
Abstract
Background
Even though several studies reported donor autologous nerve grafts for digital nerve defects, there is no report in the literature regarding acceptable graft for thumb nerves. The purpose of this study is to provide guidelines for autologous nerve graft selection by detecting similarities between thumb nerve zones and donor nerve with regard to the number of fascicles and cross-sectional area.
Materials and methods
Five cadavers were used in this study. An anatomical zoning system was defined for thumb nerves (zones 1, 2, 3). Sural nerve (SN), medial antebrachial cutaneous nerve (MABCN), lateral antebrachial cutaneous nerve (LABCN), posterior interosseous nerve (PIN), and anterior interosseous nerve (AIN) were selected as donor nerve grafts. The number of fascicles and surface area (mm2) was defined.
Results
The mean of the fascicle number in zone 1, zone 2, zone 3, AIN, PIN, LABCN, MABCN, and SN were 3.8, 4.7, 6.1, 2.2, 1.8, 4.5, 3.1, and 6.4, respectively. The mean of the surface area in zone 1, zone 2, zone 3, AIN, PIN, LABCN, MABCN, and SN were 2.19, 6.26, 4.04, 1.58, 0.71, 5.00, 3.01, and 8.06, respectively.
Conclusions
LABCN is the best choice for all zones that has fascicular matching with all three zones of thumb nerves and caliber matching with zones 2 and 3. In zone 1, the best nerve graft is MABCN which has both suitable caliber and fascicle count.
Similar content being viewed by others


Introduction
Untreated digital nerve injury of the thumb can lead to significant sensory impairment. In cases of nerve gap, an autologous nerve graft is considered as the gold standard to bridge defects [1, 2]. So it is crucial to assess the available donor nerves for reconstructing thumb nerve defects. Several studies reported donor autologous nerve grafts for digital nerve defects, but there is no report in the literature regarding acceptable graft for thumb nerves [3,4,5,6].
Thumbs have four functional muscles that are mostly motor innervated by the lateral terminal branch of the median nerve and then by the deep branch of the ulnar nerve [7]. Generally, the median nerve divides into three common palmar digital nerves, which the first one trifurcates and two of them supply the sides of the thumb. Three variations had been reported by Jolley et al. in thumb-index finger sensory innervations in 1997 [8]. Type I with a rate of 69% has a radial thumb palmar digital nerve and a common palmar digital nerve that bifurcates at the first web space and innervates the ulnar side of the thumb and the radial side of the index finger [8]. Type II has a common thumb palmar digital nerve and a radial index finger digital nerve present in 6% of cases, and type III with a trifurcation of the median nerve has proper digital nerves to radial and ulnar thumb and radial index finger, existing in 25% [8]. In 1985, Hirasawa et al. reported the thumb digital nerve trifurcation into the main, median, and lateral branches before distal palmar thumb crease [9]. In 2002, Higgins et al. tried to cater a nerve graft selection guideline for the middle finger [10], but up to now, no survey for thumb has been done as the main finger for gripping.
Considering the importance of the thumb function in the quality of life and criticality of meticulous nerve repair, this study was designed to provide a guideline for autologous nerve graft selection in case of thumb nerve defects, emphasizing on thumb nerve zone similarities to donor nerve based on histological measurements. As near-matching fascicular patterns and caliber of stumps result in optimum functional recovery, fascicles count and surface area measurements were considered for the present histological assessment [11,12,13].
Methods
At fall 2019, twenty upper and lower limbs of five cadavers were used. At the palmar surface, median nerve ramification is obvious. Based on a defined anatomic zoning system (Fig. 1), zone 3 (distal to the flexor retinaculum and proximal to the metacarpophalangeal joint) consists of two proper palmar digital nerves branched out of the median nerve, while zone 2 (proximal to the interphalangeal joint) encompasses three branches that one of them travels deeply to the dorsal surface. And zone 1 (distal to the interphalangeal joint) contains two branches of the median nerve at the palmar surface. The specimens were harvested from the proximal of each zone to standardize the harvest of thumb nerves by the hand surgeon.

Schematic of thumb nerve zones. The figure illustrates the anatomical description of the palm, emphasizing on palmar digital nerves and zoning of the thumb. Zone 1 = distal to the interphalangeal joint. Zone 2 = proximal to the interphalangeal joint. Zone 3 = distal to the flexor retinaculum and proximal to the metacarpophalangeal joint
The sural nerve (SN), medial antebrachial cutaneous nerve (MABCN), lateral antebrachial cutaneous nerve (LABCN), posterior interosseous nerve (PIN), and anterior interosseous nerve (AIN) were selected as donor nerve grafts. The SN was harvested at the level of the lateral malleolus. The AIN was identified in the proximal border of the pronator quadrates and then the AIN was dissected and harvested at the branching point in the muscle. The PIN was identified at the midpoint of the pronator quadrates muscle belly and harvested by dorsal incision on the distal forearm before entering the wrist joint. The MABCN and LABCN were dissected at the elbow joint between the proximal and middle thirds of the forearm.
Harvested specimens were sectioned and stained by hematoxylin and eosin and examined through an Olympus microscope BX41 in a single-blind manner by the pathologist. Fascicle count and surface area measurements were done. Then data were analyzed using SPSS software, version 22 (SPSS Inc., Chicago, IL, USA). T test was performed to compare the variables, and P values less than 0.05 were considered significant meaning the specimens are not matched. P values more than 0.05 showed that samples were matched with no statistical differences and are appropriate for grafting.
Results
The demographic data of the used cadavers (ranging in age from 68 to 75 years) are mentioned in Table 1. The mean (SD) number of nerve fascicles of all specimens have been shown in Fig. 2. T test analysis revealed that as donor nerves, AIN and PIN fascicle counts differed significantly than all three zones of the thumb (P ≤ 0.001), while LABCN had non-significant differences with all three zones (P = 0.125, P = 0.776, and P = 0.151, respectively, for zone 1, zone 2, and zone 3). MABCN fascicle count differed significantly with zones 2 and 3 (P = 0.035 and P = 0.005, respectively) but showed a non-significant difference with zone 1 (P = 0.168). And SN fascicle count had significant differences with zones 1 and 2 (P = 0.001 and P = 0.012, respectively) but did not differ significantly with zone 3 (P = 0.059).

Fascicle counts in zones of digital nerves and donor nerve grafts. Bar chart showing the mean (SD) of the number of fascicles of different samples. DN, digital nerve; AIN, anterior interosseous nerve; PIN, posterior interosseous nerve; LABCN, lateral antebrachial cutaneous nerve; MABCN, medial antebrachial cutaneous nerve; SN, sural nerve
The mean (SD) surface area (mm2) of cross-sectional matching in all nerve specimens is shown in Fig. 3. T test analysis showed that as donor nerves, just PIN surface area differed significantly than all three zones of thumb (P = 0.004 for zone 1 and P ≤ 0.001 for zones 2 and 3). AIN surface area differed significantly with zones 2 and 3 (P = 0,010 and P = 0.001, respectively) but had no significant difference with zone 1 (P = 0.489).

Cross-sectional assessment in zones of digital nerves and donor nerve grafts. Bar chart showing the mean (SD) of the surface area (mm2) of different samples. DN, digital nerve; AIN, anterior interosseous nerve; PIN, posterior interosseous nerve; LABCN, lateral antebrachial cutaneous nerve; MABCN, medial antebrachial cutaneous nerve; SN, sural nerve
MABCN surface area differed significantly with zone 3 (P = 0.006) but showed non-significant differences with zones 1 and 2 (P = 0.233 and P = 0.279, respectively). LABCN and SN surface areas had significant differences with zone 1 (P = 0.003 and P = 0.001, respectively), while they did not differ significantly with zones 2 and 3 (P = 0.648, P = 0.302 and P = 0.093, P = 0.053, respectively) (Fig. 4).

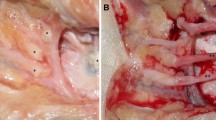
Histopathological sections of the nerves and the method of dimensions and surface area measurement. a Histological section of the medial antebrachial cutaneous nerve (MABCN) shows fascicles number and their arrangement. In this image, you can see 5 fascicles (H&E stain, × 40). b One fascicle (H&E, × 100). c, d Histological section of the lateral antebrachial cutaneous nerve (LABCN) cross-section (c) and longitudinal section (d), in which you can see two fascicles with their measurements including the maximum diameter of each fascicle, surface area of each fascicle, and total surface area of the nerve in pixels. The microscope camera’s software converts the measurements in to millimeters/millimeters2 (H&E stain, × 40)
Discussion
In cases of nerve defect, tension is possible at the repair site. When the injured nerve underwent a high tensile stress by simple microsurgical repair, the best technique for reconstruction is nerve graft or nerve transfer [14,15,16,17]. Although up to now, many techniques including conduits, veins, and allografts have been used to cover finger’s nerve defects, the best is to do autologous nerve graft [18,19,20]. Autografts are superior to the allografts because they are genetically identical with the recipient tissue. So, while allografts take longer time to incorporate into the recipient’s body, autografts decrease clinical failure.
Careful controlled electrolyte homeostasis of neurons makes action potentials and antegrade/retrograde axoplasmic transport of neurotransmitters [4]. Previous studies proved that the only significant elements for functional recovery are entering axons throughout the fascicles, which contain endoneurium [12, 13]. The number of fascicles of palmar digital nerves increases from proximal to distal level (from zone 3 to zone 1), but fascicle diameters are much smaller at the distal portion than the proximal. Also, this number is higher for nerves of the thumb and then the index fingers than the others, as the thumb has the highest fascicle count at proximal and distal levels [21]. The count of myelin nerve fibers normally decreases from proximal to distal level of palmar digital nerves, in which the number of these fibers is higher for the thumb, index, and long fingers and less for the ring and small fingers [21]. Thus, near-matching fascicular patterns of stumps can result in optimum axons sprouting throughout the recipient fascicles [11]. The diameter and cross-sectional area of nerves are important factors in nerve reconstruction. These measurements are nearly the same in palmar digital nerves of the thumb and other fingers [21]. However, for more precise technical success in nerve defect reconstruction, selecting the best cross-section (surface area), the number of fascicles and length match are clinically important to have the best functional outcome. A significantly smaller nerve graft in diameter than the proximal stump of the recipient nerve leads to fascicle lost and the possibility of neuroma formation. Due to more required time for regeneration, excessive length of the graft causes loss in numbers of regenerative fascicles of the nerve graft by increasing the risk of atrophy and fibrous ingrowth [11]. And smaller distal stump of the nerve graft than the distal recipient stump results in no regeneration in some fascicles of the distal recipient nerve end [10, 11]. These mismatchings act as a break in the axonal bilayer lipid membrane and result in irreversible apoptosis [4]. Also, less sutures are needed in caliber matching of two nerve stumps, resulting in less scar formation at the neurorraphy site and more nerve regeneration chance [10, 22]. This study presented that in fascicle counts, LABCN matches with all three zones of thumb digital nerve. while MABCN just matches with zone 1 and SN just matches with zone 3. In cross-sectional matching, MABCN matches with zones 1 and 2 and LABCN and SN match with zones 2 and 3. while AIN just matches with zone 1 of the thumb digital nerve. Thus, for zone 3, SN and LABCN are the best grafts with acceptable matching in caliber and fascicle count. For zone 2, although all three LABCN, MABCN, and SN nerves are suitable in caliber, just LABCN matches the best in fascicle count. And in zone 1, the best nerve graft is MABCN which matches suitable in caliber and either in fascicle count.
Another noticeable factor in selecting a nerve graft is the ease to harvest and yield sensory loss. Among the evaluated nerves for graft, AIN and PIN are technically difficult to harvest with a minimal apparent scar but yield in trivial sensory loss at the donor site. LABCN and MABCN are easier to harvest with less apparent scar but result in significant sensory loss, although the dermatome overlap minimizes that. SN supplies a great long and easy harvesting graft, but with a squalid scar site and sensory loss of lateral aspect of the leg and foot ankle that lessens by time [10].
Higgin’s assay introduced AIN, PIN, and MABCN as caliber matches and LABCN as fascicle count match for fingertip digital nerve (zone 1). And ignoring fascicle match, they suggested PIN as the best one due to ease of harvesting and minimal sensory deficit at the donor site [10]. In the present study, AIN and MABCN are caliber matches, while LABCN and MABCN are fascicle count matches for fingertip digital nerve of thumb (zone 1). Thus, considering all the criteria for selecting the best donor nerve as grafts, this study revealed that MABCN is the best match for zone 1 in caliber and fascicle count.
For zones 2 and 3 of the middle finger, Higgin’s assay suggested LABCN, especially for zone 3 with equal fascicle count. In their point of view, LABCN had minor non-significant differences in caliber and fascicle count and either easy to harvest and negligible consequent sensory deficit because of the dermatome overlap by sensory branches of the radial nerve [10]. This time, although all three MABCN, LABCN, and SN are caliber matches for zone 2, LABCN is the best choice due to its fascicle count matching.
Finally, Higgins et al. introduce SN as the best match for zone 4 of their assay, although it has fewer fascicles and smaller caliber [10]. Here, in the same anatomical level, SN and LABCN match best with zone 3 of the thumb in both fascicle count and caliber. In addition to the surface area, the cross-sectional shape matching is also important. As SN is basically a flap [11], it seems to be more appropriate for zone 3 of the thumb digital nerve, which has either a flap shape.
LABCN nerve graft for fingers’ nerves was firstly done by McFarlane and Mayer in 1976 that 11 of 13 patients showed excellent two-point discrimination between 7 and 20 mm. They also concluded that LABCN has a good length to graft and is easy to obtain [23]. Tank et al. showed that LABCN has more similarity to the fingers’ nerves in the fascicle pattern [12]. Also, some clinical trials such as Schonauer et al., Pilanci et al., and Unal et al.’s works elucidated that more sensory regaining chance at recipient occurred by LABCN as interposed graft and encouraged by the advantage of LABCN uptake from the non-resting area of distal lateral of forearm that makes no critical problem in the patient [24,25,26].
Since Higgins et al. tried to cater a nerve graft selection guideline for the middle finger, the strong point of the present study is introducing a new practical guideline for thumb nerve defects as the main finger for gripping and the importance of its function in quality of life. But the disadvantages were its cadaveric modality and the small sample size of the study. Thus, the effectiveness of this guideline needs to be confirmed by more investigations on patients and correlated with clinical results. Also, it must be considered that axon count can demonstrate more precise results than fascicle count because some nerves have more fascicles with less axon fibers. However, combining such clinical trials with optimizing nerve repair techniques and drugs can be helpful to gain more valuable clinical results [27].
Considering the donor nerve grafts matching with thumb nerve zones in fascicle count and caliber (Table 1), LABCN is the best choice for all zones, which has fascicular matching with all three zones of thumb nerves and caliber matching with zones 2 and 3. This is also the consensus recommendation of literature [10, 28], as despite the notable donor site sensory deficit [10], its harvesting does not make disability and discomfort [28]. After that, SN and MABCN with more caliber matching are good choices. However, in addition to double preparation and anesthesia for SN harvesting than those of the upper limb, its high affinity to form sequelae and symptomatic painful neuroma must be considered [11, 28].
Conclusion
LABCN is the best choice for all zones as it has fascicular matching with all three zones of thumb nerves and caliber matching with zones 2 and 3. In zone 1, the best nerve graft is MABCN which has both suitable caliber and fascicle count.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Mermans JF, et al. Digital nerve injuries: a review of predictors of sensory recovery after microsurgical digital nerve repair. HAND. 2012;7(3):233–41.
Paprottka FJ, et al. Sensory recovery outcome after digital nerve repair in relation to different reconstructive techniques: meta-analysis and systematic review. Plastic Surg Int. 2013;2013:704589.
Chen C, Tang P, Zhang X. Reconstruction of proper digital nerve defects in the thumb using a pedicle nerve graft. Plast Reconstr Surg. 2012;130(5):1089–97.
Grinsell D, Keating C. Peripheral nerve reconstruction after injury: a review of clinical and experimental therapies. Biomed Res Int. 2014;2014:698256.
Poppler LH, et al. Alternatives to sural nerve grafts in the upper extremity. HAND. 2015;10(1):68–75.
Slutsky DJ. A practical approach to nerve grafting in the upper extremity. Atlas Hand Clin. 2005;10(73):e92.
Standring S. Gray’s anatomy e-book: the anatomical basis of clinical practice. Philadelphia: Elsevier Health Sciences; 2015.
Jolley BJ, Stern PJ, Starling T. Patterns of median nerve sensory innervation to the thumb and index finger: an anatomic study. J Hand Surg. 1997;22(2):228–31.
Hirasawa Y, et al. An investigation of the digital nerves of the thumb. Clin Orthop Relat Res. 1985;198:191–6.
Higgins JP, et al. Assessment of nerve graft donor sites used for reconstruction of traumatic digital nerve defects. J Hand Surg. 2002;27(2):286–92.
Wolford LM, Stevao EL, editors. Considerations in nerve repair. Baylor University Medical Center Proceedings. Dallas: Taylor & Francis; 2003.
Tank MS, Lewis RC Jr, Coates PW. The lateral antebrachial cutaneous nerve as a highly suitable autograft donor for the digital nerve. J Hand Surg. 1983;8(6):942–5.
Hudson AR, et al. Peripheral nerve autografts. J Surg Res. 1972;12(4):267–74.
Roganovic Z, Ilic S, Savic M. Radial nerve repair using an autologous denatured muscle graft: comparison with outcomes of nerve graft repair. Acta Neurochir. 2007;149(10):1033–9.
Namazi H, et al. Obturator to tibial nerve transfer via saphenous nerve graft for treatment of sacral plexus root avulsions: a cadaveric study. Orthop Traumatol Surg Res. 2020;106(2):291–5.
Namazi H, Haji Vandi S. Transfer of extensor digiti minimi and extensor carpi ulnaris nerve branches to the intrinsic motor nerve branches: A histological study on cadaver. Orthop Traumatol Surg Res. 2017;103(4):509–11.
Namazi H, HajiVandi S. Supinator to ulnar nerve transfer via in situ anterior interosseous nerve bridge to restore intrinsic muscle function in combined proximal median and ulnar nerve injury: a novel cadaveric study. J Surg Res. 2017;211:95–9.
Ahmad I, Akhtar M. Use of vein conduit and isolated nerve graft in peripheral nerve repair: a comparative study. Plastic Surg Int. 2014;2014:587968.
Foroutan KS, et al. Bone marrow mesenchymal stem cell and vein conduit on sciatic nerve repair in rats. Trauma monthly. 2015;20(1):e23325.
Sabongi RG, Fernandes M, dos Santos JBG. Peripheral nerve regeneration with conduits: use of vein tubes. Neural Regen Res. 2015;10(4):529.
Bonnel F, Foucher G, Saint-Andre J-M. Histologic structure of the palmar digital nerves of the hand and its application to nerve grafting. J Hand Surg. 1989;14(5):874–81.
Hudson AR, et al. Histological studies of experimental interfascicular graft repairs. J Neurosurg. 1979;51(3):333–40.
McFarlane RM, Mayer JR. Digital nerve grafts with the lateral antebrachial cutaneous nerve. J Hand Surg. 1976;1(3):169–73.
Pilanci O, et al. Is there a profit to use the lateral antebrachial cutaneous nerve as a graft source in digital nerve reconstruction? Microsurgery. 2014;34(5):367–71.
Schonauer F, et al. Digital nerve reconstruction by multiple Y-shaped nerve grafts at the metacarpophalangeal joint level. J Plast Reconstr Aesthet Surg. 2008;61(11):e13–6.
Unal MB, et al. Lateral antebrachial cutaneous nerve as a donor source for digital nerve grafting: a concept revisited. Open Orthop J. 2017;11:1041–8.
Namazi H, et al. Simvastatin vs. L-Carnitine: An experimental study on optimizing nerve repair. Turk Neurosurg. 2019;29(5):710–7.
Chevrollier J, et al. Evaluation of emergency nerve grafting for proper palmar digital nerve defects: a retrospective single centre study. Orthop Traumatol Surg Res. 2014;100(6):605–10.
Acknowledgements
We thank the Vice Chancellor of Research, Shiraz University of Medical Sciences, for the financial support of this work (Grant No. 1396-01-01-15682). The present article was extracted from the thesis written by Sobhani (MD) and has been accomplished in collaboration with Bone and Joint Diseases Research Center.
Funding
The present research was based on the thesis belonging to Ahmad Sobhani (Grant #1396-01-01-15682 from Shiraz University of Medical Sciences).
Author information
Authors and Affiliations
Contributions
Hamid Namazi: conceptualization, project administration, methodology, visualization, supervision, and investigation. Ahmad Sobhani: formal analysis, data curation, methodology, and writing original draft preparation. Saeed Gholamzadeh: methodology, visualization, and investigation. Amirreza Dehghanian: methodology, data curation, visualization, validation, and investigation. Fatemeh Dehghani Nazhvani: formal analysis, data curation, writing original draft, and writing, reviewing, and editing. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Research Ethics Committee of Shiraz University of Medical Sciences (#1396-01-01-15682).
Consent for publication
Not applicable.
Competing interests
The authors declare no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Namazi, H., Sobhani, A., Gholamzadeh, S. et al. Donor nerve graft assessment for covering thumb nerve defects: a cadaveric study. J Orthop Surg Res 15, 456 (2020). https://doi.org/10.1186/s13018-020-01974-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-020-01974-2