
Abstract
Background
When chemotherapy is indicated in patients with early breast cancer, regimens that contain anthracyclines and taxanes are established standard treatments. Gemcitabine has shown promising effects on the response and prognosis in patients with metastatic breast cancer. The SUCCESS-A trial (NCT02181101) examined the addition of gemcitabine to a standard chemotherapy regimen in high-risk early breast cancer patients.
Methods
A total of 3754 patients with at least one of the following characteristics were randomly assigned to one of the two treatment arms: nodal positivity, tumor grade 3, age ≤ 35 years, tumor larger than 2 cm, or negative hormone receptor status. The treatment arms received either three cycles of 5-fluorouracil, epirubicin, and cyclophosphamide, followed by three cycles of docetaxel (FEC → Doc); or three cycles of FEC followed by three cycles of docetaxel and gemcitabine (FEC → Doc/Gem). The primary study aim was disease-free survival (DFS), and the main secondary objectives were overall survival (OS) and safety.
Results
No differences were observed in the 5-year DFS or OS between FEC → Doc and FEC → Doc/Gem. The hazard ratio was 0.93 (95% CI, 0.78 to 1.12; P = 0.47) for DFS and 0.94 (95% CI, 0.74 to 1.19; P = 0.60) for OS. For patients treated with FEC → Doc and FEC → Doc/Gem, the 5-year probabilities of DFS were 86.6% and 87.2%, and the 5-year probabilities of OS were 92.8% and 92.5%, respectively.
Conclusion
Adding gemcitabine to a standard chemotherapy does not improve the outcomes in patients with high-risk early breast cancer and should therefore not be included in the adjuvant treatment setting.
Trial registration
Clinicaltrials.gov NCT02181101 and EU Clinical Trials Register EudraCT 2005-000490-21. Registered September 2005.
Similar content being viewed by others

Introduction
In research on breast cancer (BC), considerable effort has been put into identifying predictive and prognostic markers to assist in decision-making for or against chemotherapy [1, 2]. However, chemotherapy continues to be one of the main treatment options for patients with unfavorable prognostic factors [3, 4]. During the last few decades, the prognosis for BC patients has been substantially improved through the introduction of chemotherapy using cyclophosphamide, methotrexate, and fluorouracil (CMF), and subsequently the introduction of anthracyclines and taxanes [5]. At the time of recruitment for the SUCCESS-A trial, the sequence of 5-fluoroucacil, epirubicin, and cyclophosphamide (FEC) followed by docetaxel (Doc) was regarded as one of the standard chemotherapy regimens for patients with high-risk early BC, after the regimen had been tested in several studies [6,7,8], and FEC → Doc showed improved overall survival (OS) in node-positive patients [9]. However, with a 5-year disease-free survival (DFS) probability of approximately 73% treatment for these patients still needed substantial improvement, for instance with the help of active agents from the metastatic setting.
In the metastatic setting, there were promising results for the addition of gemcitabine to taxanes with regard to tumor response, time to progression, and OS [10]. Partial and complete response rates were 26% (95%CI, 21%–32%) in patients receiving paclitaxel monotherapy and 41% (95% CI, 35%–47%) in those treated with addition of gemcitabine (Gem). This benefit contributed to advantages in time to progression and OS [10]. A meta-analysis summarized additional smaller studies and came to the same conclusion: the addition of gemcitabine improves the response and prognosis in first-line treatments, but not for patients receiving later treatment lines [11]. Thus, gemcitabine seemed to be a promising candidate for improvement of adjuvant cytotoxic therapy as it showed good efficacy as a first-line treatment in the metastatic setting and—unlike most other agents—was even associated with an OS benefit [10,11,12,13]. Therefore, the aim of the SUCCESS-A trial was to compare efficacy of standard chemotherapy to standard chemotherapy with the addition of gemcitabine in relation to DFS and OS in patients with high-risk early BC.
Methods
Study design
SUCCESS-A (NCT02181101) was an open-label, multicenter phase III randomized study and was conducted as an investigator-initiated trial in Germany that enrolled patients ≥ 18 years with an invasive BC and a high recurrence risk, defined as positive lymph nodes, large tumor (pT2/pT3), high tumor grade (G3), negative hormone-receptor status, or young age (≤ 35 years) (see Appendix A for a complete list of inclusion and exclusion criteria). All patients provided written informed consent before entering the study, which was approved by all of the relevant ethics committees in Germany and conducted in accordance with the Declaration of Helsinki.
The SUCCESS-A trial had also an affiliated translational research project with focus on circulating tumor cells, serum tumor marker, and pharmacogenetics [14,15,16,17].
Randomization and treatment
Patients were treated with three cycles of FEC (500/100/500 mg/m2) followed by either three cycles of docetaxel (100 mg/m2, q3w) (FEC → Doc) or gemcitabine (1000 mg/m2 on days 1 and 8) and docetaxel (75 mg/m2, q3w) (FEC → Doc/Gem). The randomization ratio was 1:1, and the stratification factors were lymph node status (pN0/pN1/pN2/pN3), hormone-receptor status (negative/positive), tumor grade (G1/G2–G3), menopausal status (pre-/postmenopausal), and HER2 status (negative/positive/unknown). Dose reductions/delays were prespecified as per protocol (Appendix B). There was an additional randomization to treatment with 2 versus 5 years of zoledronate after chemotherapy. Randomization was performed by fax or electronically via internet by the appointed clinical research organization.
Further and supportive therapies
Antihormonal and HER2 treatment were prespecified as per protocol: premenopausal, HRS-positive women received tamoxifen for 5 years (± goserelin for the first 2 years in women < 40 years), postmenopausal patients only for 2 years, followed by anastrozole for 3 years. HER2-positive patients received trastuzumab for 1 year after chemotherapy completion. The primary surgery had to result in complete resection of the tumor (R0). Axillary surgery was performed in accordance with the national guidelines (either as sentinel node biopsy or lymph node dissection) as was radiotherapy [18, 19].
End points, follow-up, and data capture
DFS and OS were defined according to the STEEP system [20]. DFS was defined as the period from the date of randomization to the earliest date of disease progression (distant metastasis, local and contralocal recurrence, and secondary primary tumors or death from any cause) or to the last date on which the patient was known to be disease-free (censored). Non-invasive (in situ) cancer events were excluded. OS was defined as the time from randomization to death from any cause or to the last date on which the patient was known to be alive (censored). The maximum observation time was 5.5 years (6 months of chemotherapy followed by 5 years of treatment with zoledronate). For assessment of survival and recurrence, the patients were followed up at the study sites at 3-month intervals for the first 3 years, and every 6 months thereafter.
Sample size calculation
The sample size calculations were based on a study comparing six cycles of FEC with three cycles of FEC followed by three cycles of docetaxel, which showed that treatment with FEC → Doc would result in a 5-year DFS probability of 78.3% [9]. An improvement by 4% from 78.3 to 82.3% for FEC → Doc/Gem patients was considered to be clinically relevant. On this basis, it was calculated that 743 events would be required to achieve 80% power to show a significant difference in the DFS using the log-rank test and the Wald test in a simple Cox proportional hazards model.
Statistical methods
The primary objective was to compare the DFS, and the secondary the OS between the two treatment groups (based on the intention-to-treat population). Survival rates were estimated using the Kaplan–Meier product limit method. Simple Cox regression models were fitted to estimate hazard ratios (HRs). For sensitivity analysis, similar analyses were performed for the end points of distant metastasis-free survival and BC-specific survival.
To get HRs adjusted for well-known prognostic factors, a mixed-effects Cox model was fitted with the study center as a random effect and the following predictors as fixed effects: age (continuous), body mass index (BMI; continuous), tumor stage (ordinal; pT1/pT2/pT3/pT4), tumor grade (ordinal; G1/G2/G3), lymph node status (categorical; pN0/pN+), tumor type (categorical; ductal/lobular/other) and receptor status for estrogen, progesterone, and HER2 (each categorical; negative/positive). This model was compared with a mixed-effects Cox model with the same predictors and additionally the treatment arm and its interactions with these predictors using the likelihood ratio test. In case of significance, interaction tests were performed to examine the significance of subgroup-specific variation in treatment effects. Missing predictor values were imputed (median value of continuous or integer predictors, the most common value of categorical or ordinal predictors), and continuous predictors were used as natural cubic spline functions, as done before [21].
All of the tests were two-sided, and a P value of < 0.05 was regarded as statistically significant. Calculations were carried out using the R system for statistical computing, version 3.0.1 (R Development Core Team, Vienna, Austria, 2013).
Results
Patients
From 2005–2007, 3754 patients from 251 study centers were randomly allocated to treatment groups (1898 FEC → Doc, 1856 FEC → Doc/Gem). The primary intention-to-treat analysis included all randomized patients. Sixty-four patients (37 FEC → Doc, 27 FEC → Doc/Gem) never started chemotherapy. A total of 3395 (90.4%) patients completed six cycles of chemotherapy, with 1728 (91.0%) receiving FEC → Doc and 1667 (89.9%) FEC → Doc/Gem. After three initial cycles of FEC, 1779 (94.9%) patients in the FEC → Doc/Gem arm started treatment with Doc/Gem and 1801 (95.9%) patients in the FEC → Doc arm started Doc monotherapy (Fig. 1).

Patient flow chart (Consolidated Standards of Reporting Trials/CONSORT diagram)
Dose reductions and delays were necessary in 261 (13.8%) and 40 (2.1%) patients in the FEC → Doc and in 427 (23.0%) and 95 (5.1%) patients in the FEC → Doc/Gem group, respectively.
Baseline characteristics were complete for 97.3% of patients. Missing values for each variable were below 1.0%, with the exception of HER2 at 2.2%. Table 1 lists the patient characteristics in each treatment arm. The median follow-up periods for DFS were 5.2 (FEC → Doc) and 5.3 years (FEC → Doc/Gem), while for OS it was 5.3 years in both arms. Overall, 269 patients died during the study, 140 in the FEC → Doc and 129 in the FEC → Doc/Gem group. The numbers of patients with distant metastases in the two groups were 183 and 165, respectively, while corresponding numbers of local recurrences were 51 and 45, respectively, resulting in total numbers of DFS events of 239 and 219, respectively.
Main analysis
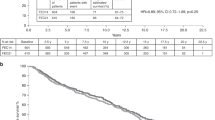
The study did not show any significant differences between the treatment arms, neither regarding DFS (HR = 0.93; 95%CI, 0.78–1.12; P = 0.47) nor OS (HR = 0.94; 95%CI, 0.74–1.19; P = 0.60); HR not adjusted. The 5-year DFS rates were 86.6% and 87.2% and the OS rates 92.8% and 92.5% in the FEC → Doc and FEC → Doc/Gem arms, respectively (see Table 2 and Fig. 2). In addition, no differences between the treatment arms were observed either for distant metastasis-free survival (HR = 0.92; 95%CI, 0.74–1.13; P = 0.43) or BC-specific survival (HR = 0.92; 95%CI, 0.71–1.20; P = 0.55).

Kaplan–Meier curves for a disease-free survival relative to treatment arm and Kaplan–Meier curves for b overall survival relative to treatment arm
Further analyses
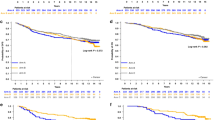
Additional analyses taking into account well-known predictors for survival showed that no treatment effects were evident, neither for all patients nor within any specific subgroups of patients (P = 0.41 for DFS, P = 0.06 for OS; likelihood ratio tests). Although global likelihood ratio tests were not significant (and therefore interaction tests were not performed; see “Statistical methods”), there was some variation in the subgroups in the estimate of the treatment effect (subgroup-specific hazard ratios are shown in Fig. 3a for DFS and Fig. 3b for OS).

Hazard ratios for the treatment arm (FEC → Doc/Gem versus FEC → Doc) in various subgroups relative to disease-free survival (a) and overall survival (b). Although there was some variation in the estimate of the treatment effect of FEC → Doc/Gem, the P values in the global likelihood ratio tests were nonsignificant. Continuous predictors were evaluated at the first decile (“low”), at the median, and at the ninth decile (“high”)
Safety
Adverse events (AEs) occurred in 1803 (96.9%) of 1861 patients receiving FEC → Doc and 1800 (98.4%) of 1829 patients treated with FEC → Doc/Gem. Serious AEs occurred in 664 (35.8%) of the patients on FEC → Doc and 706 (37.2%) of those on FEC → Doc/Gem. AEs leading to treatment discontinuation occurred in 53 (2.8%) of the FEC → Doc and 67 (3.7%) of the FEC → Doc/Gem patients. The most common AEs in FEC treatment (cycles 1–3, both groups, all grades) were leukopenia (67.0%), alopecia (65.4%), and nausea (53.6%). Leukopenia (39.1%) and neutropenia (27.8%) were the most common grade 3 or 4 AEs during cycles 1–3. During cycles 4–6, leukopenia and anemia were the most common AEs in both groups (Doc and Doc/Gem). Granulocyte-colony stimulating factor (G-CSF) support was received by 24.3% of patients in the FEC → Doc group and by 23.4% of patients in the FEC → Doc/Gem group during the first three cycles. The corresponding values for the second three cycles were 36.3% and 57.8%. Grade 3 or 4 AEs that occurred more often with Doc/Gem than with Doc were leukopenia, nausea, anemia, serum glutamate pyruvate transaminase (SGPT) elevation, fatigue, and thrombopenia [22]. More detailed information on toxicity with extensive table for grade 3/4 AEs, information on death during the trial, long-term safety, use of G-CSF, and patient-reported quality of life are already published separately [22, 23].
Discussion
This randomized phase III trial did not demonstrate any improvement in outcome with the addition of gemcitabine to FEC → Doc for early BC. DFS and OS were almost identical in the randomization arms, even in subgroup analyses, but toxicity was significantly higher in the FEC → Doc/Gem arm [22]. Thus, addition of gemcitabine does not contribute to further improvement of adjuvant cytotoxic treatment in those patients.
Regarding the dose of gemcitabine used in SUCCESS-A, we do not assume any negative impact by the chosen Gem-dosis on the presented outcome as the results of SUCCESS-A are complementary to the adjuvant and neoadjuvant studies tAnGo, Neo-tAnGo, NSAPB-B38, and NSABP-B40 testing gemcitabine [24,25,26,27,28]. It should be noted that Neo-tAnGo and NSABP-B38 used the highest dose intensity (1000 mg/m2/week) [26, 28], while tAnGo had a dose intensity of 833 mg/m2/week [27] and NSABP-B40 and SUCCESS-A used a dose intensity of 666 mg/m2/week [24, 25]. Although it might be hypothesized that these relevant differences in gemcitabine dose intensity may influence efficacy, there are two studies at each end of the dose intensity range (Neo-tAnGo/NSABP-B38 with a high and NSABP-B40/SUCCESS-A with a low dose) uniformly showing no improvement in the prognosis with either application scheme or dose [24, 26, 28]. While these results do not support the use of Gemcitabine in the (neo)adjuvant setting, the observed phenomenon is already known as several agents showing efficacy in the metastatic setting failed to become established in treatment for early BC like capecitabine [29,30,31] or lapatinib [32].
Though this study prospectively randomized more than 3700 patients within a national phase III trial and thereby is one of the largest performed clinical trial for breast cancer in Germany ever, limitations need to be clearly addressed. As the number of expected events was much higher than the number of observed events, the study is formally underpowered. However, as the presented results are unambiguous, we do not expect any relevant bias due to the lower rate of events. As breast cancer follow-up usually consists of 10 years due to well-known late recurrences, the study follow-up with only 5 years is quite short and so a potentially relevant proportion of disease recurrences might have been missed due to their later appearance. Furthermore, the definition of DFS used for the SUCCESS-A trial including contralateral invasive disease recurrence (according to the STEEP system [20]) might affect the final interpretation, as these recurrences might represent new primary cancers and not a recurrence of the initially treated cancer. The non-subtype based study design with inclusion of more than 3000 patients does not represent the current trend in oncology any more. More recent clinical trials for improvement of cancer therapy usually include patients with well-defined biological subtypes and predictive biomarkers such as genomics that potentially can identify patients who may benefit from a given treatment. Furthermore, none of the stratification factors was a pre-specified factor powered to show a difference in hazard ratio.
In addition, also some data published after the start of the SUCCESS-A study affect the interpretation of the present results in terms of new standard chemotherapy regimens. Although FEC → Doc is regarded as a highly active chemotherapy regimen in high-risk BC patients, using 5-FU may not be necessary in the adjuvant treatment of BC. During the development of chemotherapies, FEC was introduced by replacing methotrexate in the commonly used CMF scheme [33], and later, the omission of 5-FU was tested [34]. In the GIM-2 study with node-positive patients, adding 5-FU to a regimen with epirubicin and cyclophosphamide followed by paclitaxel did not improve the DFS [34]. In clinical practice, weekly paclitaxel may also be used more often than three-weekly docetaxel as weekly paclitaxel results in a longer OS than using either paclitaxel or docetaxel every 3 weeks or docetaxel weekly [35]. Although FEC → Doc is not the preferred choice of chemotherapy in the adjuvant situation anymore, the used chemotherapy backbone in SUCCESS-A consisting of an anthracycline-taxane-containing chemotherapy regimen is still standard of care in breast cancer treatment. The present study—along with the NSAPB-B38/40 and tAnGo/Neo-tAnGo trials—clearly provides solid evidence that adding gemcitabine to chemotherapy in the adjuvant setting does not improve the prognosis for patients with BC.
Further progress in systematic treatment of oncological patients will unlikely come from large-scale phase III studies including thousands of patients. Due to high toxicity with potentially severe long-term morbidity, use of chemotherapy and also number of applicated cytotoxic agents should be reduced and restricted to those patients who clearly benefit from those therapies. Molecular tests based on multigene expression profiling indicated that a large proportion of patients might not need chemotherapy at all [1, 2], and further research is focused on identification of high-risk patients and of those patient groups most likely to benefit from a specific treatment.
However, as long as there are no specific molecular profiles or predictive factors for gemcitabine-related efficacy identified, gemcitabine is not used for the overall population of adjuvant high-risk BC patients. With the presented results of SUCCESS-A, the role of gemcitabine as an added agent in adjuvant chemotherapy regimen is clearly and finally determined, as the addition of gemcitabine did not show improved survival outcomes, but was associated with increased toxicity.
Conclusion
Within the phase III SUCCESS-A trial, 3754 high-risk early breast cancer patients were randomized for adjuvant chemotherapy. Thereby, the addition of gemcitabine to standard chemotherapy (FEC/DOC) was analyzed. Adding gemcitabine to a standard chemotherapy does not improve the outcomes in patients with high-risk early breast cancer and should therefore not be included in the adjuvant treatment setting.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AE:
-
Adverse event
- ANC:
-
Absolute neutrophil count
- BC:
-
Breast cancer
- BMI:
-
Body mass index
- CI:
-
Confidence interval
- CMF:
-
Cyclophosphamide, methotrexate, and fluorouracil
- CTC:
-
Circulating tumor cells
- DFS:
-
Disease-free survival
- Doc:
-
Docetaxel
- ER:
-
Estrogen receptor
- FEC:
-
5-Fluoroucacil, epirubicin and cyclophosphamide
- FEC-Doc:
-
5-Fluorouracile, epirubicin, cyclophosphamide-docetaxel
- FEC-Doc/Gem:
-
5-Fluorouracile, epirubicin, cyclophosphamide-docetaxel, gemcitabine
- 5-FU:
-
5-Fluorouracil
- G-CSF:
-
Granulocyte-colony stimulating factor
- Gem:
-
Gemcitabine
- HER2:
-
Human epidermal growth factor receptor 2
- HR:
-
Hazard ratio
- HRS:
-
Hormone receptor status
- OS:
-
Overall survival
- PR:
-
Progesterone receptor
- SGPT:
-
Serum glutamate pyruvate transaminase
References
Sparano JA, Gray RJ, Makower DF, et al. Adjuvant chemotherapy guided by a 21-gene expression assay in breast cancer. N Engl J Med. 2018;379(2):111–21. https://doi.org/10.1056/NEJMoa1804710.
Cardoso F, van’t Veer LJ, Bogaerts J, et al. 70-gene signature as an aid to treatment decisions in early-stage breast cancer. N Engl J Med. 2016;375(8):717–29. https://doi.org/10.1056/NEJMoa1602253.
Goldhirsch A, Wood WC, Coates AS, et al. Strategies for subtypes—dealing with the diversity of breast cancer: highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011. Ann Oncol. 2011;22(8):1736–47. https://doi.org/10.1093/annonc/mdr304.
Goldhirsch A, Winer EP, Coates AS, et al. Personalizing the treatment of women with early breast cancer: highlights of the St Gallen international expert consensus on the primary therapy of early breast Cancer 2013. Ann Oncol. 2013;24(9):2206–23. https://doi.org/10.1093/annonc/mdt303.
Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) EBCTCG, Peto R, Davies C, et al. Comparisons between different polychemotherapy regimens for early breast cancer: meta-analyses of long-term outcome among 100,000 women in 123 randomised trials. Lancet (London, England). 2012;379(9814):432–44. https://doi.org/10.1016/S0140-6736(11)61625-5.
Adlard JW, Dodwell DJ. Optimum anthracycline-based chemotherapy for early breast cancer. Lancet Oncol. 2001;2(8):469–74. https://doi.org/10.1016/S1470-2045(01)00452-1.
Coombes RC, Bliss JM, Wils J, et al. Adjuvant cyclophosphamide, methotrexate, and fluorouracil versus fluorouracil, epirubicin, and cyclophosphamide chemotherapy in premenopausal women with axillary node-positive operable breast cancer: results of a randomized trial. The International Collab. J Clin Oncol. 1996;14(1):35–45.
Levine MN, Pritchard KI, Bramwell VHC, et al. Randomized trial comparing cyclophosphamide, epirubicin, and fluorouracil with cyclophosphamide, methotrexate, and fluorouracil in premenopausal women with node-positive breast cancer: update of National Cancer Institute of Canada Clinical Trials Group Trial MA5. J Clin Oncol. 2005;23(22):5166–70. https://doi.org/10.1200/JCO.2005.09.423.
Roché H, Fumoleau P, Spielmann M, et al. Sequential adjuvant epirubicin-based and docetaxel chemotherapy for node-positive breast cancer patients: the FNCLCC PACS 01 trial. J Clin Oncol. 2006;24(36):5664–71. https://doi.org/10.1200/JCO.2006.07.3916.
Albain KS, Nag SM, Calderillo-Ruiz G, et al. Gemcitabine plus paclitaxel versus paclitaxel monotherapy in patients with metastatic breast cancer and prior anthracycline treatment. J Clin Oncol. 2008;26(24):3950–7. https://doi.org/10.1200/JCO.2007.11.9362.
Hu Q, Jiang J-X, Luo L, et al. A systematic review of gemcitabine and taxanes combination therapy randomized trials for metastatic breast cancer. Springerplus. 2014;3:293. https://doi.org/10.1186/2193-1801-3-293.
Zielinski C, Beslija S, Mrsic-Krmpotic Z, et al. Gemcitabine, epirubicin, and paclitaxel versus fluorouracil, epirubicin, and cyclophosphamide as first-line chemotherapy in metastatic breast cancer: a Central European Cooperative Oncology Group International, multicenter, prospective, randomized phase III trial. J Clin Oncol. 2005;23(7):1401–8. https://doi.org/10.1200/JCO.2005.12.106.
Dent S, Messersmith H, Trudeau M. Gemcitabine in the management of metastatic breast cancer: a systematic review. Breast Cancer Res Treat. 2008;108(3):319–31. https://doi.org/10.1007/s10549-007-9610-z.
Rack B, Jückstock J, Trapp E, et al. CA27.29 as a tumour marker for risk evaluation and therapy monitoring in primary breast cancer patients. Tumor Biol. 2016;37(10):13769–75. https://doi.org/10.1007/s13277-016-5171-2.
Jueckstock J, Rack B, Friedl TWP, et al. Detection of circulating tumor cells using manually performed immunocytochemistry (MICC) does not correlate with outcome in patients with early breast cancer – results of the German SUCCESS-A- trial. BMC Cancer. 2016;16(1):401. https://doi.org/10.1186/s12885-016-2454-3.
Rack B, Schindlbeck C, Jückstock J, et al. Circulating tumor cells predict survival in early average-to-high risk breast cancer patients. J Natl Cancer Inst. 2014;106(5) https://doi.org/10.1093/jnci/dju066.
Rack B, Schindlbeck C, Jückstock J, et al. Prevalence of CA 27.29 in primary breast cancer patients before the start of systemic treatment. Anticancer Res. 2010;30(5):1837–41.
Sautter-Bihl M-L, Budach W, Dunst J, et al. DEGRO practical guidelines for radiotherapy of breast cancer I. Strahlenther Onkol. 2007;183(12):661–6. https://doi.org/10.1007/s00066-007-1811-1.
Sautter-Bihl M-L, Souchon R, Budach W, et al. DEGRO practical guidelines for radiotherapy of breast cancer II. Strahlenther Onkol. 2008;184(7):347–53. https://doi.org/10.1007/s00066-008-1901-8.
Hudis CA, Barlow WE, Costantino JP, et al. Proposal for standardized definitions for efficacy end points in adjuvant breast cancer trials: the STEEP system. J Clin Oncol. 2007;25(15):2127–32. https://doi.org/10.1200/JCO.2006.10.3523.
Salmen J, Neugebauer J, Fasching PA, et al. Pooled analysis of the prognostic relevance of progesterone receptor status in five German cohort studies. Breast Cancer Res Treat. 2014;148(1):143–51. https://doi.org/10.1007/s10549-014-3130-4.
Schröder L, Rack B, Sommer H, et al. Toxicity assessment of a phase III study evaluating FEC-Doc and FEC-Doc combined with gemcitabine as an adjuvant treatment for high-risk early breast cancer: the SUCCESS-A trial. Geburtshilfe Frauenheilkd. 2016;76(5):542–50. https://doi.org/10.1055/s-0042-106209.
Cámara RJA, Schwentner L, Friedl TWP, et al. Quality of life during and after adjuvant anthracycline-taxane-based chemotherapy with or without gemcitabine in high-risk early breast cancer: results of the SUCCESS A trial. Breast Cancer Res Treat. 2019; https://doi.org/10.1007/s10549-019-05171-6.
Bear HD, Tang G, Rastogi P, et al. Neoadjuvant plus adjuvant bevacizumab in early breast cancer (NSABP B-40 [NRG Oncology]): secondary outcomes of a phase 3, randomised controlled trial. Lancet Oncol. 2015;16(9):1037–48. https://doi.org/10.1016/S1470-2045(15)00041-8.
Bear HD, Tang G, Rastogi P, et al. Bevacizumab added to neoadjuvant chemotherapy for breast cancer. N Engl J Med. 2012;366(4):310–20. https://doi.org/10.1056/NEJMoa1111097.
Earl HM, Vallier A-L, Hiller L, et al. Effects of the addition of gemcitabine, and paclitaxel-first sequencing, in neoadjuvant sequential epirubicin, cyclophosphamide, and paclitaxel for women with high-risk early breast cancer (Neo-tAnGo): an open-label, 2×2 factorial randomised phase 3 trial. Lancet Oncol. 2014;15(2):201–12. https://doi.org/10.1016/S1470-2045(13)70554-0.
Poole CJ, Hiller L, Howard HC, et al. tAnGo: a randomized phase III trial of gemcitabine (gem) in paclitaxel-containing, epirubicin/cyclophosphamide-based, adjuvant chemotherapy (CT) for women with early-stage breast cancer (EBC). J Clin Oncol. 2008;26(15_suppl):506. https://doi.org/10.1200/jco.2008.26.15_suppl.506.
Swain SM, Tang G, Geyer CE, et al. Definitive results of a phase III adjuvant trial comparing three chemotherapy regimens in women with operable, node-positive breast cancer: the NSABP B-38 trial. J Clin Oncol. 2013;31(26):3197–204. https://doi.org/10.1200/JCO.2012.48.1275.
von Minckwitz G, Rezai M, Loibl S, et al. Capecitabine in addition to anthracycline- and taxane-based neoadjuvant treatment in patients with primary breast cancer: phase III GeparQuattro study. J Clin Oncol. 2010;28(12):2015–23. https://doi.org/10.1200/JCO.2009.23.8303.
von Minckwitz G, Rezai M, Fasching PA, et al. Survival after adding capecitabine and trastuzumab to neoadjuvant anthracycline-taxane-based chemotherapy for primary breast cancer (GBG 40—GeparQuattro). Ann Oncol. 2014;25(1):81–9. https://doi.org/10.1093/annonc/mdt410.
Joensuu H, Kellokumpu-Lehtinen P-L, Huovinen R, et al. Adjuvant capecitabine, docetaxel, cyclophosphamide, and epirubicin for early breast cancer: final analysis of the randomized FinXX trial. J Clin Oncol. 2012;30(1):11–8. https://doi.org/10.1200/JCO.2011.35.4639.
Piccart-Gebhart M, Holmes E, Baselga J, et al. Adjuvant lapatinib and trastuzumab for early human epidermal growth factor receptor 2–positive breast cancer: results from the randomized phase III adjuvant lapatinib and/or trastuzumab treatment optimization trial. J Clin Oncol. 2016;34(10):1034–42. https://doi.org/10.1200/JCO.2015.62.1797.
Levine MN, Bramwell VH, Pritchard KI, et al. Randomized trial of intensive cyclophosphamide, epirubicin, and fluorouracil chemotherapy compared with cyclophosphamide, methotrexate, and fluorouracil in premenopausal women with node-positive breast cancer. National Cancer Institute of Canada Clinical. J Clin Oncol. 1998;16(8):2651–8.
Del Mastro L, De Placido S, Bruzzi P, et al. Fluorouracil and dose-dense chemotherapy in adjuvant treatment of patients with early-stage breast cancer: an open-label, 2 × 2 factorial, randomised phase 3 trial. Lancet. 2015;385(9980):1863–72. https://doi.org/10.1016/S0140-6736(14)62048-1.
Sparano JA, Wang M, Martino S, et al. Weekly paclitaxel in the adjuvant treatment of breast cancer. N Engl J Med. 2008;358(16):1663–71. https://doi.org/10.1056/NEJMoa0707056.
Acknowledgements
We are grateful to all patients and would also like to thank all of the staff involved in the study at the participating study sites (SUCCESS-A sites).
Funding
SUCCESS-A was in part supported by grants from Novartis, AstraZeneca, Chugai, Sanofi-Aventis, and Lilly. The study was investigator-initiated and investigator-led and the bodies providing financial support played no part in the study design, data collection, data analysis, data interpretation, or writing of the report. The authors had full access to all of the data and had final responsibility for the decision to submit for publication. Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
BR and WJ designed the study, participated in data acquisition, and drafted the manuscript. LH and TWPF performed the statistical analysis, contributed to the interpretation of the data, and helped to draft the manuscript. PAF, VM, IS, RL, HF, EM, NdG, MD, VF, IB, IA, AS, HT, SM, SYB, JWB, TNF, GH, KL, MWB, and BR contributed to data acquisition and helped to revise the manuscript. PAF helped with data analysis, contributed to data acquisition and interpretation, participated in drafting the manuscript, and revised the manuscript. AdG contributed to data acquisition and interpretation and drafted and revised the manuscript. All authors read and approved the manuscript. AdG and LH as well as BR and WJ contributed equally to this work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The protocol was reviewed and approved by the relevant ethics committees in Germany and conducted in accordance with the Declaration of Helsinki and good clinical practice guidelines. All patients gave written informed consent before entering the study.
Consent for publication
Not applicable.
Competing interests
AdG: honoraria from Novartis, Roche, Pfizer, Daiichi-Sankyo, Tesaro, and Eisai. PF: honoraria and/or grants from Novartis, Amgen, Pfizer, Eisai, Celgene, Myelo Therapeutics, Merk Sharp & Dohme, Macrogenics, Roche, MSD, Daiichi-Sankyo, TEVA, AstraZeneca, Novartis, Puma, Biontech, Daiichi-Sankyo, and Cepheid. VM: speaker honoraria from Amgen, Astra Zeneca, Celgene, Daiichi-Sankyo, Eisai, Pfizer, Novartis, Roche, Teva, and consultancy honoraria from Genomic Health, Hexal, Roche, Pierre Fabre, Amgen, Novartis, MSD, Daiichi-Sankyo, Eisai, Lilly, Tesaro, and Nektar. Institutional research support from Novartis, Roche, Seattle Genetics, and Genentech. HF: honoraria from Novartis, Roche, Celgene, Astellas Pharma, and Merck. TWPF: honoraria from Novartis. NdG: honoraria from Roche, Tesaro, Amgen, PharmaMar, Astrazeneca, and Clovis. AS: honoraria, grants, personal fees, and non-financial support from Roche, Celgene, AbbVie, Molecular Partner, AstraZeneca, Pfizer, Novartis, MSD, Tesaro, and Lilly. HT: honoraria from Novartis and Roche. SM: research support, honoraria, travel expenses from AstraZeneca, Bayer, Boehringer Ingelheim, Clovis, Eisai, GlaxoSmithKline, Jenapharm, Janssen-Cilag, Medac, MSD, PharmaMar, Roche, Sensor Kinesis, Teva, and Tesaro. JUB: honoraria from Roche, Novartis, and Pfizer. SYB: honoraria from Novartis, Roche, and Pfizer. MWB: MWB’s institution conducts research with funding from Novartis and Pfizer. BR: honoraria from AstraZeneca, Chugai, Lilly, Novartis, Sanofi-Aventis, and Jannssen-Cilag. WJ: honoraria from Sanofi-Aventis, Novartis, and Pfizer. All other authors have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix A
Full inclusion and exclusion criteria
Inclusion criteria | |
Patients may be included in the study only if they meet all the following criteria: | |
1 | Primary epithelial invasive carcinoma of the breast pT1–4, pM0 |
2 | Histopathological confirmation of axillary lymph node metastases (pN1–3) or high-risk pN0/NX, defined as: “pT ≥ 2 or histopathological grade 3 or age ≤ 35 or negative hormone receptor status” |
3 | Complete resection of the primary tumor, with resection margins free of invasive carcinoma, no more than 6 weeks previously |
4 | Females ≥ 18 years of age |
5 | Performance status ≤ 2 on the Eastern Cooperative Oncology Group (ECOG) scale |
6 | Adequate bone marrow reserve: leukocytes ≥ 3.0 × 109/L and platelets ≥ 100 × 109/L |
7 | Bilirubin within 1-fold of the reference laboratory’s normal range, ASAT (SGOT), ALAT (SGPT), and AP within 1.5-fold of the reference laboratory’s normal range for patients |
8 | Intention to attend regular follow-up visits for the duration of the study |
9 | Ability to understand the nature of the study and to provide written informed consent |
Exclusion criteria | |
Patients will be excluded from the study for any of the following reasons: | |
10 | Inflammatory breast cancer |
11 | Previous or concomitant cytotoxic or other systemic antineoplastic treatment that is not part of or not allowed in this study |
12 | History of treatment or disease affecting bone metabolism (e.g., Paget’s disease, primary hyperparathyroidism) |
13 | Prior treatment with bisphosphonates within the previous 6 months |
14 | Severe renal insufficiency as evidenced by creatinine clearance (CrCl) < 30 mL/min, as calculated using the Cockcroft–Gault formula: \( \mathrm{CrCl}=\frac{140-\mathrm{age}\left(\mathrm{years}\right)\times \mathrm{weight}\ \left(\mathrm{kg}\right)\times 0.85}{72\times \mathrm{serum}\ \mathrm{creatinine}\ \left(\frac{\mathrm{mg}}{\mathrm{dl}}\right)} \) |
15 | Second primary malignancy (except in situ carcinoma of the cervix or adequately treated basal cell carcinoma of the skin) |
16 | Cardiomyopathy with impaired ventricular function (New York Heart Association > II), cardiac arrhythmias influencing left ventricular ejection fraction and requiring medication, history of myocardial infarction or angina pectoris within the previous 6 months, or arterial hypertension not controlled by medication |
17 | Any known hypersensitivity against docetaxel, epirubicin, cyclophosphamide, fluorouracil, gemcitabine, or any other medication included in the study protocol |
18 | Use of any investigational agent within 3 weeks prior to inclusion |
19 | Patients in pregnancy or breastfeeding (in premenopausal women contraception has to be ensured: intrauterine devices, surgical sterilization methods, or—in hormone-insensitive tumors only—oral, subcutaneous or transvaginal hormonal, non-estrogen-containing contraceptives) |
20 | Current active dental problems, including infection of the teeth or jaw (maxilla or mandible); dental or fixture trauma, or a current or prior diagnosis of osteonecrosis of the jaw (ONJ), of exposed bone in the mouth, or of slow healing after dental procedures |
21 | Recent (within 6 weeks) or planned dental or jaw surgery (e.g., extraction, implants) |
Appendix B
Dose-level adjustments
Treatment could be postponed for up to 2 weeks if the patient had not recovered from hematological and/or nonhematological toxicity. Primary prophylactic application of granulocyte-colony stimulating factor (G-CSF) was not recommended unless one of the following conditions applied: previous febrile neutropenia, prolonged neutropenia for more than 5 days with an absolute neutrophil count (ANC) < 0.5 × 109/L, ANC < 0.1 × 109/L, or prolongation of a chemotherapy cycle due to insufficient leukocytes or neutrophils. Dose reduction was performed in accordance with a prespecified dose level tablea:
Dose level | |||
|---|---|---|---|
0 | − 1 | − 2 | |
Fluorouracil | 500 mg/m2 | 400 mg/m2 | 300 mg/m2 |
Epirubicin | 100 mg/m2 | 80 mg/m2 | 60 mg/m2 |
Cyclophosphamide | 500 mg/m2 | 400 mg/m2 | 300 mg/m2 |
Docetaxel in combination with gemcitabine | 75 mg/m2 | 60 mg/m2 | 45 mg/m2 |
Docetaxel as monotherapy | 100 mg/m2 | 80 mg/m2 | 60 mg/m2 |
Gemcitabine (each arm) | 1000 mg/m2 | 800 mg/m2 | 600 mg/m2 |
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
de Gregorio, A., Häberle, L., Fasching, P.A. et al. Gemcitabine as adjuvant chemotherapy in patients with high-risk early breast cancer—results from the randomized phase III SUCCESS-A trial. Breast Cancer Res 22, 111 (2020). https://doi.org/10.1186/s13058-020-01348-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13058-020-01348-w