
Abstract
Background
Atrial septal defect (ASD) closure has been widely accepted and is now routinely performed using a percutaneous approach under especially echocardiographic guidance Transesophageal echocardiography (TEE). One major complication is dislocation of occluder device during or after the device implantation. Surgical removal may be required, especially when the device stuck in the left ventricular outflow tract (LVOT).
Case introduction
A 21-year-old female was admitted to our department for percutaneous closure of secundum ASD. Percutaneous closure under the guidance of TEE was recommended for the patients. During device implantation, the TEE showed dislocation of the 22 mm ASD occluder device, stucked into the LVOT and behind the anterior mitral leaflet, producing severe LVOT obstruction Fig. 1). We herein present a safe and quick technique for surgical removal of an ASD occlude device located in the LVOT.
Conclusion
This technique provides a safe method for surgical removal of malposition and migration ASD occluder device.
Similar content being viewed by others


Background
Atrial septal defect (ASD) is one of the most common congenital anomalies. Percutaneous closure of secundum ASD has evolved over the past three decades, and is considered a standard treatment for ASD in recent years [1]. Although infrequent, complications such as arrhythmia, embolization, thrombosis, dislocation of occluder device and perforation have been reported associated with this procedure [2]. The occluder device be retrieved percutaneously sometimes, however surgical removal may be needed, especially when the device stuck in the LVOT and left atrial disk towards the ASD. It is difficult to remove the device without damage to the chordae and mitral valve. We present a safe and quick technique for surgical removal of ASD closure device stuck in the LVOT behind the anterior mitral leaflet.
Case report
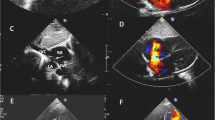
A 21-year-old female was admitted to our department for percutaneous closure of secundum ASD because of progressive decrease in exercise tolerance. Transthoracic echocardiography (TTE) revealed a 16 mm secundum ASD with adequate rims, the posterior rim, superior rim, inferior rim were 10 mm, 12 mm, 16 mm respectively. Left to right shunt and moderate right-sided heart enlargement were also proved by TTE. Percutaneous closure under the guidance of TEE with 22 mm ASD occluder device was recommended for the patients. During device implantation, the TEE showed dislocation of the 22 mm ASD occluder device (Shanghai Shape Memory Alloy, China), stucked into the LVOT and behind the anterior mitral leaflet, producing severe LVOT obstruction (Fig. 1, videos 1 and 2).

TEE showed the ASD occluder device trapped in into the LVOT and behind the anterior mitral leaflet, producing severe LVOT obstruction
Additional file 1: Video 1.
Additional file 2: Video 2.
Emergent surgical removal of the ASD occluder device was performed immediately with general anesthesia. A standard median sternotomy was performed in the patient, after institution of cardiopulmonary bypass, The ASD was approached via right atriotomy. The ASD occluder device was stuck in the LVOT, behind the anterior mitral leaflet, twined by the mitral chordae and the left atrial disk towards the ASD, making it difficult to hold the device by its screw located on the right atrial disk. So 3/0 prolene suture is placed through the middle of the device in the right disk of the occluder device. Then the 3/0 prolene suture is passed through a 16F soft plastic snugger (Shanghai Shape Memory Alloy, China) which is advanced well into the ASD avoiding of any chordal apparatus. As the suture is pulled, the ASD occlude device is gradually retrieved into the snugger. Finally, the snugger can be removed from the heart safely with the compressed device inside (Fig. 2), then the ASD was closed with pericardial patch. The postoperative course was uneventful.

Retrieval of ASD occluder device into a snugger to facilitate safe removal from the LVOT when the left atrial disk towards the ASD
Discussion
Recently improvements in device design and operator experience have resulted in increasing adoption of percutaneous ASD closure, complications such as arrhythmia, embolization, thrombosis, dislocation of occluder device and perforation have been reported associated with this procedure [2, 3]. Device malposition and migration are one of the major complications following ASD device closure, often requiring emergent or urgent surgical intervention [4]. AND TEE is the important means to get the exact morphology of the ASD, such as the size, position in the interatrial septum, and adequacy of septal rims [5, 6].
Although successful percutaneous retrieval of the device are widely reported in the literature, surgical removal was necessary when the occluder devices are stucked in the special location [5]. Device dislocation generally occur early and may be related to the initial positioning of this device [4], the rim was inadequate especially when retro-aortic rim less than 5 mm [6]. The device dislocation reason of our case is the device cable connecting with the disk was loose during the deployment of the left-sided disk.
Various techniques for surgical removal of closure devices have been reported such as direct retrieval of the deployed device. Such devices are deployed from a sheath and when being removed percutaneously are resheathed for safe removal [7]. However, the authors only described the technique applicable to right atrial disk towards the ASD. Actually, when the left disk of the occluder device towards the ASD and twined by the mitral chordae, the technique also worked. Our technique keep the surgical removal quick and safe and minimize valve damage and conduction system complications. It is important to understand the technique for any cardiac surgeon involved in the care of such patients [7].
Conclusion
This technique provides a safe method for surgical removal of malposition and migration ASD occluder device.
Availability of data and materials
The datasets used are available from the corresponding author on reasonable request.
Abbreviations
- ASD:
-
Atrial septal defect
- TEE:
-
Transesophageal echocardiography
- LVOT:
-
Left ventricular outflow tract
- LV:
-
Left ventricle
- LA:
-
Left atrium
- AO:
-
Aorta
References
Oster M, Bhatt AB, Zaragoza-Macias E, Dendukuri N, Marelli A. Interventional therapy versus medical therapy for Secundum atrial Septal defect: a systematic review (part 2) for the 2018 AHA/ACC guideline for the Management of Adults with Congenital Heart Disease: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Circulation. 2019;139(14):e814–30.
Yang MC, Wu JR. Recent review of transcatheter closure of atrial septal defect. Kaohsiung J Med Sci. 2018;34(7):363–9.
Levi DS, Moore JW. Embolization and retrieval of the Amplatzer septal occluder. Catheter Cardiovasc Interv. 2004;61(4):543–7.
Errahmouni A, Hattaoui ME, Drighil A, Boumzebra D. Silent embolization of an Amplatzer septal occluder into the left ventricular outflow tract requiring emergent surgical retrieval. Ann Pediatr Cardiol. 2012;5(1):89–91.
Shirodkar S, Patil S, Pinto R, Dalvi B. Successful retrieval of migrated Amplatzer septal occluder. Ann Pediatr Cardiol. 2010;3(1):83–6.
O'Byrne ML, Glatz AC, Goldberg DJ, et al. Accuracy of transthoracic echocardiography in assessing retro-aortic rim prior to device closure of atrial Septal defects. Congenit Heart Dis. 2015;10(4):E146–54.
Yates MT, Anderson DR. Safe Surgical Retrieval of Embolized Atrial Septal Defect Closure Device 2017; 103(2):e213–e214.
Acknowledgements
We appreciate Professor Yongjun Qian for his support to this project.
Funding
None.
Author information
Authors and Affiliations
Contributions
WB and HJ contributed to data collection and analysis; WB wrote this article; HJ support and encourage the study. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
None.
Consent for publication
Consent was obtained from the patient for the publication of this report.
Competing interests
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wen, B., He, J. Emergent surgical removal of a migrated atrial septal defect occluder: case report. J Cardiothorac Surg 15, 327 (2020). https://doi.org/10.1186/s13019-020-01350-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13019-020-01350-5