
Abstract
Background
Resistance to thyroid hormones is a very rare condition, which is often misdiagnosed and mistreated. The cases where there is a concomitant autoimmune thyroid disorder are ultra-rare and particularly challenging to treat. Diagnostic and research-based genomic testing can sometimes identify pathogenic variants unrelated to the primary reason for testing (incidental findings).
Case presentation
We present a patient with thyroid resistance associated with hypothyroid Hashimoto thyroiditis. The long diagnostic odyssey spanning over 20-years included repeated misdiagnoses and mistreatments and was concluded by a research-based genomic testing, identifying a “de novo” THRB pathogenic variant. The varying sensitivity of various tissues to thyroid hormones accompanied by hypothyroid Hashimoto thyroiditis continues to pose a significant treatment challenge.
Conclusions
Thyroid hormone resistance continues to be an un(der)- and misdiagnosed thyroid condition whose management is particularly challenging when associated with autoimmune thyroid disease. Whole exome sequencing has the potential to identify THRB pathogenic variants as incidental findings. Reporting such secondary findings from genomic testing may be particularly important in the context of the rarity of the condition and the potential clinical consequences of misdiagnosis and mistreatment.
Similar content being viewed by others


Introduction
Resistance to thyroid hormones – RTH (OMIM 190160, 188570, 145650) is a rare condition characterised by increased levels of thyroid hormones (particularly free fractions, fT4, fT3) and inappropriately unsuppressed levels of TSH, often in the normal or even increased range [1,2,3]. Although the true prevalence of this condition is not known, it is considered to be a very rare condition affecting about 1 in 40000 people, with about 3000 patients described worldwide so far [1,2,3].
The classical RTH is an autosomal dominant condition due to either germline inherited or ‘de novo’ dominant negative pathogenic variants in the THRB gene (coding for the beta subunit of the thyroid hormone receptor, THRβ), rendering the thyroid receptor less responsive to the thyroid hormones [1,2,3]. Mosaic forms of RTH due to pathogenic variants in THRβ have also been described [4].
The variable expression of THRβ in various tissues resulting in varying degrees of relative thyroid deficit and the increased T4/T3 signalling through the unaffected THRα make it difficult to understand the genotype - phenotype relationship and to make sense of the laboratory results and interpret them in the context of the clinical features in RTH [5, 6]. The clinical features in RTH are highly variable, even within the same family harbouring the same THRβ pathogenic variant [5]. Most patients with RTH present with goitre and/or tachycardia, hyperactive behaviour, and about half of the patients have neurocognitive symptoms including emotional disturbances, anxiety, learning difficulty, developmental delay and intellectual disability. Most patients reach normal stature, but children can have lower body weight and height [1, 3, 7].
The syndrome of RTH, like other rare conditions, poses complex diagnostic and treatment challenges and can lead to long and expensive diagnostic odysseys and suboptimal patient care [8,9,10]. The diagnostic power of genomic testing based on next generation sequencing, has revolutionised the field of rare diseases [11, 12]. Notwithstanding its diagnostic utility, genomic testing also introduced some challenges, such as reporting of incidental (and/or secondary) findings, particularly in the context of genomic testing of children [13, 14]. Despite the ability of genomics to provide diagnosis in 20–60% cases, access to genetic services remains a major challenge in the developing low- and middle-income countries due to lack of genetic resources, infrastructure and expertise [15, 16].
We present a complex case of resistance to thyroid hormones and Hashimoto thyroiditis (HT) with a long diagnostic odyssey ended by genomic testing in a research setting and discuss the challenges of diagnosis and clinical management of this patient with RTH-related unusual thyroid hormones homeostasis combined with a HT-related hypothyroid state.
Case report
The patient is the elder of two sisters in the family, born prematurely at 7-month gestation to non-consanguineous parents and had normal development. She presented for medical attention at age 19 with Jackson-type seizures and was referred for her first thyroid evaluation (6/91, Table 1) due to a history of nervousness, heat intolerance, mild sleep disturbance and heart palpitations. Clinically, she was tachycardic (96 bpm), with sweaty hands, slightly palpable thyroid gland, with no tremor and normal blood pressure. A diagnosis of hyperthyroidism was made based on elevated thyroid hormone levels, and positive antimicrosomal antibodies, despite the unsuppressed TSH levels and the patient was started on antithyroid treatment (6/91, Table 1). In the course of the following 3 years the patient was on and off antithyroid treatment due to exaggerated response to tiamazol (9/91, Table 1) with varying clinical symptoms consistent with hyperthyroid state (4/93). There was a suspicion of high levels of thyroid hormone carriers, which was ruled out by high fT4 levels (1/94, Table 1).
The first clinical suspicion of RTH was documented in 11/94 and corroborated by the high levels of total and free thyroid hormones and unsuppressed TSH, and a result from TRH test under suppression with high dose T3 consistent with RTH. The patient remained without treatment for the following 10-years, and was lost to follow up during the subsequent 8 years. During this period, the patient sought international thyroid expertise, and was diagnosed and treated for thyrotoxicosis based on high total and free thyroid hormone levels and some symptoms consistent with a hyperthyroid state, despite unsuppressed TSH levels. Of note, during this period she was diagnosed with a moderate to severe rheumatoid arthritis (RA) and treated with methotrexate and subsequently with biologic therapy.
In 12/15 (Table 1) the patient presented to our department complaining of feeling tired, slow and intolerant to cold, with levels of thyroid hormones lower and TSH level higher than her usual, elevated levels of cholesterol and weight gain of 17 kg over the preceding 8-year period. Those findings together with positive antithyroid antibodies, palpatory firm gland with non-homogenous hyperechogenic ultrasound appearance lead to the diagnosis of hypothyroid Hashimoto thyroiditis and she was initiated on thyroid replacement treatment.
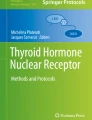
In 2018 our patient was recruited in an international research study approved by the Human Genetic Committees of the Australian National University and The Canberra Hospital and underwent whole exome sequencing. The details of the used genomic and bioinformatic methodology is described elsewhere [17]. This testing identified a “de novo” pathogenic variant (with confirmed paternity and maternity, data not shown) in the beta subunit of the thyroid hormone receptor, THRB p.Arg228Trp) leading to RTH (Fig. 1). This variant has been described in more than 30 families/cases with RTH so far [18], and has not been described in the databases of human variation (dbSNP, 1000 genomes). The variant affects an evolutionary highly conserved amino acid, is predicted to be damaging/deleterious by in silico prediction tools (PolyPhen, SIFT), and in vitro studies have shown that this variant affects T3 binding to the thyroid hormone receptor [19].

Patient’s pedigree and results from genetic testing. Whole exome sequencing identified a heterozygous “de novo” pathogenic variant NM_001252634.1(THRB):c.1012C > T changing evolutionary conserved amino acid Arg338 to Trp (p.Arg338Trp). The variant was not found in the healthy parents (I:1, I:2) and sister (II:1), both maternity and paternity was confirmed with microsatellite testing (data not shown)
The patient continues to be treated with low doses thyroid replacement therapy, mostly based on clinical features, taking into consideration her personal usual levels of thyroid hormones and TSH. The ongoing challenge is judging her thyroid state clinically given the variable distribution of alpha and beta thyroid hormone receptors leading to discrepant symptoms of hyperthyroidism (tachycardia, sweating) and hypothyroidism (hypercholesterolemia, weight gain, cold intolerance).
Discussion
We present an unusual and rare case of rare RTH and hypothyroid HT. As other in other cases, the RTH in our case was initially misdiagnosed and mistreated as autoimmune thyrotoxicosis aiming to reduce thyroid hormone levels, which should be avoided particularly in pregnant patients [3, 20,21,22,23]. We would argue that the same holds true in (young) children with RTH, where antithyroid treatment could be dangerous and potentially detrimental to the intellectual development. Unfortunately, given no prior clinical experience with this very rare condition and lack of access to genetic testing services and clinical genetics support, the diagnosis of RTH in this patient was not confirmed until 24 years later. This long diagnostic odyssey contributed to patient’s mistrust and frequent change of thyroid specialists, which at some stage lead to the correct clinical diagnosis of thyroid hormone resistance, but also prompted the patient to seek second opinions from thyroid physicians, including international experts, which ultimately lead to repeated misdiagnosis and mistreatment with antithyroid medications.
Our case was made more challenging by the co-existence of HT, formally diagnosed later in the course of the disease. For a while, the thyroid autoimmune process in our patient was detectable only on level of positive thyroid autoantibodies and later it manifested with increasing level of thyroid autoantibodies, ultrasonographic changes consistent with inflammation and overt clinical hypothyroidism with increased levels of TSH (compared to the usual in this patient) - established the diagnosis of HT and prompted treatment with thyroid hormone replacement which is ongoing at this point in time [24]. The association between autoimmunity and RTH and the possible underlying mechanisms remain anecdotal [25] and there are isolated reports of both RTH associated with Graves disease [26,27,28,29,30] and Hashimoto thyroiditis [31,32,33,34,35,36] – all emphasising the diagnostic and management challenges posed by these associations, cautioning about the possibility of erroneous diagnosis and treatment.
Our case is unusual in that the genetic diagnosis was established by genomic testing, using whole exome sequencing. While the genetic test did not find a causative variant for the immune-mediated conditions in the patient (RA and HT), it detected a pathogenic THRB variant causing RTH. This finding could be considered an “incidental” finding in the context of the primary autoimmunity focus of our research project, and pose the dilemma of reporting an incidental finding for a condition (RTH) which affects the same organ (thyroid axis) as the primary condition (HT) [13]. This consideration prompted us to ask the question whether the THRB gene should be nominated for the list of reportable “actionable” incidental findings [13, 37]. In the context of increased use of genomic testing in children (including young children and even newborn babies), it is plausible that there may be instances where children with RTH and pathogenic THRB variants are sequenced for unrelated reasons, but would benefit greatly from having the information about having RTH, which could prevent misdiagnosis and potentially harmful consequences of iatrogenic hypothyroidism induced by treatment with antithyroid medications. We also wonder about the full applicability of the protocol used to assess the “clinical actionability” associated with genomic variation [37] in the context of such a rare disease as RTH, for which it may be a while before we have clinical practice guidelines, or high-level evidence from systemic reviews and/or meta-analyses.
Conclusion
In conclusion, RTH is a very rare and often misdiagnosed and mistreated condition, often creating a long diagnostic odyssey due to lack of access to genetic services. When recognised RTH poses a significant treatment challenge, particularly when combined with a more common autoimmune thyroid disease. Elevated levels of thyroid hormones, particularly fT4 and fT3, with unsuppressed TSH levels should raise suspicion of RTH and prompt referral to a tertiary thyroid centre with capacity to differentiate and established this rare diagnosis.
Availability of data and materials
Please contact corresponding author for data requests.
Abbreviations
- (f)T3:
-
(free) triiodothyronine
- (f)T4:
-
(free) thyroxine
- HT:
-
Hashimoto thyroiditis
- RA:
-
Rheumatoid arthritis
- RTH:
-
Resistance to thyroid hormones
- THRB:
-
Thyroid hormone receptor beta subunit gene
- TSH:
-
Thyroid stimulating hormone
References
Agrawal NK, Goyal R, Rastogi A, Naik D, Singh SK. Thyroid hormone resistance. Postgrad Med J. 2008;84(995):473–7.
Cyniak-Magierska A. The syndromes of reduced sensitivity to thyroid hormone – the current state of art. Thyroid Res. 2015;8:A5.
Dumitrescu AM, Refetoff S. The syndromes of reduced sensitivity to thyroid hormone. Biochim Biophys Acta. 2013;1830(7):3987–4003.
Mamanasiri S, Yesil S, Dumitrescu AM, Liao XH, Demir T, Weiss RE, et al. Mosaicism of a thyroid hormone receptor-beta gene mutation in resistance to thyroid hormone. J Clin Endocrinol Metab. 2006;91(9):3471–7.
Ortiga-Carvalho TM, Sidhaye AR, Wondisford FE. Thyroid hormone receptors and resistance to thyroid hormone disorders. Nat Rev Endocrinol. 2014;10(10):582–91.
Visser WE. Disorders of the thyroid hormone transporters and receptors. In: Luster M, Duntas HL, Wartofsky L, editors. The thyroid and its diseases, a comprehensive guide for the clinician. Cham: Switzerland Springer; 2019. p. 49–60.
Rivas AM, Lado-Abeal J. Thyroid hormone resistance and its management. Proc (Bayl Univ Med Cent). 2016;29(2):209–11.
Carmichael N, Tsipis J, Windmueller G, Mandel L, Estrella E. "is it going to hurt?": the impact of the diagnostic odyssey on children and their families. J Genet Couns. 2015;24(2):325–35.
Lopes MT, Koch VH, Sarrubbi-Junior V, Gallo PR, Carneiro-Sampaio M. Difficulties in the diagnosis and treatment of rare diseases according to the perceptions of patients, relatives and health care professionals. Clinics (Sao Paulo). 2018;(73):e68.
Stoller JK. The challenge of rare diseases. Chest. 2018;153(6):1309–14.
Sawyer SL, Hartley T, Dyment DA, Beaulieu CL, Schwartzentruber J, Smith A, et al. Utility of whole-exome sequencing for those near the end of the diagnostic odyssey: time to address gaps in care. Clin Genet. 2016;89(3):275–84.
Wright CF, FitzPatrick DR, Firth HV. Paediatric genomics: diagnosing rare disease in children. Nat Rev Genet. 2018;19(5):253–68.
Kalia SS, Adelman K, Bale SJ, Chung WK, Eng C, Evans JP, et al. Recommendations for reporting of secondary findings in clinical exome and genome sequencing, 2016 update (ACMG SF v2.0): a policy statement of the American College of Medical Genetics and Genomics. Genet Med. 2017;19(2):249–55.
Botkin JR, Belmont JW, Berg JS, Berkman BE, Bombard Y, Holm IA, et al. Points to consider: ethical, legal, and psychosocial implications of genetic testing in children and adolescents. Am J Hum Genet. 2015;97(1):6–21.
Kingsmore SF, Lantos JD, Dinwiddie DL, Miller NA, Soden SE, Farrow EG, et al. Next-generation community genetics for low- and middle-income countries. Genome Med. 2012;4(3):25.
WHO. Medical genetic services in developing countries. https://apps.who.int/iris/bitstream/handle/10665/43288/924159344X_eng.pdf?sequence=1&isAllowed=y (accessed April, 2019). 2006.
Arsov T, Sestan M, Cekada N, Frkovic M, Andrews D, He Y, et al. Systemic lupus erythematosus: a new autoimmune disorder in kabuki syndrome. Eur J Med Genet. 2018.
Guo QH, Wang BA, Wang CZ, Wang M, Lu JM, Lv ZH, et al. Thyroid hormone resistance syndrome caused by heterozygous A317T mutation in thyroid hormone receptor beta gene: report of one Chinese pedigree and review of the literature. Medicine (Baltimore). 2016;95(33):e4415.
Sasaki S, Nakamura H, Tagami T, Miyoshi Y, Nogimori T, Mitsuma T, et al. Pituitary resistance to thyroid hormone associated with a base mutation in the hormone-binding domain of the human 3,5,3′-triiodothyronine receptor-beta. J Clin Endocrinol Metab. 1993;76(5):1254–8.
Refetoff S. Resistance to thyroid hormone: an historical overview. Thyroid. 1994;4(3):345–9.
Weiss RE, Dumitrescu A, Refetoff S. Approach to the patient with resistance to thyroid hormone and pregnancy. J Clin Endocrinol Metab. 2010;95(7):3094–102.
Weiss RE, Refetoff S. Thyroid hormone resistance syndromes. In: Luster M, Duntas HL, Wartofsky L, editors. The thyroid and its diseases, a comprehensive guide for the clinician. Cham: Switzerland Springer; 2019. p. 741–51.
Weiss RE. Endocrinology Advisor. Endocrinology Metabolism. Thyroid hormone resistance. https://www.endocrinologyadvisor.com/home/decision-support-in-medicine/endocrinology-metabolism/thyroid-hormone-resistance-2/ (accessed April 2019). 2017.
Caturegli P, De Remigis A, Rose NR. Hashimoto thyroiditis: clinical and diagnostic criteria. Autoimmun Rev. 2014;13(4–5):391–7.
Barkoff MS, Kocherginsky M, Anselmo J, Weiss RE, Refetoff S. Autoimmunity in patients with resistance to thyroid hormone. J Clin Endocrinol Metab. 2010;95(7):3189–93.
Ogawa K, Yoshida M, Hayashi Y, Murata Y, Miyata M, Oiso Y. A rare case of resistance to thyroid hormone coexisting with Graves' disease. Endocrine. 2011;40(2):318–9.
Sato H. Clinical features of primary hyperthyroidism caused by Graves' disease admixed with resistance to thyroid hormone (P453T). Endocr J. 2010;57(8):687–92.
Shiwa T, Oki K, Awaya T, Nakanishi S, Yamane K. Resistance to thyroid hormone accompanied by Graves' disease. Intern Med. 2011;50(18):1977–80.
Sivakumar T, Chaidarun S. Resistance to thyroid hormone in a patient with coexisting Graves' disease. Thyroid. 2010;20(2):213–6.
Sun H, Xu S, Xie S, Cao W, Chen G, Di H, et al. Graves' disease coexisting with resistance to thyroid hormone: a rare case. Clin Case Rep. 2018;6(2):337–41.
Aksoy DY, Gurlek A, Ringkananont U, Weiss RE, Refetoff S. Resistance to thyroid hormone associated with autoimmune thyroid disease in a Turkish family. J Endocrinol Investig. 2005;28(4):379–83.
Fukata S, Brent GA, Sugawara M. Resistance to thyroid hormone in Hashimoto's thyroiditis. N Engl J Med. 2005;352(5):517–8.
Jonas C, Daumerie C. Conservative management of pregnancy in patients with resistance to thyroid hormone associated with Hashimoto's thyroiditis. Thyroid. 2014;24(11):1656–61.
Wu D, Guo R, Guo H, Li Y, Guan H, Shan Z. Resistance to thyroid hormone beta in autoimmune thyroid disease: a case report and review of literature. BMC Pregnancy Childbirth. 2018;18(1):468.
Ch’ng TW, Chin VL. Challenging diagnosis of thyroid hormone resistance initially as Hashimoto's thyroiditis. J Pediatr Endocrinol Metab. 2019;32(2):203–6.
Kammoun I, Bouzid C, Kandara H, Ben Salem L, Turki Z, Ben SC. A case of resistance to thyroid hormone with chronic thyroiditis: discovery of a novel mutation (I54V). Case Rep Endocrinol. 2011;2011:584930.
Hunter JE, Irving SA, Biesecker LG, Buchanan A, Jensen B, Lee K, et al. A standardized, evidence-based protocol to assess clinical actionability of genetic disorders associated with genomic variation. Genet Med. 2016;18(12):1258–68.
Acknowledgements
Not applicable.
Funding
NHMRC Centre of Research Excellence grant (2015–2019) APP1079648 entitled “Genetic and cellular analysis of autoimmune and inflammatory disease”.
Author information
Authors and Affiliations
Contributions
OV provided clinical data. TA, CV, CX, NS and DA were involved in the bioinformatic assembly, genomic analysis and variant interpretation. OV, TA and CV drafted the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written informed consent for genetic testing as part of a research study was obtained from the patient and family members. The study was approved by the Human Ethics Committees of the Australian National University and Canberra Teaching Hospital (Canberra, Australia).
Consent for publication
Not applicable.
Competing interests
The authors have no competing interests to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Arsov, T., Xie, C., Shen, N. et al. Genomic test ends a long diagnostic odyssey in a patient with resistance to thyroid hormones. Thyroid Res 12, 7 (2019). https://doi.org/10.1186/s13044-019-0068-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13044-019-0068-y