to the International 10–20 electroencephalography system. We will apply direct current of 2 mA for 30 min/day, for 15 days over three consecutive weeks. The dose and frequency of stimulation was chosen based on previous research for depression in young adults [22].
For the sham group, the device will be turned off after 1 min of active stimulation. The electrode position and the other procedures to set up, including electrode moisture, checking the contact, will be identical. The display on the device will be kept outside participants’ visual fields as the device will be turned off without subjects noticing. A controlled study demonstrated that blinding integrity of tDCS and pharmacological treatment were comparable [34]. The raters and patients will be blinded to the treatment, and the contact between participants will be avoided to enhance the effect of study blinding.
A trained psychiatrist will administer the tDCS intervention. Since the experimenter will not be blinded, their interaction with participants will be minimized. Also, the experimenter will not participate in the assessment of outcomes or in any other aspect of the trial.
Allocated interventions will be discontinued according to the following criteria:
-
1.
In case patients cease giving their informed consent to participate
-
2.
In case a severe adverse effect is observed
-
3.
In case patients fail to undergo five consecutive sessions of tDCS
In order to improve adherence, we will provide all included patients and their study partners with costs of transportation, and will remind and reschedule all of the patients’ visits if necessary.
The following interventions will be restricted and recognized as protocol deviation during the trial:
-
1.
Adjusting the dose of antidepressant drugs except trazodone or mianserin
-
2.
Adjusting the dose of antidementia drugs
-
3.
Antiepileptic drugs
-
4.
Adjusting the dose of lithium
-
5.
Quetiapine over a dose of 50 mg/day
-
6.
Trazodone over a dose of 50 mg/day
-
7.
Mianserin over a dose of 20 mg/day
-
8.
Adjusting the dose of antipsychotic medication except quetiapine
-
9.
Benzodiazepines
Outcome measures
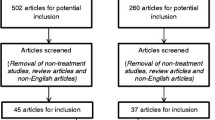
Patients will be assessed after being informed of the objectives of the study and giving their informed consent to participate (see Additional files 2 and 3). Data will be collected following an assessment that will be implemented at baseline, immediately, and 2 weeks after the end of treatment (see Fig. 2). Baseline and follow-up evaluations will be performed by experienced psychiatrists blinded to group assignments.

Flowchart summarizing the trial
The primary outcome measure is attrition rate caused by any adverse event since no study has evaluated the safety of tDCS on depression in AD. Secondary outcome measures include the MMSE, the CDR, the GDS, the Cornell Scale for Depression in Dementia (CSDD) [33], the Neuropsychiatric Inventory (NPI) [35], the Starkstein Apathy Scale (SAS) [36], the Quality of Life-Alzheimer’s Disease (QOL-AD) [37], the Zarit Burden Interview (ZBI) [38], the Alzheimer’s Disease Cooperative Study-Activities of Daily Living (ADCS-ADL) [39], and the Clinical Global Impression (CGI) [40]. The MMSE is an objective scale developed to provide a brief screening test that quantitatively assesses the severity of cognitive impairment and documents cognitive changes occurring over time [31]. The CDR is an objective scale used to characterize six domains of cognitive and functional performance applicable to Alzheimer’s disease and related dementias [32]. The GDS (self-report) and the CSDD (objective scale) are both valid screening tools for depression in older people [33]. The NPI is a proxy-reported scale developed to assess 12 neuropsychiatric disturbances common in dementia [35]. The SAS is a self-reported scale recommended to screen for, and measure, the severity of apathetic symptoms [36]. The QOL-AD is one of the most widely used self-reported dementia-specific QOL instruments in the world [37]. The ZBI is a valid and reliable caregiver-reported instrument for measuring the burden of them [38]. The ADCS-ADL is a proxy-rated scale developed to assess the ability of patients with moderate to severe dementia to perform activities of daily living [39]. The CGI is a tool used to offer a readily understood, practical measurement tool that can easily be administered by a clinician in a busy clinical practice setting [40]. To ensure the success of blinding, we will ask participants and outcome assessors at the endpoint to guess whether the treatment was active or sham.
The schedule of enrollment, interventions, and assessments is summarized in Fig. 1. Participants will be recruited by referrals of two experienced psychiatrists (ZN and YY) in the National Center of Neurology and Psychiatry. This is a pilot study to inform the design of a future full-scale randomized trial and aims to test the feasibility of conducting the study. Recruitment of a total of 20 participants, 10 for the active tDCS group and 10 for the sham tDCS group, respectively, will be deemed sufficient for a pilot study and will be affordable in our research setting. We will use a blocked randomization process, with random 4-size and 6-size blocks, in order to maintain an adequate balance in the number of subjects allocated to both groups. We expect that one or two patients can be recruited per month on average, and that it will be possible to recruit 20 participants in 20 months.
All assessors will be trained at a workshop every month. All data will be administered in the Electronic Data Capture (EDC) system. Allocation and other identifiable data of participants will be stored in a computer which does not have Internet access. Only the study coordinators and the Data Monitoring Committee can open the EDC system using passwords.
Statistical analysis
Statistical analysis on outcome measures will be conducted using STATA. We will handle missing data with a multiple imputation method as an intention-to-treat (ITT) analysis for participants who received at least one session of tDCS. We will also perform a per-protocol approach as a sensitivity analysis for the comparison of the results. For the MMSE, the CDR, the GDS, the CSDD, the NPI, the SAS, the QOL-AD, the ZBI, and the ADCS-ADL, we will use analysis of covariance (ANCOVA) regarding age, sex, severity of depression, and severity of AD at baseline as covariates. For the CGI, we will use the Wilcoxon signed-rank test. With alpha of 0.05, a two-sided p value, and power of 0.8, a 7-point CSDD difference (standard deviation = 5) will be required to create significance between groups [14].
Monitoring
A systematic review has demonstrated that the most common adverse events from tDCS are itching, tingling, headache, burning sensation, and discomfort [41]. A trained psychiatrist will check for adverse effects during/immediately after every session and evaluate the safety every week during the intervention. An independent Safety Monitoring Committee will run an interim analysis for safety when the tenth participant finishes the schedule, and will decide if the trial has to be terminated or modified. An independent Monitoring Committee will monitor the data in the EDC system every week.
Discussion
Depression is one of the most frequent NPS in patients with AD, and has a negative impact on their QOL [10]. However, neither antidepressant drugs nor ECT have been established as a persuasive treatment for it because the former has not shown significant effect [13, 14] and the latter has not ensured its safety [17,18,19,20].
As stated before, tDCS is a safe method of brain stimulation and has a plausible evidence for treating depression in young patients [22,23,24]. Given this, tDCS may be also potentially useful to ameliorate depression in older patients with AD. Nevertheless, so far no RCT has been performed for tDCS in patients with depression in AD. The RCT described in this paper concerns the safety and effect of neuromodulation by weak direct current that may have a significant impact on both depression and cognition, and may be useful for patients with depression in AD to enhance their QOL.
The topic of adherence may be regarded as a potential pitfall in this protocol. However, as mentioned before, by adding costs of transportation for all included patients and their study partners to the study budget, we plan to compensate for this situation. Also, the study coordinator will remind and reschedule all of the patients’ visits as needed.
Another limitation in this trial would be the small sample. Since this is a pilot study to inform the design of a future full-scale randomized trial and aims to test the feasibility of conducting the study, we estimated that a sample size of 20 will be sufficient and will be affordable in terms of feasibility in recruitment and study implementation. We will perform a blocked randomization to equalize the number of subjects in each group but there may be still imbalance in baseline characteristics between groups which will compromise the internal validity. Furthermore, even if tDCS shows significant effect on several outcome measures in this trial, we may not immediately generalize the result to the wider population because the sample may not directly represent it which is an issue of external validity. Hence, further RCTs with larger samples and additional evaluations will be needed.
We believe that this trial is a well-designed RCT that will investigate tDCS intervention in a way which has not yet been evaluated. Even if the results do not prove our hypothesis, the gathered data will contribute to a field which has not been widely studied.
Trial status
This study is currently recruiting participants.
Abbreviations
- AD:
-
Alzheimer’s disease
- ADCS-ADL:
-
Alzheimer’s Disease Cooperative Study Activities of Daily Living
- ANCOVA:
-
Analysis of covariance
- CDR:
-
Clinical Dementia Rating
- CGI:
-
Clinical Global Impression
- CSDD:
-
Cornell Scale for Depression in Dementia
- DLPFC:
-
Dorsolateral prefrontal cortex
- ECT:
-
Electroconvulsive therapy
- EDC:
-
Electronic Data Capture
- GDS:
-
Geriatric Depression Scale
- ITT:
-
Intention-to-treat
- MADRS:
-
Montgomery-Asberg Depression Rating Scale
- MMSE:
-
Mini Mental State Examination
- NIMH:
-
National Institute of Mental Health
- NINCDS-ADRDA:
-
National Institute of Neurological and Communicative Diseases and Stroke-Alzheimer’s Disease and Related Disorders Association
- NPI:
-
Neuropsychiatric Inventory
- NPS:
-
Neuropsychiatric symptoms
- QOL:
-
Quality of life
- QOL-AD:
-
Quality of Life-Alzheimer’ disease
- RCT:
-
Randomized controlled trial
- SAS:
-
Starkstein Apathy Scale
- SPIRIT:
-
Standard Protocol Items: Recommendations for Interventional Trials
- ZBI:
-
Zarit Burden Interview
References
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Arlington: American Psychiatric Association; 2013.
Alzheimer’s Disease International. World Alzheimer Report 2015 The global impact of dementia. An analysis of prevalence, incidence, cost and trends. 2015
Rocca WA, Petersen RC, Knopman DS, Hebert LE, Evans DA, Hall KS, et al. Trends in the incidence and prevalence of Alzheimer’s disease, dementia, and cognitive impairment in the United States. Alzheimers Dement J Alzheimers Assoc. 2011;7(1):80–93.
Ganguli M, Hendrie HC. Screening for cognitive impairment and depression in ethnically diverse older populations. Alzheimer Dis Assoc Disord. 2005;19(4):275–8.
Llibre Rodriguez JJ, Ferri CP, Acosta D, Guerra M, Huang Y, Jacob KS, et al. Prevalence of dementia in Latin America, India, and China: a population-based cross-sectional survey. Lancet Lond Engl. 2008;372(9637):464–74.
Prince M, Bryce R, Albanese E, Wimo A, Ribeiro W, Ferri CP. The global prevalence of dementia: a systematic review and metaanalysis. Alzheimers Dement J Alzheimers Assoc. 2013;9(1):63–75.e2.
Sosa-Ortiz AL, Acosta-Castillo I, Prince MJ. Epidemiology of dementias and Alzheimer’s disease. Arch Med Res. 2012;43(8):600–8.
Hebert LE, Weuve J, Scherr PA, Evans DA. Alzheimer disease in the United States (2010–2050) estimated using the 2010 census. Neurology. 2013;80(19):1778–83.
León-Salas B, Olazarán J, Muñiz R, González-Salvador MT, Martínez-Martín P. Caregivers’ estimation of patients’ quality of life (QoL) in Alzheimer’s disease (AD): an approach using the ADRQL. Arch Gerontol Geriatr. 2011;53(1):13–8.
León-Salas B, Olazarán J, Cruz-Orduña I, Agüera-Ortiz L, Dobato JL, Valentí-Soler M, et al. Quality of life (QoL) in community-dwelling and institutionalized Alzheimer’s disease (AD) patients. Arch Gerontol Geriatr. 2013;57(3):257–62.
Acosta-Castillo GI, Luisa Sosa A, Orozco R, Borges G. Neuropsychiatric symptoms in older adults with dementia and their relationship to disease severity. Rev Investig Clin Organo Hosp Enfermedades Nutr. 2012;64(4):354–63.
Aalten P, Verhey FRJ, Boziki M, Bullock R, Byrne EJ, Camus V, et al. Neuropsychiatric syndromes in dementia. Results from the European Alzheimer Disease Consortium: part I. Dement Geriatr Cogn Disord. 2007;24(6):457–63.
Nelson JC, Devanand DP. A systematic review and meta-analysis of placebo-controlled antidepressant studies in people with depression and dementia. J Am Geriatr Soc. 2011;59(4):577–85.
Banerjee S, Hellier J, Dewey M, Romeo R, Ballard C, Baldwin R, et al. Sertraline or mirtazapine for depression in dementia (HTA-SADD): a randomised, multicentre, double-blind, placebo-controlled trial. Lancet Lond Engl. 2011;378(9789):403–11.
Gábor G, László T. The efficacy of ECT treatment in depression: a meta-analysis. Psychiatr Hung Magy Pszichiatriai Tarsasag Tudomanyos Folyoirata. 2005;20(3):195–200.
Pagnin D, de Queiroz V, Pini S, Cassano GB. Efficacy of ECT in depression: a meta-analytic review. J ECT. 2004;20(1):13–20.
Oudman E. Is electroconvulsive therapy (ECT) effective and safe for treatment of depression in dementia? A short review. J ECT. 2012;28(1):34–8.
Hausner L, Damian M, Sartorius A, Frölich L. Efficacy and cognitive side effects of electroconvulsive therapy (ECT) in depressed elderly inpatients with coexisting mild cognitive impairment or dementia. J Clin Psychiatry. 2011;72(1):91–7.
Rao V, Lyketsos CG. The benefits and risks of ECT for patients with primary dementia who also suffer from depression. Int J Geriatr Psychiatry. 2000;15(8):729–35.
Fong TG, Jones RN, Shi P, Marcantonio ER, Yap L, Rudolph JL, et al. Delirium accelerates cognitive decline in Alzheimer disease. Neurology. 2009;72(18):1570–5.
Brunoni AR, Nitsche MA, Bolognini N, Bikson M, Wagner T, Merabet L, et al. Clinical research with transcranial direct current stimulation (tDCS): challenges and future directions. Brain Stimulat. 2012;5(3):175–95.
Loo CK, Alonzo A, Martin D, Mitchell PB, Galvez V, Sachdev P. Transcranial direct current stimulation for depression: 3-week, randomised, sham-controlled trial. Br J Psychiatry J Ment Sci. 2012;200(1):52–9.
Brunoni AR, Valiengo L, Baccaro A, Zanão TA, de Oliveira JF, Goulart A, et al. The sertraline vs. electrical current therapy for treating depression clinical study: results from a factorial, randomized, controlled trial. JAMA Psychiat. 2013;70(4):383–91.
Brunoni AR, Moffa AH, Fregni F, Palm U, Padberg F, Blumberger DM, et al. Transcranial direct current stimulation for acute major depressive episodes: meta-analysis of individual patient data. Br J Psychiatry J Ment Sci. 2016;208(6):522–31.
Brunoni AR, Teng CT, Correa C, Imamura M, Brasil-Neto JP, Boechat R, et al. Neuromodulation approaches for the treatment of major depression: challenges and recommendations from a working group meeting. Arq Neuropsiquiatr. 2010;68(3):433–51.
Alonzo A, Brassil J, Taylor JL, Martin D, Loo CK. Daily transcranial direct current stimulation (tDCS) leads to greater increases in cortical excitability than second daily transcranial direct current stimulation. Brain Stimulat. 2012;5(3):208–13.
Suemoto CK, Apolinario D, Nakamura-Palacios EM, Lopes L, Leite REP, Sales MC, et al. Effects of a non-focal plasticity protocol on apathy in moderate Alzheimer’s disease: a randomized, double-blind, sham-controlled trial. Brain Stimulat. 2014;7(2):308–13.
Chan A-W, Tetzlaff JM, Gøtzsche PC, Altman DG, Mann H, Berlin JA, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ. 2013;346, e7586.
McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 1984;34(7):939–44.
Teng E, Ringman JM, Ross LK, Mulnard RA, Dick MB, Bartzokis G, et al. Diagnosing depression in Alzheimer disease with the national institute of mental health provisional criteria. Am J Geriatr Psychiatry Off J Am Assoc Geriatr Psychiatry. 2008;16(6):469–77.
Tombaugh TN, McIntyre NJ. The Mini-Mental State Examination: a comprehensive review. J Am Geriatr Soc. 1992;40(9):922–35.
Morris JC. The Clinical Dementia Rating (CDR): current version and scoring rules. Neurology. 1993;43(11):2412–4.
Kørner A, Lauritzen L, Abelskov K, Gulmann N, Marie Brodersen A, Wedervang-Jensen T, et al. The Geriatric Depression Scale and the Cornell Scale for Depression in Dementia. A validity study. Nord J Psychiatry. 2006;60(5):360–4.
Brunoni AR, Schestatsky P, Lotufo PA, Benseñor IM, Fregni F. Comparison of blinding effectiveness between sham tDCS and placebo sertraline in a 6-week major depression randomized clinical trial. Clin Neurophysiol Off J Int Fed Clin Neurophysiol. 2014;125(2):298–305.
Cummings JL. The Neuropsychiatric Inventory: assessing psychopathology in dementia patients. Neurology. 1997;48(5 Suppl 6):S10–16.
Pedersen KF, Alves G, Larsen JP, Tysnes O-B, Møller SG, Brønnick K. Psychometric properties of the Starkstein Apathy Scale in patients with early untreated Parkinson disease. Am J Geriatr Psychiatry Off J Am Assoc Geriatr Psychiatry. 2012;20(2):142–8.
Wolak-Thierry A, Novella J-L, Barbe C, Morrone I, Mahmoudi R, Jolly D. Comparison of QoL-AD and DQoL in elderly with Alzheimer’s disease. Aging Ment Health. 2015;19(3):274–8.
Bédard M, Molloy DW, Squire L, Dubois S, Lever JA, O’Donnell M. The Zarit Burden Interview: a new short version and screening version. Gerontologist. 2001;41(5):652–7.
Niina R, Honma A, Sugai Y. Reliability, validity, and utility of Japanese version of the SIB and the modified ADCS-ADL. Rounen Seishin Igaku. 2005-6;16(6);683-91. Japanese.
Busner J, Targum SD. The Clinical Global Impressions Scale. Psychiatry Edgmont. 2007;4(7):28–37.
Brunoni AR, Amadera J, Berbel B, Volz MS, Rizzerio BG, Fregni F. A systematic review on reporting and assessment of adverse effects associated with transcranial direct current stimulation. Int J Neuropsychopharmacol. 2011;14(8):1133–45.
Acknowledgements
Not applicable.
Funding
Grants-in-Aid for Encouragement of Young Scientists (category B, 26860958), Japan Society for the Promotion of Science, Ministry of Education, Culture, Sports, Science and Technology, Japan.
Availability of data and materials
Not applicable.
Authors’ contributions
ZN developed the design and methodology, developed the analysis plan, and reviewed and commented on drafts of the protocol of the paper. YY developed the original concept of the trial, drafted the original protocol, and adapted the trial proposal as a protocol paper. Both authors contributed to drafting the article, and read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
The protocol was presented to an Institutional Review Board for approval (National Center of Neurology and Psychiatry Ethics Committee, A2014-086). The principal investigator, the research coordinator, or the research assistant will be responsible for conducting the informed consent process with all the study participants. All subjects must give consent in order to participate in the trial. Any relevant changes in the study protocol and/or the informed consent will be sent to the Institutional Review Board as a protocol amendment. All the subjects’ identities will be protected with an individual code which only the principal investigator has access to. The protocol was registered in ClinicalTrials.gov before starting the trial.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Additional files
Additional file 1:
SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) 2013 Checklist: recommended items to address in a clinical trial protocol and related documents. (DOC 121 kb)
Additional file 2:
Consent Form (translated to English). (DOC 44 kb)
Additional file 3:
Information Sheet (translated to English). (DOCX 424 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Narita, Z., Yokoi, Y. Transcranial direct current stimulation for depression in Alzheimer’s disease: study protocol for a randomized controlled trial. Trials 18, 285 (2017). https://doi.org/10.1186/s13063-017-2019-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13063-017-2019-z