
Abstract
Background
There were several reports describing the biomechanics and microstructure of multifidus muscles in patients with lumbar disc herniation. However, correlations between lumbar multifidus muscle atrophy (LMA), spinopelvic parameters, and severity of adult degenerative scoliosis (ADS) have not been investigated. The study evaluated the impact of LMA and spinopelvic parameters on the severity of ADS.
Methods
One hundred and thirty-two patients with ADS were retrospectively reviewed. Standing whole-spine X-ray was used to evaluate the coronal (coronal Cobb angle, CA; coronal vertical axis, CVA) and sagittal (sagittal vertical axis, SVA; thoracic kyphosis, TK; lumbar lordosis, LL; pelvic incidence, PI; pelvic tilt, PT; sacral slope, SS) parameters. LMA was evaluated on axial T2-weighted magnetic resonance imaging (MRI) at intervertebral levels above and below the vertebra at the apex of the scoliotic curve. Clinical symptoms were evaluated by the Oswestry Disability Index (ODI) and the Japanese Orthopaedic Association (JOA) score. Multiple linear regression was used to assess correlations between LMA, spinopelvic parameters, and severity of scoliosis.
Results
LL and PT were negatively correlated with CA (P < 0.001); LL was positively correlated with SVA (P < 0.001). PI was positively correlated with CA (P < 0.001) and CVA (P < 0.001). PT (P < 0.001) and SS (P < 0.001) were negatively correlated with CVA. SS was negatively correlated with SVA (P < 0.001). Concave LMA at the upper or lower intervertebral level of the apical vertebra was positively correlated with CA (P ≤ 0.001); convex LMA at the upper or lower intervertebral level was negatively correlated with CA (P < 0.001). Convex LMA at the upper intervertebral level and concave LMA at the lower intervertebral level of the apical vertebra were negatively correlated with the SVA (P ≤ 0.001). At the upper intervertebral level, LMA on the concave side was positively correlated with CVA (P = 0.028); LMA on the convex side was negatively correlated with CVA (P = 0.012). PI was positively correlated with ODI (P < 0.001); PT (P < 0.001) and SS (P < 0.001) were negatively correlated with ODI. At the lower intervertebral level, LMA on the concave side was positively correlated with ODI (P = 0.038); LMA on the convex side was negatively correlated with ODI (P = 0.011). PI was positively correlated with JOA (P < 0.001); PT (P < 0.001) and SS (P < 0.001) were negatively correlated with JOA.
Conclusions
Spinopelvic parameters are correlated with the severity of ADS. Asymmetric LMA at both upper and lower intervertebral levels of the apical vertebra is positively correlated with CA. LMA on the diagonal through the apical vertebra is very important to maintain sagittal imbalance via parallelogram effect. LMA at lower intervertebral levels of the apical vertebra may have a predictive effect on ODI. JOA score seems to be more correlated with spinopelvic parameters than LMA.
Similar content being viewed by others


Background
Adult degenerative lumbar scoliosis (ADS) is defined as spinal deformity with a coronal deviation of greater than 10° in a skeletally mature patient, especially older than 40 years, without a history of scoliosis in childhood or adolescence [1]. The prevalence of ADS rises with age, with estimates ranging from 6 to 68%; therefore, it is becoming a major public health concern as the global incidence is increasing with the aging population [2, 3].
There were several reports describing the biomechanics and microstructure of multifidus muscles in patients with lumbar disc herniation [4]. Results showed correlations between lumbar multifidus muscle atrophy (LMA) and chronic low back pain, disc degeneration, and radiculopathy [5, 6]. However, correlations between LMA, spinopelvic parameters, and severity of ADS have not been investigated. Yagi et al. [7] reported that the cross-sectional area (CSA) of the multifidus (MF) and psoas (PS) were significantly smaller in degenerative lumbar scoliosis (DLS) patients. However, their muscle CSA analysis only included the L5-S1 level, which could not reflect the characteristics of paravertebral muscles around the apex vertebra. Our study simplified the approach to assessing LMA by using Goutallier Classification system [8]; LMA on the convex and concave sides of the scoliotic curve was measured on axial T2-weighted MR images at intervertebral levels above and below the apical vertebras. All of them would make the results more applicable.
The purpose of this study was to evaluate the correlation between LMA, spinopelvic parameters, and the severity of ADS and identify variables that predict progression in ADS. To our knowledge, this has not been previously reported.
Methods
Selection criteria
Patients with ADS that attended our inpatient clinic during the period from January 2016 to December 2017 were eligible for study. Inclusion criteria were age > 40 years at the time of attendance, medical records containing anteroposterior and lateral X-ray radiographs of total spine and magnetic resonance imaging (MRI) of the lumbar spine, and Cobb angle of lumbar curve in the coronal plane > 10° on a standing posteroanterior film. Exclusion criteria were history of scoliosis in childhood or adolescence, history of spinal surgery, local infection, inflammation around the spine, history of severe spinal trauma, spinal tumor, and presence of other systemic diseases that can affect spinal alignment (e.g., muscular dystrophy, ankylosing spondylitis, Parkinson disease). All patients included in our study provided written informed consent. This study has been approved by the institutional review board following the Declaration of Helsinki principles.
Evaluation of muscles in MRIs
In this study, 1.5 imaging system (Magnetom Symphony; Siemens, Berlin, Germany) for MRIs was used, and three T2-weighted axial images at intervertebral levels above and below the apical vertebras were obtained. The slices were separated by a 0.1-mm gap and were 4 mm thick; multifidus muscles on the convex and concave sides of the scoliotic curve were analyzed from the center slice of each of the three T2-weighted axial images. Muscle atrophy was known to be related to increased fatty infiltration; therefore, the Goutallier Classification system [8] was used to quantify muscle fatty degeneration in the lumbar multifidus muscle (Fig. 1).

Goutallier grades (range, 0 to 4) on axial T2W1 MRI are represented by a to e: grade 0, normal muscle tissue (a); grade 1, fat streaks (b); grade 2, more muscle than fat (c); grade 3, equal amounts of fat and muscle tissue (d); and grade 4, more fat than muscle (e)
Radiographic measurement and analysis
Standing whole-spine X-ray (Philips Digital Diagnost; Zhejiang Province, China) was used to evaluate the patients (Fig. 2). All radiologic parameters were measured twice at 1-month intervals by two researchers who were not involved in the patient encounters.

Radiological parameter measurement methods. a The coronal Cobb angle (CA) is measured from the superior end plate of the cephalad end vertebra and the inferior end plate of the caudal end vertebra on the coronal plane; the coronal vertical axis (CVA) is defined as the distance from a perpendicular line drawn from the superior end plate of S1 vertebral body to the C7 plumb line on the coronal plane. b The sagittal vertical axis (SVA) is defined as the distance from a perpendicular line drawn from the superior end plate of S1 vertebral body to the C7 plumb line on lateral radiographs; the thoracic kyphosis (TK) is measured from the upper end plate of T2 to the lower end plate of T12; the lumbar lordosis (LL) is measured from the upper end plate of T12 to the upper end plate of S1; the sacral slope (SS) is defined as the angle between the cranial sacral end plate and a horizontal line; the pelvic incidence (PI) is defined as the angle subtend by a line connecting the center of the femoral head to the center of the cephalad end plate of S1 and a perpendicular line from the upper end plate of S1; the pelvic tilt (PT) is measured as the angle between the vertical axis and the line through the midpoint of the sacral end plate to femoral heads axis
Clinical assessment
Demographic data, including patients’ age and sex, were recorded. Clinical symptoms were evaluated by the Oswestry Disability Index (ODI) and the Japanese Orthopaedic Association (JOA) score. All of them were valid and rigorous functional measures used for assessing ADS.
Statistical analysis
Statistical analyses were performed using Statistical Package for the Social Sciences version 17.0 software (SPSS, Inc., Chicago, IL). Non-contiguous data was presented as number or ratio, whereas continuous variables were reported as mean ± standard deviations (SD). Shapiro-Wilk test was used to test for normality. Wilcoxon rank-sum test was used to compare the differences in LMA between the concave and convex sides at intervertebral levels above and below the apical vertebras, or between upper intervertebral levels and lower intervertebral levels of the apical vertebras in concave or convex sides. Pearson’s correlation test was used to analyze the correlation between different parameters. Multiple linear regression was used to assess correlations between LMA, spinopelvic parameters, and severity of scoliosis. Statistical significance was set at P < 0.05.
Results
Patient demographics
This study included 132 ADS patients (42 males, 90 females) with a mean age of 61.5 ± 7.2 years (Table 1). Scoliotic curves typically had an apex at L3 (42.4%) and were convex to the left (58.3%). Mean CA was 25.4 ± 1.0°, TK was 31.2 ± 12.5°, LL was 29.7 ± 12.5°, PI was 53.4 ± 8.0°, PT was 29.2 ± 7.3°, and SS was 27.3 ± 7.5°. There was a wide range of severity of sagittal imbalance in these patients with a mean value of 8.9 ± 10.0 cm.
Comparison of LMA between different intervertebral levels or sides
The Goutallier Classification system showed the following: at the upper intervertebral level, LMA (upper LMA, U-LMA) significantly increased on the concave side compared with the convex side (convex vs. concave, Z = − 7.616, P < 0.001); at the lower intervertebral level, LMA (lower LMA, L-LMA) similarly increased on the concave side compared with the convex side (convex vs. concave, Z = − 2.345, P = 0.019); on the concave side, no significant difference was found in between U-LMA and L-LMA (lower vs. upper, Z = − 0.093, P = 0.926); and on the convex side, U-LMA was significantly increased compared with L-LMA (lower vs. upper, Z = − 7.049, P < 0.001; Table 2; Fig. 3).

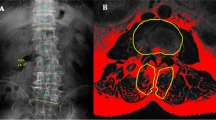
A 58-year-old female patient with adult degenerative scoliosis (ADS). a Standing anteroposterior (AP) and lateral radiographs. Coronal Cobb angle (CA), 35.6°; coronal vertical axis (CVA), − 1.6 cm; sagittal vertical axis (SVA), + 4.8 cm; thoracic kyphosis (TK), 9.2°; lumbar lordosis (LL), 28.1°; pelvic incidence (PI), 62.6°; pelvic tilt (PT), 35.2°; sacral slope (SS), 27.4°. b T2-weighted axial image at intervertebral levels above the apical vertebra (T12/L1): grade 1 LMA on the convex side and grade 4 LMA on the concave side. c T2-weighted axial images at the intervertebral level below the apical vertebra (L1/2): grade 2 LMA on the convex side and grade 3 LMA on the concave side
Correlation of spinopelvic parameters and LMA
Pearson correlation analysis showed a positive correlation between SS and LL (coefficient = 0.900, P < 0.001); LL and U-LMA on the concave side (coefficient = 0.212, P = 0.015); PI and LL (coefficient = 0.621, P < 0.001); PI and SS (coefficient = 0.758, P < 0.001); PI and L-LMA on the concave side (coefficient = 0.218, P = 0.012); PT and L-LMA on the concave side (coefficient = 0.442, P < 0.001); PT and L-LMA on the convex side (coefficient = 0.406, P < 0.001); U-LMA on the concave side and convex side (coefficient = 0.718, P < 0.001); U-LMA on the concave side and L-LMA on the concave side and on the convex side (coefficient = 0.385, P < 0.001; coefficient = 0.505, P < 0.001, respectively); U-LMA on the convex side and L-LMA on the concave side and the convex side (coefficient = 0.628, P < 0.001; coefficient = 0.502, P < 0.001, respectively); L-LMA on the concave side and L-LMA on the convex side (coefficient = 0.668, P < 0.001; Table 3). There were negative correlations between PT and LL and SS (coefficient = − 0.561, P < 0.001; coefficient = − 0.575, P < 0.001, respectively). Therefore, pelvic parameters and LMA in different positions were taken into multiple linear regression analysis.
Correlation of influencing factors and severity of ADS
Multiple linear regression (R2 = 0.705) of spinal pelvic parameters and CA showed there was a positive correlation between PI and CA (B = 1.519, P < 0.001); the correlations between PT (B = − 0.335, P < 0.001), LL (B = − 0.558, P < 0.001), and CA were negative (Table 4). On the concave side, both U-LMA (B = 4.266, P = 0.001) and L-LMA (B = 13.343, P < 0.001) were positively correlated with CA; on the convex side, both U-LMA (B = − 8.123, P < 0.001) and L-LMA (B = − 4.272, P < 0.001) were negatively correlated with CA; R2 value of this model was 0.500 (Table 4). Table 5, which summarizes the correlation between spinal pelvic parameters, L-LMA, or U-LMA on concave or convex side and SVA, shows that LL was positively correlated with SVA (B = 0.342, P < 0.001) and SS was negatively correlated with SVA (B = − 0.751, P < 0.001); because R2 value was 0.129, this model made little meaning; there were negative correlations between U-LMA on the convex side (B = − 8.123, P < 0.001), L-LMA (B = − 4.198, P = 0.001) on the concave side, and SVA (R2 = 0.319); R2 value of this model indicated a poor predictive power. Multiple linear regression analysis (R2 = 0.764; Table 6) of spinal pelvic parameters and CVA revealed that PI was positively correlated with CVA (B = 0.271, P < 0.001); PT (B = − 0.237, P < 0.001) and SS (B = − 0.182, P < 0.001) were negatively correlated with CVA. At the upper intervertebral level, LMA on the concave side was positively correlated with CVA (B = 0.364, P = 0.028); LMA on the convex side was negatively correlated with CVA (B = − 0.296, P = 0.012); considering the R2 value was 0.050, the meaning of this multiple linear regression model was limited (Table 6). Multiple linear regression (R2 = 0.680) of spinal pelvic parameters and ODI showed PI was positively correlated with ODI (B = 0.407, P < 0.001); PT (B = − 0.229, P < 0.001) and SS (B = − 0.466, P < 0.001) were negatively correlated with ODI (Table 7). At the lower intervertebral level, LMA on the concave side was positively correlated with ODI (B = 0.735, P = 0.038); LMA on the convex side was negatively correlated with ODI (B = − 0.668, P = 0.011); however, this multiple linear regression model made little sense (R2 = 0.051; Table 7). PI was positively correlated with JOA (B = 0.192, P < 0.001); PT (B = − 0.119, P < 0.001) and SS (B = − 0.213, P < 0.001) were negatively correlated with JOA; R2 value of this model was 0.687 (Table 8). Duration of disease was positively correlated with SVA (B = 0.138, P < 0.001, R2 = 0.111) and negatively correlated with CA (B = − 0.086, P = 0.017, R2 = 0.043); no significant correlation was found between duration of disease and CVA (P = 0.838), ODI (P = 0.352), and JOA (P = 0.121). Considering the R2 value of this model was very low, duration of disease was not a good predictor of the severity of ADS.
Discussion
The multifidus muscle is the most medially located back muscle; it is also the largest muscle, which spans the lumbosacral junction; in addition, it contributes to maintaining the erector posture of the trunk and to rotating and abducting the trunk [9]. Degeneration of soft tissue structures occurs in adult spinal degenerative disease [10]. Consequently, LMA may result in instability of the spine and exacerbate disc and facet degeneration in the lumbar spine [11]. Paraspinal muscle plays a more important role in maintaining the stability of L3–L4 segment than others [12]. This may explain why the apical vertebras of ADS patients most commonly occurred in L3 or L4 segment.
Hypotheses describing the mechanisms of LMA include disuse, denervation, inflammation, and injury [13,14,15,16]. In ADS patients, disuse and immobilization of the back muscles are common; these changes may cause atrophy at different intervertebral levels; furthermore, paraspinal denervation and re-innervation are common in disc herniation or nerve root compression [17]. Considering multifidus muscle is innervated by the dorsal root of the lumbar spinal nerve, atrophy of multifidus muscle innervated by medial branch of the dorsal ramus of the lumbar nerve root would occur when the nerve root is compressed by herniated mass [18]. Sun et al. [17] stated that as there was no denervation phenomenon at the L3–L4 level, LMA could be the cause of disc degeneration; at the L5–S1 level, however, LMA could also be the consequence of L4–L5 disc herniation; pathogenetic mechanisms of U-LMA and L-LMA were different. Similarly, our study showed that LMA on the concave side was more severe than that on the convex side; on the convex side, there were differences in the causes of U-LMA and L-LMA. These indicated that the method, in which the axial image obtained at the level of the apex of the curvature was used as a reference for comparison to minimize the effect of the deformity on the morphometry of the paraspinal muscle, in the previous study might not be proper [19]. U-LMA may be the cause of ADS, while L-LMA may be the consequence of ADS. The positional change of the morphometry of paraspinal muscles will be influenced by the difference in the length of the arc in both sides of scoliosis; this is positively related to the radius of the arc; in addition, it is also proportional to their distance from the center of the axis of the spine. The CSA of paraspinal muscles can sometimes show discordant patterns of differences; the possible explanation is that the paraspinal muscles far from the axis of the spinal column will show the obvious effect of the positional change more than others that are closer to the axis of the spine; however, the influence of positional change on multifidus muscles may be caused by the change in the muscle itself, including the atrophy on the concave side or hypertrophy on the convex side [5, 19]. Therefore, patients in supine position during the MRI examination will not influence the evaluation of LMA.
Results of Pearson correlation analysis of spinopelvic parameters and LMA in our study showed that there were correlations among LL, SS, PI, and PT without TK. This is because spinopelvic parameters are geometrically related, such that PI is equal to the sum of SS and PT; variations in the lower arc of lordosis are determined by the sacral slope; when the sacral slope increases, the lower arc of lordosis increases, then the global curvature of lordosis increases as well; thoracic segments are supported by ribs with relatively poor compensatory ability; therefore, the correlation between TK and other radiographic parameters is not significant [20]. Acting like a bowstring, the multifidus muscle could switch compression loading to stretch loading and transmit some of the axial compression force on the disc to the anterior longitudinal ligament, then maintains the spinopelvic parameters [21]. However, our study showed that L-LMA on both concave and convex sides were positively correlated with PT; U-LMA on the concave side was positively correlated with LL; L-LMA on the concave side was positively correlated with PI. These revealed that when the ADS occurred, bowstring effect of multifidus muscle would be influenced by multiple complex factors; the status of multifidus muscle on the concave side would play more important roles in maintaining spinopelvic parameters than others.
A high pelvic incidence is associated with long, curved lumbar lordosis; this reciprocal association is an important component of overall sagittal alignment [22]. It was reported that lumbar hypolordosis was associated with lateral listhesis, vertebral rotation in ADS patients, which would aggravate scoliosis [23]. Therefore, in our study, LL and PT are both protective factors of CA; LL was positively correlated with SVA. PI reflects compensatory ability of the lumbar spine and pelvis in maintaining global alignment of the spine. In patients with high PI, the occurrence of ADS may mean a more severe decompensated state than others. In consequence, PI was positively correlated with CA and CVA in our study [24]. A previous study reported that there was a correlation between an anterior shift in the C7 plumb line and a vertically oriented sacrum [25]. In addition, the sacral slope was positional parameters that can be affected by changes in the alignment of the lower extremities, which would also influence CVA [26]. Therefore, SS was negatively correlated with SVA in our study.
The correlations of LMA at different intervertebral levels and severity of ADS were analyzed in our study. Results showed that U-LMA and L-LMA on the concave side were positively correlated with CA; U-LMA and L-LMA on the convex side were negatively correlated with CA. Yagi et al. [7] suggested that ADS patients did not have an age-related, progressive global muscle weakness, but rather a localized myopathy, which was commonly seen in patients with dropped head syndrome. Significant asymmetric LMA may be the primary cause of ADS and could be used to predict the progression of ADS. Convex U-LMA and concave L-LMA were negatively correlated with the SVA. This indicated that LMA on the diagonal through the apical vertebra would balance the stress and secure the stress conduction via parallelogram effect, which was very important to maintain sagittal imbalance. This parallelogram effect is first proposed in this study. Considering sagittal imbalance has a more disastrous influence on the clinical outcome than coronal imbalance in ADS patients, the significance of CVA may be limited [24]. R2 value of multiple linear regression analysis of LMA and CVA was very low in our study, which indicated that LMA could not accurately predict CVA. This might be explained by the effects of various factors on CVA [27].
Schwab et al. [28] reported that no significant correlation was found between adult scoliosis and nutritional status or VAS scores in elderly patients. Similarly, our results showed that none of the parameters were correlated with VAS score. Therefore, VAS score would not be an effective method to measure the severity of ADS. In our study, PI was positively correlated with ODI; however, PT and SS were negatively correlated with ODI. Mac-Thiong et al. [29] found that sagittal spinal balance was strongly correlated with ODI in ADS; however, coronal spinal balance did not influence the ODI in their study. Therefore, influencing factors of SVA and ODI may be overlapping. Results in our study showed, at the lower intervertebral level, LMA on the concave side was positively correlated with ODI; in contrast, LMA on the convex side of ODI was negatively correlated with ODI. These indicated LMA at the lower intervertebral level would have a predictive effect on ODI in ADS patients. Compared with ODI, JOA scores are more focused on evaluating neurologic functions [30]. It was reported that worse sagittal spinopelvic alignment was the main cause of functional loss in ADS patients [20]. Therefore, JOA score seemed to be more correlated with spinopelvic parameters than LMA in our study.
There are several limitations associated with our study. First, this is a retrospective cross-sectional study that may result in unavoidable selection bias. Secondly, this is a single-center study and sample size is thus limited. Third, a comparative analysis of different phases of ADS was not conducted as the course ADS is difficult to follow. Studies with a larger sample size that include patients at different stages of disease progression are warranted to confirm the results of the present study.
Conclusion
In ADS patients, LMA on the concave side is more severe than the convex side; on the convex side, there are differences in the causes of U-LMA and L-LMA. LL and PT are both protective factors of CA progression; high LL is a risk of sagittal imbalance. High SS is a protective factor of sagittal imbalance. Asymmetric LMA may be positively correlated with CA. LMA on the diagonal through the apical vertebra may be very important to maintain sagittal imbalance via parallelogram effect. In addition, LMA at lower intervertebral levels of the apical vertebra may have a predictive effect on ODI. JOA score seems to be more correlated with spinopelvic parameters than LMA.
Availability of data and materials
Please contact the author for data requests.
Abbreviations
- ADS:
-
Adult degenerative scoliosis
- CA:
-
Coronal Cobb angle
- CSA:
-
Cross-sectional area
- DLS:
-
Degenerative lumbar scoliosis
- LL:
-
Lumbar lordosis
- L-LMA:
-
Lower intervertebral level LMA
- LMA:
-
Lumbar multifidus muscle atrophy
- MF:
-
Multifidus
- MRI:
-
Magnetic resonance imaging
- PI:
-
Pelvic incidence
- PS:
-
Psoas
- PT:
-
Pelvic tilt
- SD:
-
Standard deviations
- SS:
-
Sacral slope
- SVA:
-
Sagittal vertical axis
- TK:
-
Thoracic kyphosis
- U-LMA:
-
Upper intervertebral level LMA
References
Schwab FJ, Smith VA, Biserni M, et al. Adult scoliosis: a quantitative radiographic and clinical analysis. Spine (Phila Pa 1976). 2002;27(4):387–92.
Jimbo S, Kobayashi T, Aono K, et al. Epidemiology of degenerative lumbar scoliosis: a community-based cohort study. Spine (Phila Pa 1976). 2012;37(20):1763–70. https://doi.org/10.1097/BRS.0b013e3182575eaa.
Yang C, Yang M, Chen Y, et al. Radiographic parameters in adult degenerative scoliosis and different parameters between sagittal balanced and imbalanced ADS patients. Medicine (Baltimore). 2015;94(29):e1198. https://doi.org/10.1097/MD.0000000000001198.
Yoshihara K, Shirai Y, Nakayama Y, et al. Histochemical changes in the multifidus muscle in patients with lumbar intervertebral disc herniation. Spine (Phila Pa 1976). 2011;26(6):622–6.
Freeman MD, Woodham MA, Woodham AW. The role of the lumbar multifidus in chronic low back pain: a review. PM R. 2010;2(2):142–6, 1-167. https://doi.org/10.1016/j.pmrj.2009.11.006.
Lee JC, Cha JG, Kim Y, et al. Quantitative analysis of back muscle degeneration in the patients with the degenerative lumbar flat back using a digital image analysis: comparison with the normal controls. Spine (Phila Pa 1976). 2008;33(3):318–25. https://doi.org/10.1097/BRS.0b013e318162458f.
Yagi M, Hosogane N, Watanabe K, et al. The paravertebral muscle and psoas for the maintenance of global spinal alignment in patient with degenerative lumbar scoliosis. Spine J. 2016;16(4):451–8. https://doi.org/10.1016/j.spinee.2015.07.001.
Battaglia PJ, Maeda Y, Welk A, et al. Reliability of the Goutallier classification in quantifying muscle fatty degeneration in the lumbar multifidus using magnetic resonance imaging. J Manip Physiol Ther. 2014;37(3):190–7. https://doi.org/10.1016/j.jmpt.2013.12.010.
Macintosh JE, Valencia F, Bogduk N, et al. The morphology of the human lumbar multifidus. Clin Biomech (Bristol, Avon). 1986;1(4):196–204. https://doi.org/10.1016/0268-0033(86)90146-4.
Wong E, Altaf F, Oh LJ, et al. Adult degenerative lumbar scoliosis. Orthopedics. 2017;40(6):e930–9. https://doi.org/10.3928/01477447-20170606-02.
Hodges P, Holm AK, Hansson T, et al. Rapid atrophy of the lumbar multifidus follows experimental disc or nerve root injury. Spine (Phila Pa 1976). 2006;31(25):2926–33. https://doi.org/10.1097/01.brs.0000248453.51165.0b.
Richardson CA, Jull GA. Muscle control-pain control. What exercises would you prescribe? Man Ther. 1995;1(1):2–10. https://doi.org/10.1054/math.1995.0243.
Bakou S, Cherel Y, Gabinaud B, et al. Type-specific changes in fibre size and satellite cell activation following muscle denervation in two strains of turkey (Meleagris gallopavo). J Anat. 1996;188(Pt 3):677–91.
Bishop DL, Milton RL. The effects of denervation location on fiber type mix in self-reinnervated mouse soleus muscles. Exp Neurol. 1997;147(1):151–8. https://doi.org/10.1006/exnr.1997.6605.
Herbison GJ, Jaweed MM, Ditunno JF. Muscle atrophy in rats following denervation, casting, inflammation, and tenotomy. Arch Phys Med Rehabil. 1979;60(9):401–4.
Weber BR, Grob D, Dvorak J, et al. Posterior surgical approach to the lumbar spine and its effect on the multifidus muscle. Spine (Phila Pa 1976). 1997;22(15):1765–72.
Sun D, Liu P, Cheng J, et al. Correlation between intervertebral disc degeneration, paraspinal muscle atrophy, and lumbar facet joints degeneration in patients with lumbar disc herniation. BMC Musculoskelet Disord. 2017;18(1):167. https://doi.org/10.1186/s12891-017-1522-4.
Macintosh JE, Bogduk N. The biomechanics of the lumbar multifidus. Clin Biomech (Bristol, Avon). 1989;1(4):205–13. https://doi.org/10.1016/0268-0033(86)90147-6.
Kim H, Lee CK, Yeom JS, et al. Asymmetry of the cross-sectional area of paravertebral and psoas muscle in patients with degenerative scoliosis. Eur Spine J. 2013;22(6):1332–8. https://doi.org/10.1007/s00586-013-2740-6.
Fu X, Sun XL, Harris JA, et al. Long fusion correction of degenerative adult spinal deformity and the selection of the upper or lower thoracic region as the site of proximal instrumentation: a systematic review and meta-analysis. BMJ Open. 2016;6(11):e12103. https://doi.org/10.1136/bmjopen-2016-012103.
Kader DF, Wardlaw D, Smith FW. Correlation between the MRI changes in the lumbar multifidus muscles and leg pain. Clin Radiol. 2000;55(2):145–9. https://doi.org/10.1053/crad.1999.0340.
Weisz G, Houang M. Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine (Phila Pa 1976). 2005;30(13):1558–9 1559.
Hong JY, Suh SW, Modi HN, et al. The prevalence and radiological findings in 1347 elderly patients with scoliosis. J Bone Joint Surg Br. 2010;92(7):980–3. https://doi.org/10.1302/0301-620X.92B7.23331.
Cho KJ, Suk SI, Park SR, et al. Risk factors of sagittal decompensation after long posterior instrumentation and fusion for degenerative lumbar scoliosis. Spine (Phila Pa 1976). 2010;35(17):1595–601. https://doi.org/10.1097/BRS.0b013e3181bdad89.
Kumar MN, Baklanov A, Chopin D. Correlation between sagittal plane changes and adjacent segment degeneration following lumbar spine fusion. Eur Spine J. 2001;10(4):314–9.
Roussouly P, Gollogly S, Berthonnaud E, et al. Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine (Phila Pa 1976). 2015;30(3):346–53.
Hawasli AH, Chang J, Yarbrough CK, et al. Interpedicular height as a predictor of radicular pain in adult degenerative scoliosis. Spine J. 2016;16(9):1070–8. https://doi.org/10.1016/j.spinee.2016.04.017.
Schwab F, Dubey A, Gamez L, et al. Adult scoliosis: prevalence, SF-36, and nutritional parameters in an elderly volunteer population. Spine (Phila Pa 1976). 2005;30(9):1082–5.
Mac-Thiong JM, Transfeldt EE, Mehbod AA, et al. Can c7 plumbline and gravity line predict health related quality of life in adult scoliosis? Spine (Phila Pa 1976). 2009;34(15):E519–27. https://doi.org/10.1097/BRS.0b013e3181a9c7ad.
Masuda K, Higashi T, Yamada K, et al. The surgical outcome of decompression alone versus decompression with limited fusion for degenerative lumbar scoliosis. J Neurosurg Spine. 2018:1–6. https://doi.org/10.3171/2018.1.SPINE17879.
Acknowledgements
This research was performed mainly at the Department of Orthopaedics of Xuanwu Hospital Capital Medical University and in the National Clinical Research Center for Geriatric Diseases.
Funding
This study was funded by the National Natural Science Foundation of China (No. 81672201, No. 81871794) and Beijing Municipal Commission of Health and Family Planning (No. PXM2017 026283 000002).
Author information
Authors and Affiliations
Contributions
XYS, TTZ, and SBL designed the study and composed the data. MCG and JZD carried out the study and collected the crucial background information. WW collected the data. CK analyzed the data. SYS interpreted the data and did the figure editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study has been approved by the Ethics Committee of the Xuanwu Hospital Capital Medical University, and the approval number is Clinical study review [2018] 014. Written informed consent was obtained from each patient prior to the study.
Consent for publication
All patients included in the study provided their informed consent at enrolment on the use of patients’ data for research.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Sun, XY., Kong, C., Zhang, TT. et al. Correlation between multifidus muscle atrophy, spinopelvic parameters, and severity of deformity in patients with adult degenerative scoliosis: the parallelogram effect of LMA on the diagonal through the apical vertebra. J Orthop Surg Res 14, 276 (2019). https://doi.org/10.1186/s13018-019-1323-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-019-1323-6