
Abstract
Background
The Utstein style for drowning (USFD) was published in 2003 with the aim of improving drowning research. To support a revision of the USFD, the current study aimed to generate an inventory of the use of the USFD parameters and compare the findings of the publications that have used the USFD.
Methods
A search in Pubmed, Embase, the Cochrane Library, Web of Science and Scopus was performed to identify studies that used the USFD and were published between 01-10-2003 and 22-03-2015. We also searched in Pubmed, Embase, the Cochrane Library, Web of Science, and Scopus for all publications that cited the two publications containing the original ILCOR advisory statement introducing and recommending the USFD. In total we identified 14 publications by groups that explicitly used elements of the USFD for collecting and reporting their data.
Results
Of the 22 core and 19 supplemental USFD parameters, 6–19 core (27–86%) and 1–12 (5–63%) supplemental parameters were used; two parameters (5%) have not been used in any publication. Associations with outcome were reported for nine core (41%) and five supplemental (26%) USFD parameters. The USFD publications also identified non-USFD parameters related to outcome: initial cardiac rhythm, time points and intervals during resuscitation, intubation at the drowning scene, first hospital core temperature, serum glucose and potassium, the use of inotropic/vasoactive agents and the Paediatric Index of Mortality 2-score.
Conclusions
Fourteen USFD based drowning publications have been identified. These publications provide valuable information about the process and quality of drowning resuscitation and confirm that the USFD is helpful for a structured comparison of the outcome of drowning resuscitation.
Similar content being viewed by others

Background
In 2003, a consensus-based ILCOR advisory statement recommended the Utstein style for drowning (USFD) for use in planning of, and reporting of the results of drowning studies to improve the quality and comparability of drowning studies [1, 2]. Since 2003 the USFD has been used to study drowning, which is a leading cause of accidental death worldwide, with an estimated death toll of 372.000 persons per year [3,4,5,6,7,8,9,10,11,12,13,14,15,16,17]. The USFD template consists of 22 core parameters that the statement recommended should be included in all drowning studies, and 19 supplemental parameters that are considered to be less important or are difficult to collect (Table 1).
The aim of this study was to generate an inventory of USFD usage during the more than 10 years since it was published, and to review and compare the findings of the publications that have used the USFD. This study elaborates on an initial study that was performed to support the revision process that generated the revised USFD, published in 2017 [18, 19]. Both the revised USFD and this current study will contribute to improvements in the uniformity of data collection and reporting, as recommended by the WHO in their recent document “Global Report on Drowning: preventing a leading killer” [17].
Methods
A literature search was performed to identify peer-reviewed publications, concerning drowning that had used the USFD [1, 2] and were published between 01-10-2003 (month of the publication of the USFD) and 22-03-2015 (the latter date was arbitrarily chosen and was shortly before the revision process of the USFD was completed).
Pubmed search terms were: "Drowning"[Mesh] OR drown*[tw]) AND utstein[tw]; Embase search terms were: 'drowning'/exp. OR drown*:ab,ti AND utstein:ab,ti; Cochrane Library and Web of Science search terms were: drown* AND utstein; the Scopus search term used was “drowning AND Utstein”.
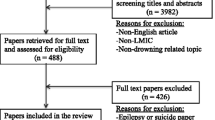
The search provided 15 publications from Pubmed, 22 from Embase, none from the Cochrane Library, 28 from Web of Science and 17 from Scopus. Altogether, the systematic literature search identified 37 different publications (Fig. 1). These publications were independently reviewed by two authors (AV and AA), to identify those that explicitly stated an a priori intention to base their study on the USFD. After exclusion of drowning publications that did not explicitly mention that data collection was based on the USFD parameters, eight USFD based drowning publications remained [3,4,5,6,7,8,9,10]. Of the 29 publications that had not used the USFD, three were drowning publications of which data collection was based on the Utstein style for out of hospital cardiac arrest [20, 21], or did not describe the use of any Utstein template [22], four were publications on resuscitation that included only a few drowning patients [23,24,25,26], one was a resuscitation publication that excluded drowning victims [27], five were reviews [28,29,30,31,32], and 16 were other types of publications (definition of drowning, editorials, abstracts, letter to the editor, non-English language articles, post mortem examinations, book chapter) [33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48].

Flowchart of search strategy
To enhance the robustness of the search, we additionally searched in Pubmed, Embase, the Cochrane Library, the Web of Science and Scopus for all publications that cited the two publications containing the original ILCOR advisory statement introducing and recommending the USFD [1, 2]. This revealed a total of six further publications that matched the inclusion criteria for our study, but had not been identified by the initial search strategy [11,12,13,14,15,16].
A total of 14 publications were thus included in the current analysis [3,4,5,6,7,8,9,10,11,12,13,14,15,16]. The individual publications were subsequently analysed independently by two reviewers (AV, AA) to identify the USFD parameters used by each publication, the information these USFD parameters provided, and USFD as well as non-USFD parameters related to outcome. In case of disagreement, discussion continued until agreement was reached.
We decided a priori to report all parameters for which an association with outcome was published, regardless of the number of publications in which they were used and to limit the reporting of non-outcome related parameters to those parameters that had been reported in five or more publications. Because the objective of our study was to report the use of the USFD, it was also decided a priori not to combine the data of the publications for a meta-analysis or to perform any statistical analysis of the patient data [49].
Results
Table 2 summarises the 14 USFD drowning publications, in which 27–86% of the core and 5–63% of the supplemental USFD parameters were used.
Table 3 describes the nine core (41%) and five supplemental (26%) USFD parameters related to outcome. Table 4 describes the 11 core (50%) and six supplemental (32%) USFD parameters not related to outcome that were reported in 5 or more of the publications. In total, 10 USFD parameters not related to outcome were reported in less than 5 of the 14 drowning publications: Race or Ethnic category (n = 2), Residence (n = 4), Time of removal of victim from water (n = 3), Cyanosis (n = 4), Time of first emergency medical services (EMS) assessment (n = 4), Oxygen haemoglobin saturation (n = 3), Toxicology testing (n = 0), Date of hospital discharge (n = 1), Quality of life (n = 0), Other injuries and morbidities (n = 3).
The USFD publications also included non-USFD parameters. The non-USFD parameters related to outcome are described below.
In one publication the first hospital core temperature of victims treated with extracorporeal life support (ECLS), 24 h survivors had a lower temperature than non-survivors (p = 0.004) [16].
Ten publications report the initial cardiac rhythm (at EMS arrival, at the emergency department (ED) and/or during hospital admission). With the exception of two studies [14, 16], the other studies showed that a shockable rhythm is rare (0–9%) in drowning victims in need of resuscitation [3,4,5, 7,8,9,10, 12]. Three of the latter publications showed a relation between the initial cardiac rhythm and outcome [3, 9, 10].
Eleven publications included parameters that were related to the start or duration of basic life support (BLS), advanced life support (ALS), or interventions by EMS, either as time intervals or as time points [3,4,5, 7,8,9,10,11,12, 14, 16]. An early start of resuscitation, rapid transfer to hospital and shorter duration of resuscitation were significantly related to better outcome [4, 5, 7, 10].
In one publication, intubation at the drowning scene was significantly related to bad outcome [9].
One publication concluded that glucose levels were significantly lower in survivors [8]. The relationship between serum potassium and outcome was inconsistent [3, 4, 8, 16].
The use of inotropes/vasoactive medications was related to outcome in three publications [4, 9, 10]. One of these publications concluded that more drowning victims that survived received vasopressin than non-survivors (64% versus 22%;p = 0.03) [4]. The use of inotropic/vasoactive agents was associated with worse outcome in two publications (p < 0.001 and p = 0.01) [9, 10].
The Paediatric Index of Mortality 2-score for patients admitted to the intensive care unit (ICU) has been calculated in one publication and was significantly higher in non-survivors [9].
In 4 of the 14 identified publications the authors commented on the USFD and/or suggested alterations to the USFD. One publication, involving a study in which identification of non-USFD outcome related parameters was a secondary study goal, recommended inclusion of information on early BLS, serum potassium, rewarming speed after the use of cardiopulmonary bypass and the initial cardiac rhythm in the USFD [3]. Another publication, involving a study in which the feasibility of the USFD parameters was tested as a secondary study goal, suggested changing some parameters on victim and scene information, including rescue related parameters and rescue related injuries [6]. In this same publication the authors also suggested use of ‘country of birth’ instead of the USFD parameter ‘race or ethnic category’ [6]. One publication suggested reporting ‘time of submersion’ as core parameter. Furthermore this same publication concluded that the USFD is applicable for reporting retrospective data of drowned children [8]. One publication promoted the USFD and suggested the creation of an international registry [16].
Discussion
Between 1-10-2003 and 22-3-2015, the USFD has been used in 14 USFD based drowning publications, which involved different populations, focus and methodology. The cumulative findings of the reports have identified 14 USFD parameters for whom associations with outcome were reported. Also non-USFD parameters related to outcome have been identified: initial cardiac rhythm, time points and intervals during resuscitation, intubation at the drowning scene, first hospital core temperature, serum glucose and potassium, the use of inotropic/vasoactive agents and the Paediatric Index of Mortality 2-score.
None of the 14 USFD based drowning publications included in this review used all USFD parameters. This is explained in part by the narrow focus of some of the publications, for example on the pre-hospital setting [6], and the differences in methodology of the publications. Furthermore, the results show that several parameters such as the age of the drowning victims were described inconsistently (mean, median or range). These inconsistencies are probably the result of both the preferences in data reporting by the individual researchers, as well as the fact that the USFD does not provide extensive advice on this matter. Such inconsistencies hinder the goal of this template that is designed to improve the quality and comparability of individual studies, in order to identify ways in which outcome can be improved. Despite these issues, the use of the USFD parameters has enabled a comparison of resuscitation outcome data from these different drowning publications during the review process.
Several researchers have included in their research additional parameters potentially related to drowning outcome and some have recommended the inclusion of these additional parameters in drowning research.
This review of 14 USFD based studies was initiated at the start of the USFD revision process. Preliminary data were included in the consensus discussions that resulted in the revised USFD publications [18, 19]. The results we report here, support the decision that was made to revise the USFD [18, 19]. It is hoped that the revised USFD and this review will assist researchers in studying drowning and will encourage them to use the USFD parameters in their research. This might lead to a more complete use of the USFD and thereby improved comparability of drowning studies in the future. The results we report here will hopefully also help to inform future revisions to the USFD.
There are some limitations regarding the review process that should be mentioned. For the purpose of this review we have only focused on USFD based drowning publications. It is possible that other publications on drowning in the same time period might have demonstrated different results. By using the search terms and databases mentioned in the Methods section, the potential for missing relevant publications is minimized, but cannot be ruled out entirely.
The results of the reviewed publications displayed a variety of important information on the outcome and circumstances of drowning resuscitation. However, the authors realise that the USFD is only a tool to facilitate drowning resuscitation research. A recent publication concluded that the methodology of future drowning studies also needs to be based on unbiased high quality data and multi-variate analysis [49].
Conclusions
Between 2003 and 2015, 14 USFD based publications on drowning have been published. These publications have identified associations between several USFD as well as non-USFD parameters and outcome. None of the publications reported all USFD parameters and there were inconsistencies in the way the USFD parameters were reported. This negatively influenced a structured comparison of the USFD parameters between the studies. However, despite the difficulties these publications still show that the use of the USFD is helpful for a structured comparison of the outcome of drowning resuscitation and provides valuable information about the process and quality of drowning resuscitation.
The analysis also points at some limitations of the USFD and has identified important additional parameters that have been considered for a revised USFD.
Abbreviations
- ALS:
-
Advanced life support
- BLS:
-
Basic life support
- ECLS:
-
Extracorporeal life support
- ED:
-
Emergency department
- EMS:
-
Emergency medical services
- ICU:
-
Intensive care unit
- USFD:
-
Utstein style for drowning
- WHO:
-
World Health Organization
References
Idris AH, Berg RA, Bierens J, Bossaert L, Branche CM, Gabrielli A, Graves SA, Handley AJ, Hoelle R, Morley PT, Papa L, Pepe PE, Quan L, Szpilman D, Wigginton JG, Modell JH, American Heart Association. Recommended guidelines for uniform reporting of data from drowning: the “Utstein style”. Circulation. 2003;108:2565–74.
Idris AH, Berg RA, Bierens J, Bossaert L, Branche CM, Gabrielli A, Graves SA, Handley AJ, Hoelle R, Morley PT, Papa L, Pepe PE, Quan L, Szpilman D, Wigginton JG, Modell JH, American Heart Association, Maatschappij tot Redding van Drenkelingen, European Resuscitation Council, US Centers for Disease Control and Prevention, University of Florida, University of North Carolina, Australia and New Zealand Resuscitation Council, InterAmerican Heart Foundation, Heart and Stroke Foundation of Canada, Resuscitation Council of Southern Africa. Recommended guidelines for uniform reporting of data from drowning: the “Utstein style”. Resuscitation. 2003;59:45–57.
Eich C, Brauer A, Timmermann A, Schwarz SK, Russo SG, Neubert K, Graf BM, Aleksic I. Outcome of 12 drowned children with attempted resuscitation on cardiopulmonary bypass: an analysis of variables based on the “Utstein Style for Drowning”. Resuscitation. 2007;75:42–52.
Grmec S, Strnad M, Podgorsek D. Comparison of the characteristics and outcome among patients suffering from out-of-hospital primary cardiac arrest and drowning victims in cardiac arrest. Int J Emerg Med. 2009;2:7–12.
Youn CS, Choi SP, Yim HW, Park KN. Out-of-hospital cardiac arrest due to drowning: an Utstein Style report of 10 years of experience from St. Mary’s Hospital. Resuscitation. 2009;80:778–83.
Venema AM, Groothoff JW, Bierens JJ. The role of bystanders during rescue and resuscitation of drowning victims. Resuscitation. 2010;81:434–9.
Choi SP, Youn CS, Park KN, Wee JH, Park JH, Oh SH, Kim SH, Kim JY. Therapeutic hypothermia in adult cardiac arrest because of drowning. Acta Anaesthesiol Scand. 2012;56:116–23.
Vahatalo R, Lunetta P, Olkkola KT, Suominen PK. Drowning in children: Utstein style reporting and outcome. Acta Anaesthesiol Scand. 2014;58:604–10.
Joanknecht L, Argent AC, van Dijk M, van As AB. Childhood drowning in South Africa: local data should inform prevention strategies. Pediatr Surg Int. 2015;31:123–30.
Kieboom JK, Verkade HJ, Burgerhof JG, Bierens JJ, Rheenen PF, Kneyber MC, Albers MJ. Outcome after resuscitation beyond 30 minutes in drowned children with cardiac arrest and hypothermia: Dutch nationwide retrospective cohort study. BMJ. 2015;350:h418.
Hunsucker JL, Davison SJ. Analysis of rescue and drowning history from a lifeguarded waterpark environment. Int J Inj Control Saf Promot. 2011;18:277–84.
Allan PF, Fang R, Martin KD, Glenn M, Conger NG. Combat-associated drowning. J Trauma. 2010;69(Suppl 1):S179–87.
Ma WJ, Nie SP, Xu HF, Xu YJ, Song XL, Guo QZ, Zhang YR. An analysis of risk factors of non-fatal drowning among children in rural areas of Guangdong Province, China: a case-control study. BMC Public Health. 2010;10:156. https://doi.org/10.1186/1471-2458-10-156.
Wanscher M, Agersnap L, Ravn J, Yndgaard S, Nielsen JF, Danielsen ER, Hassager C, Romner B, Thomsen C, Barnung S, Lorentzen AG, Hogenhaven H, Davis M, Moller JE. Outcome of accidental hypothermia with or without circulatory arrest experience from the Danish Praesto Fjord boating accident. Resuscitation. 2012;83:1078–84.
Orlowski JP, Cramer CL. The drowning risks associated with visiting family or friends. J Pediatr Intensive Care. 2012;1:31–5.
Champigneulle B, Bellenfant-Zegdi F, Follin A, Lebard C, Guinvarch A, Thomas F, Pirracchio R, Journois D. Extracorporeal life support (ECLS) for refractory cardiac arrest after drowning: an 11-year experience. Resuscitation. 2015;88:126–31.
World Health Organization. Global report on drowning: preventing a leading killer. 2014. http://www.who.int/violence_injury_prevention/global_report_drowning/en/. Accessed 14 Dec 2017.
Idris AH, Bierens JJLM, Perkins GD, Wenzel V, Nadkarni V, Morley P, Warner DS, Topjian A, Venema AM, Branche CM, Szpilman D, Morizot-Leite L, Nitta M, Løfgren B, Webber J, Gräsner J, Beerman SB, Youn CS, Jost U, Quan L, Dezfulian C, Handley AJ, Hazinski MF. 2015 revised Utstein-style recommended guidelines for uniform reporting of data from drowning-related resuscitation: an ILCOR advisory statement. Circ Cardiovasc Qual Outcomes. 2017;10(7).
Idris AH, Bierens JJLM, Perkins GD, Wenzel V, Nadkarni V, Morley P, Warner DS, Topjian A, Venema AM, Branche CM, Szpilman D, Morizot-Leite L, Nitta M, Løfgren B, Webber J, Gräsner J, Beerman SB, Youn CS, Jost U, Quan L, Dezfulian C, Handley AJ, Hazinski MF. 2015 revised Utstein-style recommended guidelines for uniform reporting of data from drowning-related resuscitation. Resuscitation. 2017;118:147–58.
Buick JE, Lin S, Rac VE, Brooks SC, Kierzek G, Morrison LJ. Drowning: an overlooked cause of out-of-hospital cardiac arrest in Canada. CJEM. 2013;15:1–8.
Nitta M, Kitamura T, Iwami T, Nadkarni VM, Berg RA, Topjian AA, Okamoto Y, Nishiyama C, Nishiuchi T, Hayashi Y, Nishimoto Y, Takasu A. Out-of-hospital cardiac arrest due to drowning among children and adults from the Utstein Osaka Project. Resuscitation. 2013;84:1568–73.
Suominen PK, Vallila NH, Hartikainen LM, Sairanen HI, Korpela RE. Outcome of drowned hypothermic children with cardiac arrest treated with cardiopulmonary bypass. Acta Anaesthesiol Scand. 2010;54:1276–81.
Hess EP, Campbell RL, White RD. Epidemiology, trends, and outcome of out-of-hospital cardiac arrest of non-cardiac origin. Resuscitation. 2007;72:200–6.
Franek O, Pokorna M, Sukupova P. Pre-hospital cardiac arrest in Prague, Czech Republic--the Utstein-style report. Resuscitation. 2010;81:831–5.
Foltin GL, Richmond N, Treiber M, Skomorowsky A, Galea S, Vlahov D, Blaney S, Kusick M, Silverman R, Tunik MG. Pediatric prehospital evaluation of NYC cardiac arrest survival (PHENYCS). Pediatr Emerg Care. 2012;28:864–8.
Kitamura T, Kiyohara K, Sakai T, Iwami T, Nishiyama C, Kajino K, Nishiuchi T, Hayashi Y, Katayama Y, Yoshiya K, Shimazu T. Epidemiology and outcome of adult out-of-hospital cardiac arrest of non-cardiac origin in Osaka: a population-based study. BMJ Open. 2014;4:e006462. https://doi.org/10.1136/bmjopen-2014-006462.
Eschmann NM, Pirrallo RG, Aufderheide TP, Lerner EB. The association between emergency medical services staffing patterns and out-of-hospital cardiac arrest survival. Prehosp Emerg Care. 2010;14:71–7.
Papa L, Hoelle R, Idris A. Systematic review of definitions for drowning incidents. Resuscitation. 2005;65:255–64.
Donoghue AJ, Nadkarni V, Berg RA, Osmond MH, Wells G, Nesbitt L, Stiell IG, CanAm Pediatric Cardiac Arrest Investigators. Out-of-hospital pediatric cardiac arrest: an epidemiologic review and assessment of current knowledge. Ann Emerg Med. 2005;46:512–22.
Schilling UM, Drowning BM. Minerva Anestesiol. 2012;78:69–77.
Szpilman D, Bierens JJLM, Handley AJ, Orlowski JP. Current concepts drowning. N Engl J Med. 2012;366:2102–10.
Tourigny PD, Hall C. Diagnosis and Management of Environmental Thoracic Emergencies. Emerg Med Clin North Am. 2012;30:501.
Bjornsson HM, Marelsson S, Magnusson V, Sigurdsson G, Thornorgeirsson G. Prehospital cardiac life support in the Reykjavik area 1999–2002. Laeknabladid. 2006;92:591–7.
Hausser J, Drowning NM. Rev Med Suisse. 2007;3:1834–8.
Schmidt A, Sempsrott J. Near drowning and adult respiratory distress syndrome. J Emerg Med. 2015;48:e47.
Bierens JJ, Warner DS. Drowning resuscitation requires another state of mind. Resuscitation. 2013;84:1467–9.
Sempsrott J, Slattery D, Schmidt A, Penalosa B, Crittle T. Systematic review of non-Utstein style drowning terms. Ann Emerg Med. 2011;58:S321.
Warner DS, Bierens JJLM, Beerman SB, Katz LM. Drowning a cry for help. Anesthesiology. 2009;110:1211–3.
van Beeck E, Branche C, Szpilman D, Modell J, Bierens J. A new definition of drowning: towards documentation and prevention of a global public health problem. Bull World Health Organ. 2005;83:853–6.
Lunetta P, Modell J, Sajantila A. What is the incidence and significance of “dry-lungs” in bodies found in water? Am J Forensic Med Pathol. 2004;25:291–301.
Lence EM, Ramos NG, Carriedo CS, Garcia-Ochoa JMB, Corral ET. Out-of-hospital cardiorespiratory arrest in children with trauma. Resuscitation. 2014;85:S92.
Newton T, Patterson LZ, Cindrich LA, Sills R, Babcock CI. Outcome of out-of-hospital infant cardiac arrest presenting with asystole as initial rhythm. Ann Emerg Med. 2013;62:S143–4.
Shin SD, Ro YS, Song KJ, Lee EJ, Ahn KO. Epidemiology and outcomes of emergency medical services-assessed out-of-hospital cardiac arrest in Korea: a nationwide observational study from 2006 to 2010. Circulation. 2012;126:A230.
Lin C, Chiang W, Chi C. Use of automated external defibrillators in patients with traumatic out-of-hospital cardiac arrest. Resuscitation. 2012;83:e61.
Tijssen J, Zhan C, Parshuram C, Morrison L, Hutchison J. Critical times in pediatric out-of-hospital cardiac arrest. Crit Care. 2012;16:S97–8.
Webber JB. Drowning, the New Zealand way: prevention, rescue, resuscitation. Resuscitation. 2010;81:S27.
Williams B, Panchal AR, Stolz U, Clark L, Bobrow B, Sanders AB. Cardiocerebral resuscitation improves survival and neurological outcome from out-of-hospital cardiac arrest. Acad Emerg Med. 2010;17:S143.
Auerbach PS, Zafren K. Environmental emergencies: drowning. In: An introduction to clinical emergency medicine; 2012. p. 641–72.
Quan L, Bierens JJLM, Lis R, Rowhani-Rahbar A, Morley P, Perkins GD. Predicting outcome of drowning at the scene: a systematic review and meta-analyses. Resuscitation. 2016;104:63–75.
Acknowledgements
The authors would like to thank K. Sijtsma of the Medical Library of the University Medical Center Groningen for assistance in creating the search terms of this study.
Funding
The research was not funded.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
All authors were involved in the conception and design of the review. AV and AA were involved in the acquisition of the data. AV, AA and JB were involved in the analysis and interpretation of the data. All authors have been involved in drafting the manuscript or revising it critically for important intellectual content. All authors have given final approval of the version to be published.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
AV, AI and JB are members of the writing group on behalf of the ‘2015 Revised Utstein-Style Recommended Guidelines for Uniform Reporting of Data From Drowning-Related Resuscitation: An ILCOR Advisory Statement’ [18, 19].
JB is a consulting governor of the Koninklijke Maatschappij tot Redding van Drenkelingen (Royal Society to Rescue People from Drowning, established in 1767), medical advisor for the Royal Dutch Lifeboat Institution (KNRM) and commissioner of the International Life Saving Federation (ILS) on behalf of the Royal Dutch Lifesaving Association (KNBRD).
AI is a volunteer committee member of the American Heart Association, and receives research funding from the US National Institutes of Health, the US Army, the American Heart Association, and HeartSine, Inc. He serves as a volunteer member of the HeartSine Clinical Advisory Board.
No other potential conflicts of interest exist.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Venema, A.M., Absalom, A.R., Idris, A.H. et al. Review of 14 drowning publications based on the Utstein style for drowning. Scand J Trauma Resusc Emerg Med 26, 19 (2018). https://doi.org/10.1186/s13049-018-0488-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13049-018-0488-z