
Abstract
Background
Patients in refractory status epilepticus (RSE) may require treatment with continuous intravenous anesthetic drugs (cIVADs) for seizure control. The use of cIVADs, however, was recently associated with poor outcome in status epilepticus (SE), raising the question of whether cIVAD therapy should be delayed for attempts to halt seizures with repeated non-anesthetic antiepileptic drugs. In this study, we aimed to determine the impact of differences in therapeutic approaches on RSE outcome using timing of cIVAD therapy as a surrogate for treatment aggressiveness.
Methods
This was a retrospective cohort study over 14 years (n = 77) comparing patients with RSE treated with cIVADs within and after 48 h after RSE onset, and functional status at last follow-up was the primary outcome (good = return to premorbid baseline or modified Rankin Scale score of less than 3). Secondary outcomes included discharge functional status, in-hospital mortality, RSE termination, induction of burst suppression, use of thiopental, duration of RSE after initiation of cIVADs, duration of mechanical ventilation, and occurrence of super-refractory SE. Analysis was performed on the total cohort and on subgroups defined by RSE severity according to the Status Epilepticus Severity Score (STESS) and by the variables contained therein.
Results
Fifty-three (68.8%) patients received cIVADs within the first 48 h. Early cIVAD treatment was independently associated with good outcome (adjusted risk ratio [aRR] 3.175, 95% confidence interval [CI] 1.273–7.918; P = 0.013) as well as lower chance of both induction of burst suppression (aRR 0.661, 95% CI 0.507–0.861; P = 0.002) and use of thiopental (aRR 0.446, 95% CI 0.205–0.874; P = 0.043). RSE duration after cIVAD initiation was shorter in the early cIVAD cohort (hazard ratio 1.796, 95% CI 1.047–3.081; P = 0.033). Timing of cIVAD use did not impact the remaining secondary outcomes. Subgroup analysis revealed early cIVAD impact on the primary outcome to be driven by patients with STESS of less than 3.
Conclusions
Patients with RSE treated with cIVADs may benefit from early initiation of such therapy.
Similar content being viewed by others


Introduction
There is an ongoing debate on the risks and benefits of the use of continuous intravenous anesthetic drugs (cIVADs) for treatment of refractory status epilepticus (RSE) [1]. As prolonged seizures have been linked to neuronal damage in animal models [2, 3] and to poor functional outcome in humans [4, 5], guidelines advocate cIVADs as third-line therapy for rapid termination of seizures [6]. Both the Neurocritical Care Society and the European Federation of Neurological Societies, however, acknowledge a shortage of data supporting this therapeutic approach [7, 8]. Recent studies reported a negative impact of cIVAD therapy on outcome in RSE [9,10,11]. These studies compared status epilepticus (SE) cohorts treated with and without cIVADs, whereas the factors associated with negative outcome specifically among patients with RSE treated with cIVADs have gained little attention by now. In the present study, we sought to examine the effects of timing of initiation of cIVADs on outcome in RSE by using a 48-h cutoff after RSE onset for definition of early and late use of cIVADs. As cIVADs were reported to be particularly hazardous when used for treatment of milder forms of SE [9], we also analyzed subgroups defined by RSE severity graded by the Status Epilepticus Severity Score (STESS) and the variables included in the STESS [12].
Methods
Patients and data collection
Patients were eligible for inclusion into the study if they received treatment for RSE on the neurological intensive care unit of our institution between January 2001 and January 2015 with continuous intravenous infusion of at least one of the following drugs (cIVADs): midazolam, propofol, thiopental, and ketamine. We used our electronic medical records and electroencephalography databases to gather information on demographics, RSE etiology, severity and duration, treatment, complications, and outcome. Demographics included gender, age at admission, and premorbid functional status. Data were assessed by two independent reviewers using a standardized data extraction form (DM and RUK). In case of disagreement, data were analyzed by a third reviewer (HBH) and consensus was found through discussion. For reasons of comparability with previous research, RSE caused by hypoxic encephalopathy was excluded. Only incidence episodes were considered; that is, in case of recurrent treatment with anesthetics for RSE in our institution during the study period, only the first episode was entered into the study [9].
Refractory status epilepticus: definition, duration, and severity
In accordance with previous studies, SE was defined as clinically or electroencephalographically persisting seizure with duration of at least 5 min or as a series of seizures without interictal recovery [8]. The worst seizure semiology prior to initiation of antiepileptic therapy was used to categorize episodes as simple partial SE (SPSE), complex partial SE (CPSE), generalized convulsive SE (GCSE), or non-convulsive SE (NCSE) in coma [10]. RSE was defined as SE with ongoing seizure activity despite application of two adequately dosed antiepileptic drugs (AEDs) [13]. RSE duration after initiation of cIVAD therapy was defined as time between the beginning of cIVAD treatment and clear and enduring electroencephalographic or clinical seizure cessation or both. Durations of RSE after initiation of cIVADs as well as times on mechanical ventilation were estimated in days. Any portion of one day in RSE or on the respirator, respectively, was counted as one full day. RSE severity was graded with the STESS and was dichotomized into STESS of less than 3 (mild) and STESS of at least 3 (severe) as previously proposed [12]. RSE etiology was categorized in accordance with the guidelines of the International League Against Epilepsy into acute symptomatic, remote symptomatic, progressive symptomatic, and unknown etiology [14]. A potentially fatal etiology was defined when meeting the criteria introduced by Rossetti et al. [15].
Definition of early and late cIVAD therapy
Treatment with cIVADs was defined as early when started within 48 h after RSE onset; otherwise, it was defined as late.
Outcome measures and outcome definitions
The primary outcome of this study was functional status at last available follow-up graded by the modified Rankin Scale (mRS) [16]. Information on outcome was extracted from discharge summaries of rehabilitation facilities or own records if patients had represented to our hospital. Outcome was defined as good in case of complete recovery after RSE (that is, when the mRS at last available follow-up equaled the premorbid mRS) or, in case of new disability, when the mRS at last available follow-up was less than 3. Otherwise, outcome was defined as poor. Secondary outcomes were functional outcome at discharge (with good and poor defined identically as for the primary outcome), in-hospital mortality, RSE termination, induction of burst suppression, use of thiopental, duration of RSE after initiation of cIVADs, duration of mechanical ventilation, and occurrence of super-refractory SE (SRSE).
Statistical analysis
Statistical analyses were performed by using SPSS Statistics 21.0 (http://www.spss.com). P values of less than 0.05 were considered statistically significant, and all tests used were two-sided. Baseline clinical data and RSE characteristics were compared by using Pearson chi-squared test or, where appropriate, Fisher’s exact tests for categorical data and Mann–Whitney U test for continuous variables. Crude and adjusted risk ratios for primary and secondary outcomes were estimated by Poisson regression with robust error variance. Multivariable analysis adjusted for STESS (as continuous variable) and a potentially fatal etiology. These calculations were performed on the overall cohort as well as subgroups defined by the STESS (cutoff 3 points) and the variables included in it (that is, age, a history of seizures, level of consciousness, and worst seizure type). Time-to-event outcomes were compared with the Kaplan–Meier method with hazard ratios estimated by using Cox proportional hazard analysis. Patients in whom RSE could not be terminated prior to discharge or death were censored from this analysis.
Results
Study population
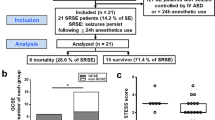
We identified 159 RSE episodes in 131 patients. In 83 (52.2%) episodes, patients received treatment with cIVADs. After exclusion of recurrent episodes (n = 6), 77 patients remained for final analysis. Of those, 53 (68.8%) received cIVAD therapy within the first 48 h of RSE (Fig. 1). A description of the study cohort is presented in Table 1. Patients were treated with up to four cIVADs, but the majority received a maximum of two cIVADs (n = 59, 76.6%). The cIVAD most frequently used first was propofol (n = 47, 61.0%; Additional file 1: Table S1). In-hospital mortality was 24.7%, and RSE termination rate was 85.7%. Follow-up data were available for all but two patients (97.4%); one patient was lost to follow-up in the early and one in the late cIVAD cohort. The median follow-up time was 11 weeks (interquartile range [IQR] 6–25).

Flowchart of study cohort. In total, 569 episodes were treated for status epilepticus (SE) in our institution between January 2001 and January 2015. Among those, 159 satisfied the criteria of refractory SE. In 83 episodes, patients received treatment with continuous intravenous anesthetic drugs (cIVADs). Seven recurrent episodes were excluded, leaving 77 patients for final analysis, of whom 53 received early cIVADs and 24 received late cIVADs. Primary and secondary study outcomes are depicted. Abbreviations: cIVAD continuous intravenous anesthetic drug, RSE refractory status epilepticus, SE status epilepticus, SRSE super-refractory status epilepticus
Factors associated with cIVAD timing
Age, SE severity, and SE etiology did not differ significantly between episodes treated with and without early cIVADs (Table 1). In the early cIVAD group, impaired consciousness on admission and GCSE were more frequent while CPSE was rarer. A comparable number of patients had NCSE in coma. No patient had SPSE.
Primary and secondary outcomes
The results of the analysis are summarized in Table 2. After adjustment for confounders, early use of cIVADs was an independent predictor of good outcome at last follow-up. The follow-up time did not differ significantly between the early and late cIVAD cohort (12 [IQR 6–26] versus 9 [IQR 5–18] weeks; P = 0.483).
In regard to secondary outcomes, early use of cIVADs was significantly associated with lower chance of both use of thiopental and induction of burst suppression but did not independently predict functional outcome at discharge, chance of RSE termination, risk of SRSE development, and in-hospital mortality. RSE duration after initiation of therapy was shorter in early cIVAD patients, whereas duration of mechanical ventilation did not differ significantly between cohorts (Fig. 2).

Kaplan–Meier curves for a duration of mechanical ventilation and b duration of status epilepticus after initiation of continuous intravenous anesthetic drugs. Censored cases are depicted by plus (+) marks along the curves. Abbreviations: CI confidence interval, cIVAD continuous intravenous anesthetic drug, HR hazard ratio, RSE refractory status epilepticus
Subgroup analysis for primary outcome
The results of the subgroup analysis for the primary outcome are depicted in Fig. 3. Early use of cIVADs was independently associated with good outcome at last follow-up in patients with STESS less than 3, age less than 65 years, and a history of seizures but not in patients with STESS of at least 3, age of at least 65 years, and no previous seizures. Level of consciousness and worst seizure type did not influence impact of timing of cIVAD therapy on functional outcome. Because among patients with NCSE in coma one outcome had zero observations, calculation of adjusted risk ratios was not possible for this subgroup. The follow-up times did not differ significantly between patients who received cIVADs early compared with those who received treatment late in any of the subgroups (Additional file 2: Table S2).

Poisson regression was used to compare the influence of early continuous intravenous anesthetic drug (cIVAD) therapy in subgroups defined by overall STESS as well as variables included in the STESS. *Risk ratios (RRs) were adjusted for STESS (as a continuous variable) and a potentially fatal etiology. In the subgroups of patients with non-convulsive status epilepticus (NCSE) in coma, one outcome had zero observations and therefore adjusted RRs could not be calculated. Abbreviations: CI confidence interval, cIVAD continuous intravenous anesthetic drug, CPSE complex partial status epilepticus, GCSE generalized convulsive status epilepticus, STESS Status Epilepticus Severity Score
Discussion
In this study, we aimed to analyze the impact of timing of anesthetic therapy on the clinical course and the prognosis of RSE and found early initiation of cIVADs to be associated with higher chance of good outcome at last follow-up. This is one of only a few studies exclusively focusing on RSE episodes treated with continuous anesthetics, and several aspects of our results deserve attention.
First, we found reduced mental status and GCSE to be more frequent among patients who received treatment with cIVADs early. This probably reflects the fact that time of initiation of such therapy may be driven by clinical necessity rather than a specific treatment strategy in many cases, including those when patients have persisting convulsions after administration of two lines of non-anesthetic AEDs or require intubation for airway protection [17]. Both severely lowered levels of consciousness and generalized convulsive seizures are known predictors of negative outcome in SE [15, 18, 19]. Thus, although unfavorable prognosticators were more common among patients with early initiation of cIVADs, these individuals had better outcome. As there were no differences in baseline characteristics accounting for this fact, it appears plausible that this observation is related to the time of cIVAD initiation, especially because this factor was an independent predictor of outcome upon multivariable analysis.
Second, the choice of anesthetics administered requires discussion. Early cIVAD therapy was a negative predictor for the use of thiopental. Previous research found that, compared with other anesthetics, thiopental for RSE was associated with higher risk of complications, prolonged mechanical ventilation [20], duration of intensive care unit and overall hospital stay, and worse short- and long-term outcome [21]. Therefore, both clinical course and outcome could depend more on the choice of a specific anesthetic agent than on the time of initiation of cIVAD therapy. However, the decision to apply barbiturates may be influenced by a higher degree of seizure refractoriness suspected, especially as previous research found their use for RSE to be a surrogate for treatment aggressiveness [22]. Refractoriness to therapy in SE is known to increase with the duration of seizures [23] and therefore late use of anesthetics could lead to administration of a more hazardous agent, thus linking late use of cIVADs to poorer outcome.
Third, stratification of the study population according to the STESS and its components revealed that the positive effect of early cIVAD initiation in the overall cohort appeared driven primarily by the subgroups of individuals with STESS less than 3, age less than 65 years, and a history of seizures. A potential association between low RSE severity and good outcome following early cIVAD use deserves particular attention, given that previous reports advocated reserving aggressive therapy for patients scoring high on the STESS because of the risk-benefit ratio [12]. Our findings, however, support the opposite approach as rapid treatment escalation was related to positive outcome specifically among patients with RSE of low severity as indicated by a STESS less than 3. This finding is intriguing, but our results along with observations from previous studies offer a plausible explanation for it: (1) RSE duration was significantly shorter in the early cIVAD cohort in our study, (2) previous research found shorter RSE duration to be an independent predictor of positive outcome among RSE patients receiving cIVADs [24], and (3) low STESS frequently implies a more benign RSE etiology and therefore a larger impact of seizure duration on outcome [5].
To our knowledge, there are no studies that specifically aimed to examine the impact of cIVAD timing on outcome in RSE. In recent research on the effects of high versus low continuous intravenous midazolam (cIV-MDZ) infusion doses on RSE course and outcome, treatment was started significantly earlier in the high-dose cohort and these patients were less likely to die during hospital stay or to have withdrawal seizures; however, in a multivariable model, time of cIV-MDZ treatment was not an independent outcome predictor [25].
A secondary analysis of the Rapid Anticonvulsant Medication Prior to Arrival Trial (RAMPART) characterized the influence of early (defined as performed pre-hospital or within 30 min of emergency department arrival) versus late endotracheal intubation on outcome in SE and observed late intubation to be associated with higher mortality [26]. This finding points in the same direction as our observations, but, given major differences in inclusion criteria and in the definition of early, it is difficult to compare study results.
Limitations
Our study has several clear limitations that need to be considered. The sample size is small, which is particularly problematic in a disorder as heterogenic as RSE. Data were collected retrospectively, and the medical records did not contain detailed enough information to determine the exact time of RSE cessation after initiation of cIVADs in all cases; therefore, we had to estimate RSE duration in days and not in hours. Furthermore, we could (with certainty) only tell that but not clearly assess the reasons why cIVADs were applied early or late. Some patients may have received cIVADs because they required intubation for airway protection or mechanical ventilation and not primarily for seizure control. Therefore, confounders not considered in our study may have substantially influenced therapeutic decisions and outcome, introducing the risk of bias into our results. Furthermore, we did not assess cIVAD dosing, and treatment of RSE with cIVADs did not follow a specific protocol in our institution during the early years of the study period. Setting the cutoff between early and late cIVAD treatment at 48 h after RSE onset represents an arbitrary definition which may appear inappropriate in light of guidelines advocating rapid treatment escalation. However, in our experience, a conservative approach in the first 48 h may represent a viable therapeutic option in non-convulsive RSE episodes, including those arising from GCSE either spontaneously or after initial treatment. The primary outcome measure of this study was not based on data collected at defined time points but relied on last available follow-up findings. Although follow-up durations were variable, they did not differ significantly between any of the cohorts compared. Furthermore, the validity of the primary outcome measure is supported by a trend toward higher chance of better outcome in the early cIVAD cohort already at time of discharge.
Conclusions
Our findings indicate that when cIVADs are applied in RSE, prescribing them early may positively impact outcome, probably by shorter seizure duration and apparently mainly in those patients who do not have a severe RSE etiology dominating their prognosis. However, whether patients with RSE generally benefit from an aggressive or a conservative therapeutic approach cannot be answered by this study and this is because we exclusively focused on individuals treated with cIVADs.
Abbreviations
- AED:
-
Antiepileptic drug
- CI:
-
Confidence interval
- cIVAD:
-
Continuous intravenous anesthetic drug
- cIV-MDZ:
-
Continuous intravenous midazolam
- CPSE:
-
Complex partial status epilepticus
- GCSE:
-
Generalized convulsive status epilepticus
- HR:
-
Hazard ratio
- IQR:
-
Interquartile range
- mRS:
-
Modified Rankin Scale
- NCSE:
-
Non-convulsive status epilepticus
- RR:
-
Risk ratio
- RSE:
-
Refractory status epilepticus
- SE:
-
Status epilepticus
- SPSE:
-
Simple partial status epilepticus
- SRSE:
-
Super-refractory status epilepticus
- STESS:
-
Status Epilepticus Severity Score
References
Hirsch LJ. Finding the Lesser of Two Evils: Treating Refractory Status Epilepticus. Epilepsy Curr. 2015;15:313–6.
Meldrum BS, Brierley JB. Neuronal loss and gliosis in the hippocampus following repetitive epileptic seizures induced in adolescent baboons by allylglycine. Brain Res. 1972;48:361–5.
Guo D, Arnspiger S, Rensing NR, Wong M. Brief seizures cause dendritic injury. Neurobiol Dis. 2012;45:348–55.
Claassen J, Hirsch LJ, Emerson RG, Mayer SA. Treatment of refractory status epilepticus with pentobarbital, propofol, or midazolam: a systematic review. Epilepsia. 2002;43:146–53.
Sutter R, Marsch S, Fuhr P, Ruegg S. Mortality and recovery from refractory status epilepticus in the intensive care unit: a 7-year observational study. Epilepsia. 2013;54:502–11.
Sutter R, Kaplan PW. Can anesthetic treatment worsen outcome in status epilepticus? Epilepsy Behav. 2015;49:294–7.
Meierkord H, Boon P, Engelsen B, Gocke K, Shorvon S, Tinuper P, et al. EFNS guideline on the management of status epilepticus in adults. Eur J Neurol. 2010;17:348–55.
Brophy GM, Bell R, Claassen J, Alldredge B, Bleck TP, Glauser T, et al. Guidelines for the evaluation and management of status epilepticus. Neurocrit Care. 2012;17:3–23.
Marchi NA, Novy J, Faouzi M, Stahli C, Burnand B, Rossetti AO. Status Epilepticus: Impact of Therapeutic Coma on Outcome. Crit Care Med. 2015;43:1003–9.
Sutter R, Marsch S, Fuhr P, Kaplan PW, Ruegg S. Anesthetic drugs in status epilepticus: risk or rescue? A 6-year cohort study. Neurology. 2014;82:656–64.
Kowalski RG, Ziai WC, Rees RN, Werner JK, Jr., Kim G, Goodwin H, et al. Third-line antiepileptic therapy and outcome in status epilepticus: the impact of vasopressor use and prolonged mechanical ventilation. Crit Care Med. 2012;40:2677–84.
Rossetti AO, Logroscino G, Milligan TA, Michaelides C, Ruffieux C, Bromfield EB. Status Epilepticus Severity Score (STESS): a tool to orient early treatment strategy. J Neurol. 2008;255:1561–6.
Jagoda A, Riggio S. Refractory status epilepticus in adults. Ann Emerg Med. 1993;22:1337–48.
Guidelines for epidemiologic studies on epilepsy. Commission on Epidemiology and Prognosis, International League Against Epilepsy. Epilepsia. 1993;34:592–6.
Rossetti AO, Hurwitz S, Logroscino G, Bromfield EB. Prognosis of status epilepticus: role of aetiology, age, and consciousness impairment at presentation. J Neurol Neurosurg Psychiatry. 2006;77:611–5.
Rankin J. Cerebral vascular accidents in patients over the age of 60. II. Prognosis. Scott Med J. 1957;2:200–15.
Sutter R, De Marchis GM, Semmlack S, Fuhr P, Ruegg S, Marsch S, et al. Anesthetics and Outcome in Status Epilepticus: A Matched Two-Center Cohort Study. CNS drugs 2017;31:65–74.
Sutter R, Kaplan PW, Ruegg S. Outcome predictors for status epilepticus--what really counts. Nat Rev Neurol. 2013;9:525–34.
Treiman DM, Meyers PD, Walton NY, Collins JF, Colling C, Rowan AJ, et al. A comparison of four treatments for generalized convulsive status epilepticus. Veterans Affairs Status Epilepticus Cooperative Study Group. N Engl J Med. 1998339:792–798.
Rossetti AO, Milligan TA, Vulliemoz S, Michaelides C, Bertschi M, Lee JW. A randomized trial for the treatment of refractory status epilepticus. Neurocrit Care. 2011;14:4–10.
Bellante F, Legros B, Depondt C, Creteur J, Taccone FS, Gaspard N. Midazolam and thiopental for the treatment of refractory status epilepticus: a retrospective comparison of efficacy and safety. J Neurol. 2016;263:799–806.
Rossetti AO, Logroscino G, Bromfield EB. Refractory status epilepticus: effect of treatment aggressiveness on prognosis. Arch Neurol. 2005;62:1698–702.
Betjemann JP, Lowenstein DH. Status epilepticus in adults. Lancet Neurol. 2015;14:615–24.
Santamarina E, Gonzalez-Cuevas GM, Sanchez A, Gracia RM, Porta I, Toledo M, et al. Prognosis of status epilepticus in patients requiring intravenous anesthetic drugs (a single center experience). Seizure 2017;45:74–79.
Fernandez A, Lantigua H, Lesch C, Shao B, Foreman B, Schmidt JM, et al. High-dose midazolam infusion for refractory status epilepticus. Neurology 2014;82:359–365.
Vohra TT, Miller JB, Nicholas KS, Varelas PN, Harsh DM, Durkalski V, et al. Endotracheal Intubation in Patients Treated for Prehospital Status Epilepticus. Neurocrit Care 2015;23:33–43.
Acknowledgments
We thank Anna Geyer for valuable support in data acquisition.
Funding
This work was not funded.
Availability of data and materials
The datasets on which the conclusions of our manuscript rely are stored in our institutional database. Anonymized data will be shared by request from a qualified investigator.
Author information
Authors and Affiliations
Contributions
DM contributed to study concept and design, acquisition of the data, statistical analysis, interpretation of the data, drafting of the manuscript, and study supervision. HBH contributed to study concept and design, acquisition of the data, interpretation of the data, critical revision of the manuscript for important intellectual content, and study supervision. RUK contributed to acquisition of the data, interpretation of the data, and critical revision of the manuscript for important intellectual content. CR, AGJ, TB, MIS, and HMH contributed to interpretation of the data and critical revision of the manuscript for important intellectual content. All authors have read the manuscript, agreed with the contents, and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the local ethics committee of the Friedrich-Alexander University Erlangen-Nürnberg (FAU), Germany (vote number: 48_15Bc). Given the retrospective nature of the study, the need for informed consent was waived.
Consent for publication
Not applicable.
Competing interests
HBH and DM received unrestricted grants from UCB Pharma. HMH received grants from the EU and served on the scientific advisory boards of Cerbomed, Desitin, Eisai, Bial, and UCB Pharma. He received personal fees from IQWiG. He served on the speakers’ bureau of or received unrestricted grants from Desitin, Eisai, Novartis, Bial, Hexal, Boehringer Ingelheim, and UCB Pharma. CR, AGJ, TB, MIS, and RUK declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
Table S1. Overview of continuous intravenous anesthetic drugs applied. (DOCX 14 kb)
Additional file 2:
Table S2. Comparison of follow-up times between patients with early versus late continuous intravenous anesthetic drug (cIVAD) treatment in the subgroups defined by Status Epilepticus Severity Score (STESS) and its components. (DOCX 14 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Madžar, D., Reindl, C., Giede-Jeppe, A. et al. Impact of timing of continuous intravenous anesthetic drug treatment on outcome in refractory status epilepticus. Crit Care 22, 317 (2018). https://doi.org/10.1186/s13054-018-2235-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-018-2235-2