
Abstract
The new human coronavirus named SARS-CoV-2 is a positive-sense RNA virus for which no specific drugs are currently available. A knowledge-based analysis strongly suggests a possible repositioning of the anti-HCV direct antiviral agent (DAA) Sofosbuvir as treatment for SARS-CoV-2. Indeed, the RNA-dependent RNA-polymerases (RdRp) of the two viruses show high sequence and structural homology, supporting the likelihood of binding the Sofosbuvir molecule with similar efficiency. Such a repositioning would allow the containment of the SARS-CoV-2 pandemic and limit the progression of disease to potentially deadly COVID19.
Similar content being viewed by others


A new human coronavirus named SARS-CoV-2 was identified in several cases of acute respiratory syndrome in Wuhan, China in December 2019 [1, 2]. The transmission pathways of the new coronavirus include direct transmission (coughing, sneezing and inhalation transmission of droplets) and transmission by contact with mucosa [3]. The viral load of SARS-CoV-2 in saliva can exceed 1 × 108 viral copies per milliliter [4] both in symptomatic and asymptomatic positive subjects [5].
Consequently, it is necessary to reduce or block viral replication to avoid the progression of the disease towards the full-blown and potentially lethal form (COVID19), but also to reduce the viral titer and viral shedding through saliva, in symptomatic and asymptomatic infected individuals.
Specific drugs for SARS-CoV-2 are obviously not available. Currently, drugs originally developed for HIV (e.g. lopinavir, ritonavir) are under evaluation on the basis of weak evidences from retrospective analyses suggesting clinical benefit in the treatment of the two previous coronavirus epidemics [6]. Similarly, anti-malaria chloroquine or hydroxychloroquine are tested [7]. The inhibitor of Influenza’s polymerase Favipiravir is currently evaluated in a clinical trial in combination with anti-IL-6 receptor Tocilizumab (NCT04310228). Finally, the inhibitor of Ebolavirus’ polymerase Remdesivir is currently evaluated in two major SIMPLE clinical trials (NCT04292899; NCT04257656) [8]. On Apr. 29, 2020 it was announced that results from the trial NCT04292899 showed clinical improvement for 50 percent of patients in 10 days in the 5-day treatment group and 11 days in the 10-day treatment group (https://www.gilead.com/news-and-press/press-room/press-releases/2020/4/gilead-announces-results-from-phase-3-trial-of-investigational-antiviral-remdesivir-in-patients-with-severe-covid-19). However, a trial conducted in China showed Remdesivir did not improve patients’ condition nor reduced the positivity to virus. Moreover, the drug showed also significant side effects (https://www.ft.com/content/0a4872d1-4cac-4040-846f-ce32daa09d99).
In the search of the potential best candidate drugs to be repositioned, structural analyses comparing target molecules in the different pathogens should be applied in order to guide a knowledge-based decision process [9].
In the specific case of SARS-CoV-2, and in general in the case of RNA viruses, the most specific target is represented by the RNA-dependent RNA-polymerase (RdRp) which is specific to each RNA virus, regardless the polarity of the viral RNA genome [10, 11]. Nevertheless, significant differences are identified between RdRp from positive-sense and negative-sense RNA viruses [12]. The latter observation strongly suggests that repositioning of antiviral drugs should take into consideration the molecular basis of the genomic viral RNA.
SARS-CoV-2 is a positive-sense RNA virus. The only positive-sense RNA virus, for which a very effective drug targeting specifically the RdRp is available and approved world-wide for clinical use, is hepatitis C virus (HCV). In the specific, Sofosbuvir (Sovaldi®; Epclusa® by Gilead) is a direct antiviral agent (DAA) that inhibits the hepatitis C NS5B RdRp protein [13]. Interestingly, it has been already shown to be effective in vitro and in humans for other two different positive-sense RNA viruses, namely Yellow Fever and Hepatitis A virus [14, 15].
The alignment of RdRp sequences from HCV and the three epidemic/pandemic coronaviruses, confirms the high homology and conservation in several residues along the sequence and in particular in the Motif B and C. On the contrary, such homology is almost lost when RdRp sequences from the three epidemic/pandemic coronaviruses are aligned with those from negative-sense RNA viruses, namely Ebola, Influenza, Rabies and Vesicular Stomatitis viruses [16].
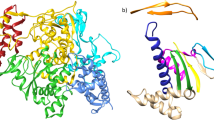
The structure modeling shows that RdRp of positive-sense (HCV and SARS-CoV-2) and negative-sense (i.e. Influenza) RNA viruses are significantly different, but they all show the formation of the Motif C β-strand-loop-β-strand structure. However, only the alignment of RdRp structures from the two positive-sense RNA viruses shows a superimposition of the two Motifs C [16].
All these sequence and structural modelling evidences strongly support the concept that the SARS-CoV-2 RdRp is much more similar to the one from HCV than the one from negative-sense Influenza and Ebola RNA viruses. Therefore, repositioning of Sofosbuvir (Sovaldi®; Epclusa® by Gilead), the inhibitor of the HCV NS5B RdRp protein, as antiviral in the treatment of the SARS-CoV-2 infection has an extremely high potentiality of success, as recently postulated by others [17], and is suggested as a potential drug for the treatment of COVID-19 in the very recent EASL-ESCMID position paper [18]. This is further supported by the great diversity between the molecular structure of the Sofosbuvir and the inhibitors of Influenza and Ebola viruses currently evaluated in clinical trials (Fig. 1).

Comparison of RdRp inhibitors of RNA viruses. The structure of the RNA-dependent RNA-polymerase inhibitors in clinical trial, Favipiravir (developed for the influenza virus) and Remdesivir (developed for the Ebola virus) are shown together with Sofosbuvir (developed for the HCV)
Moreover, Sofosbuvir is a prodrug of the protide type and is metabolized to the active antiviral agent GS-461203 (2′-deoxy-2′-α-fluoro-β-C-methyluridine-5′-triphosphate) in the liver. The enzymes involved in such activation are cathepsin A and the histidine triad nucleotide-binding protein 1 (HINT1), and subsequent repeated phosphorylation. All these enzymes have RNA and protein expression in the lung cells comparable to liver cells, ensuring the appropriate activation of the Sofosbuvir to become an effective substrate of the SARS-CoV-2 RdRp in the target cells of the respiratory tract.
In conclusion, the data here reported indicate the Sofosbuvir as the lead compound with the highest potential of antiviral efficacy in SARS-CoV-2 infection. In addition, the long-lasting use in patients for treating and eradicating HCV chronic infection provides also the full knowledge of its safety profile [13]. If the evaluation in humans will hold the premises of the in silico analyses, Sofosbuvir will become an extraordinary therapeutic tool to inhibit the SARS-CoV-2 replication and, ultimately, to make the current pandemic a manageable disease.
Availability of data and materials
N/A
References
Hui DS, Azhar I, Madani TA, Ntoumi F, Kock R, Dar O, et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health - the latest 2019 novel coronavirus outbreak in Wuhan, China. Int J Infect Dis. 2020;91:264–6.
Bogoch II, Watts A, Thomas-Bachli A, Huber C, Kraemer MUG, Khan K. Potential for global spread of a novel coronavirus from China. J Travel Med. 2020;27(2):taaa011. https://doi.org/10.1093/jtm/taaa011. PMID: 31985790.
Lu CW, Liu XF, Jia ZF. 2019-nCoV transmission through the ocular surface must not be ignored. Lancet. 2020;395:e39.
To KK, Tsang OT, Chik-Yan YC, Chan KH, Wu TC, Chan JMC, et al. Consistent detection of 2019 novel coronavirus in saliva. Clin Infect Dis. 2020;ciaa149. https://doi.org/10.1093/cid/ciaa149. Online ahead of print.
Rothe C, Schunk M, Sothmann P, Bretzel G, Froeschl G, Wallrauch C, et al. Transmission of 2019-nCoV infection from an asymptomatic contact in Germany. N Engl J Med. 2020;382:970–1.
Chu CM, Cheng VC, Hung IF, Wong MM, Chan KH, Chan KS, et al. Role of lopinavir/ritonavir in the treatment of SARS: initial virological and clinical findings. Thorax. 2004;59:252–6.
Cortegiani A, Ingoglia G, Ippolito M, Giarratano A, Einav S. A systematic review on the efficacy and safety of chloroquine for the treatment of COVID-19. J Crit Care. 2020;S0883-9441(20)30390–7. https://doi.org/10.1016/j.jcrc.2020.03.005. Online ahead of print.PMID: 32173110.
Agostini ML, Andres EL, Sims AC, Graham RL, Sheahan TP, Lu X et al.: Coronavirus Susceptibility to the Antiviral Remdesivir (GS-5734) Is Mediated by the Viral Polymerase and the Proofreading Exoribonuclease. mBio 2018;9(2):e00221-18. https://doi.org/10.1128/mBio.00221-18.
Talevi A, Bellera CL. Challenges and opportunities with drug repurposing: finding strategies to find alternative uses of therapeutics. Expert Opin Drug Discov. 2020;15:397–401.
Jia H, Gong P. A structure-function diversity survey of the RNA-dependent RNA polymerases from the positive-Strand RNA viruses. Front Microbiol. 2019;10:1945.
Jacome R, Becerra A, de LS P, Lazcano A. Structural Analysis of Monomeric RNA-Dependent Polymerases: Evolutionary and Therapeutic Implications. PLoS One. 2015;10:e0139001.
Poch O, Sauvaget I, Delarue M, Tordo N. Identification of four conserved motifs among the RNA-dependent polymerase encoding elements. EMBO J. 1989;8:3867–74.
Bourliere M, Pietri O. Hepatitis C virus therapy: no one will be left behind. Int J Antimicrob Agents. 2019;53:755–60.
Mendes EA, Pilger DRB, Santos Nastri ACS, Malta FM, Pascoalino BDS, Carneiro D'Albuquerque LA, et al. Sofosbuvir inhibits yellow fever virus in vitro and in patients with acute liver failure. Ann Hepatol. 2019;18:816–24.
Jiang W, Muhammad F, Ma P, Liu X, Long G. Sofosbuvir inhibits hepatitis a virus replication in vitro assessed by a cell-based fluorescent reporter system. Antivir Res. 2018;154:51–7.
Buonaguro L, Tagliamonte M, Tornesello ML, Buonaguro FM. SARS-CoV-2 RNA polymerase as target for antiviral therapy. J Transl Med In press 2020;18(1):185. https://doi.org/10.1186/s12967-020-02355-3. PMID: 32370758.
ElFiky AA. Anti-HCV, nucleotide inhibitors, repurposing against COVID-19. Life Sci. 2020;248:117477.
Boettler T, Newsome PN, Mondelli MU, Maticic M, Cordero E, Cornberg M, et al. Care of patients with liver disease during the COVID-19 pandemic: EASL-ESCMID position paper. JHEP Rep. 2020;2:100113.
Acknowledgements
N/A
Funding
H2020 Transcan2—HEPAMUT project (Grant Nr. 643638) (LB); Italian Ministry of Health through Institutional “Ricerca Corrente” (LB); POR FESR 2014/2020 “Campania OncoTerapie” (LB).
Author information
Authors and Affiliations
Contributions
LB conceived the concept; FMB contributed to the concept; LB drafted the manuscript; LB and FMB revised the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
N/A
Consent for publication
N/A
Competing interests
Authors declare the absence of any competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Buonaguro, L., Buonaguro, F.M. Knowledge-based repositioning of the anti-HCV direct antiviral agent Sofosbuvir as SARS-CoV-2 treatment. Infect Agents Cancer 15, 32 (2020). https://doi.org/10.1186/s13027-020-00302-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13027-020-00302-x