
Abstract
Background
We aimed to explore the efficacy of orbital radiotherapy (RT) in patients with moderate-to-severe active Graves’ orbitopathy (GO), including long-lasting disease, and to determine the predictive factors associated with treatment response.
Methods
This was a retrospective study of 62 moderate-to-severe active GO patients treated with RT. Demographic data and ophthalmic findings prior to RT and at 3 and 6 months afterward were analyzed. Computed tomography was performed before and after RT to compare orbital volume change. We used logistic regression to determine the predictive factors for treatment response. Subjects were divided into early- and late-active phase groups based on GO duration of 24 months and treatment outcomes were compared with each other to observe the effects of RT timing on treatment response.
Results
Forty (64.5%) and forty-six (74.1%) patients experienced improvements in GO at 3 and 6 months after radiotherapy, respectively. Ocular parameters such as clinical activity score (CAS), proptosis, extraocular muscle (EOM) limitation, and compressive optic neuropathy (CON) were improved by RT. Volumes of EOM significantly decreased after RT. The enlargement of EOMs and EOM limitation were predictive factors for a good response to RT. At 6 months after RT, 22 (68.8%) patients of late-active phase group exhibited improvement in GO, which is comparable to the number of 24 (80.0%) patients of early-active phase group. In the late-active phase group, CAS, diplopia, and visual acuity were improved significantly, but there was no change in EOM limitation.
Conclusions
In moderate-to-severe active GO patients, orbital RT may help improve high CAS, proptosis, EOM limitation, and CON. The orbital RT in long-lasting active GO patients may be considered as treatments for the relief of symptoms including high CAS and poor visual acuity.
Similar content being viewed by others


Background
Graves’ orbitopathy (GO) is an autoimmune disorder of the orbit, accompanied by a complex of ocular symptoms. It is the most common extrathyroidal manifestation of Graves’ disease (GD) and is associated with hyperthyroidism in 90% of cases [1]. GO primarily involves inflammatory changes in orbital tissues with potential thickening and fibrosis of the extraocular muscles (EOM) and orbital fat, increasing the volume within bony orbit [2]. The development of GO is characterized by progressive deterioration accompanying active symptoms, followed by a plateau, then gradual improvement toward the baseline [3]. Progressive deterioration is caused by an autoimmune process and characterized by lymphocyte infiltration, cytokine secretion, and fibroblast proliferation. In this active inflammatory phase, mainstay treatment includes systemic glucocorticoid therapy and orbital radiotherapy (RT) [4]. High-dose intravenous (IV) glucocorticoid is the first-line treatment for moderate-to-severe active GO patients, with studies reporting varying success rates from 54.3 to 77% [5,6,7], but relapse is frequent when they are withdrawn or tapered.
Orbital RT is used to improve symptoms during the progressive deterioration phase in GO patients and is particularly useful in treating those who are not sensitive to or tolerant of glucocorticoid therapy, or who have relapsing symptoms after glucocorticoid therapy [8]. Orbital RT is slower to show a therapeutic effect than glucocorticoid therapy but can be effective for a longer period [9]. Several retrospective studies have reported on the efficacy of orbital RT [10, 11], but prospective studies have yielded inconsistent results [12,13,14]. In randomized clinical trials, orbital RT was a safe treatment, but efficacy of RT was limited. The available data suggest particularly effective in EOM involvement, especially when it is of recent onset [15]. Since recent-onset active GO is much more treatable than longstanding or inactive disease, only certain patients can be expected to experience successful outcomes of orbital RT. Signs of inflammation, recent-onset eye muscle dysfunction, and optic neuropathy respond well to orbital RT, while proptosis and longstanding eye muscle restriction respond poorly [16]. However, the progression of GO varies among individual patients, so active GO is not always obvious in the early stages and is sometimes observed in long-lasting GO. There has been no study of orbital RT efficacy in long-lasting active GO.
We, therefore, aimed to evaluate the efficacy of orbital RT in patients with moderate-to-severe active GO including long-lasting disease and to determine factors that can predict treatment response.
Methods
This study was approved by the institutional review board, and the requirement of informed consent was waived considering its retrospective design. This study adheres to the guidelines of the Declaration of Helsinki. Research data are stored in an institutional repository and will be shared upon request to the corresponding author.
We reviewed the medical records of 62 consecutive GO patients treated with RT between December 2015 and December 2018. Patients who were diagnosed with moderate-to-severe active GO, treated with RT, and followed up for at least 6 months were included in this study. These patients were refractory to high-dose IV steroids or were not eligible for treatment with high-dose IV steroids. The activity and severity of GO were accessed according to the standardized criteria recommended by the European Group on Graves’ Orbitopathy (EUGOGO) [17]. Patients who underwent ophthalmic surgery within three months prior to RT, pregnant patients, patients under 20 or over 80 years old, and patients with a history of other eye diseases such as glaucoma, diabetic retinopathy, or maculopathy, were excluded. Information on age, sex, duration of GD and GO prior to RT, smoking, family history of GO, and treatment history was collected. Serum concentrations of thyroid stimulating hormone (TSH), free thyroxine (FT4), and thyroxine binding inhibitory immunoglobulin (TBII) were evaluated prior to RT.
Comprehensive ophthalmologic examinations including the degree of proptosis, margin reflex distance 1 (MRD1, the vertical distance between the center of the pupil and the center of the upper eyelid), palpebral fissure height (PFH, the vertical distance between the center of the lower eyelid to the center of the upper eyelid), intraocular pressure (IOP), diplopia, EOM movement, visual acuity (VA), existence of compressive optic neuropathy (CON), and clinical activity score (CAS) were carried out before RT and at 3 and 6 months afterward. The degree of proptosis was measured using a Hertel exophthalmometer (Oculus, Arlington, VA, US). MRD1 and PFH were measured using custom-made PC-based EAS software (Eyelid Analysis Software, Biomedical Research Institute, Seoul, Korea) using photographs taken in primary position [18]. Diplopia was evaluated based on Gorman score [19]. EOM movement was measured using the Light Reflex Method, where a score of 45° was given when the light reflex was at the limbus, 30° at halfway between the limbus and pupil edge, and 15° at the pupil edge. Improvement in the EOM movement was defined if the variation was at least 15°, as previously described [20]. VA measured using a Snellen chart was converted to the logarithm of the minimum angle of resolution (logMAR). CON was judged based on the presence of decreased VA, plus one or more of the following findings: relative afferent pupillary defect, color vision deficit, or visual field defect [21]. A modified CAS was assessed using a seven-point modified formulation [21]. When differences in scores or measures existed for the two eyes of one patient, data from the worse eye were considered for analysis. All ophthalmic examinations were performed by one specialist (J.K.L).
Computed tomography (CT) was performed before and again at 3–6 months after RT at convenience. Orbital CT scans were obtained with 1 mm sections. Volumetric measurements of EOM and orbital fat were carried out as per Regensburg et al. [22] The volumes of the superior rectus, inferior rectus, medical rectus, lateral rectus, and orbital fat were calculated with the use of manual segmentation of CT scans with the Eclipse treatment planning system (TPS) (ver. 13.7, Varian Medical Systems Inc., Palo Alto, CA, USA). The orbital soft tissue CT numbers referenced for volume measurements were set at − 200 to − 30 Hounsfield units (HU) for fat tissue and − 30 to + 100 HU for muscle tissue. Tissues of interest with the chosen CT number in all slices were delineated and reconstructed in three dimensions and tissue volumes were measured.
All patients were treated with retroorbital irradiation using a linear accelerator with a three-dimensional conformal technique. Patients were immobilized with a custom-made thermoplastic case, and CT scanning with a slice thickness of 2.5 mm without contrast was performed for image acquisition and target contouring. The clinical target volume (CTV) included the EOMs and retroorbital fat. The lenses, optic nerves and lacrimal glands were zoned as organs-at-risk. A 2 mm margin around the CTV was generated as the planning target volume. The planned irradiation dose was 24 Gy in 12 fractions, and treatment planning was carried out using Eclipse TPS. Irradiation was performed using a 6 MeV photon beam. Concurrent low-dose oral steroids of 20 mg prednisone daily were administered to patients with active high CAS score for 2 ~ 4 weeks.
Response to orbital RT was defined as an improvement in at least two of the following six parameters: 1) CAS improvement in at least two points, 2) reduced proptosis by at least 2 mm, 3) improvement in diplopia (lessening of Gorman score), 4) improvement in EOM movement, 5) improvement in VA, and 6) disappearance of CON.
To verify the effects of timing of orbital RT on the treatment response, the subjects were divided into two groups based on the GO symptom duration from onset. The timing of RT according to GO duration was classified as the early-active phase until 24 months, and after 24 months as the late-active phase. Orbital RT in the late-active phase was performed in patients who recently experienced a distinct deterioration of symptoms or patients resistant to long-term steroid treatment. Response to orbital RT was analyzed and symptoms improved after RT was identified in each group.
All statistical analyses were performed using R version 3.4.0. Data are expressed as mean ± SD or median (interquartile range) for continuous variables. Categorical variables were reported as sample numbers and percentages. Changes in ophthalmic findings before and after treatment were compared using a linear mixed effect model or a generalized linear mixed effect model to analyze a fixed-time effect by controlling for random effects. For ordinal response variables, repeated measures proportional odds logistic regression was used. Changes in orbital fat and EOM volumes were compared using paired t-tests. Changes in ophthalmic findings according to the treatment phase were compared using the Wilcoxon signed-rank test or McNemar test. Univariable and multivariable logistic regression analyses were performed to analyze the effect of each clinical measurement on the binary response to RT. Variables showing significance levels of 0.1 in the univariable analysis were used in the multivariable analysis. All statistical analyses were considered significant at two-tailed P < 0.05.
Results
Patient characteristics
In total, 62 patients (23 male and 39 female) met the inclusion criteria. Their baseline characteristics are shown in Table 1. Their mean age was 52.08 ± 12.09 years. The median duration of GD was 43.7 (24.9–93.9) months and the median duration of GO was 25.5 (13.7–40) months. Forty-five patients (72.6%) had previously been treated with high-dose IV glucocorticoids. Low-dose oral steroids were administered to 34 patients (54.8%) during RT. Thirty patients continued to have active GO despite receiving high-dose IV steroid therapy and were administered supplemental steroids at low doses; four patients received low doses because they were not eligible for high-dose IV steroid therapy. Mean TSH and FT4 were within the normal range prior to RT. TBII was high at 15.02 ± 15.40 IU/L before RT and decreased to 2.56 ± 9.93 IU/mL within 6 months of RT.
Response to orbital radiotherapy
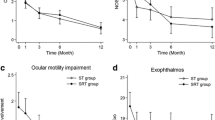
Forty (64.5%) and forty-six (74.1%) GO patients improved at 3 and 6 months after RT, respectively. Changes in individual ophthalmic findings after RT at these time points are shown in Table 2. CAS improved steadily, while proptosis and VA improved up to 3 months and then remained unchanged (Fig. 1). The number of patients with EOM movement ≤30° and CON also significantly decreased after RT. Diplopia improved after RT, but not significantly so. MRD1, PFH, and IOP were unchanged before and after RT. Volumes of the superior rectus, inferior rectus, medial rectus, lateral rectus, and orbital fat significantly decreased after RT (Table 3).

Changes in clinical activity score (CAS), proptosis, and visual acuity after radiotherapy. After orbital radiotherapy, CAS improved steadily, while proptosis and visual acuity improved for up to 3 months and then remained unchanged. **P < 0.01, *P < 0.05.
Complications included facial redness occurring in three patients (4.8%). This was well-controlled with the application of ointment. Cataract formation occurred in one patient (1.6%), who was treated with lens removal and intraocular lens implementation. Malignancy or radiation retinopathy was not detected.
Factors predicting orbital radiotherapy response
Factors associated with a good response to RT in the univariable analysis included concurrent oral steroid use during RT (odds ratio [OR]: 3.75, 95% confidence interval [CI]: 1.11–12.65, P = 0.033); EOM limitation of < 30° (OR: 5.63, 95% CI: 1.56–20.31, P = 0.008); decreased VA (OR: 7.64, 95% CI: 1.56–37.47, P = 0.012); and the sum of EOM volume (OR: 1.18, 95% CI: 0.99–1.41, P = 0.050) (Table 4). GO duration was not prognostic for RT response. Multivariable analysis indicated that an EOM limitation of < 30° (OR: 5.13, 95% CI: 1.25–21.14, P = 0.043) and the sum of EOM volume (OR: 3.68, 95% CI: 1.22–11.11, P = 0.021) remained predictive of a good response to RT. Decreased VA tended to suggest a good response, but this did not reach statistical significance (OR: 4.32, 95% CI: 0.54–34.55, P = 0.168). Furthermore, concurrent oral steroid use during RT was not a significant factor in the multivariable analysis (OR: 0.99, 95% CI: 0.156–6.292, P = 0.921).
Effect of the timing of orbital radiotherapy
Thirty patients received RT for early-active GO (duration ≤24 months) and 32 received RT for late-active GO (duration > 24 months). In patients receiving orbital RT in the late-active phase, the therapeutic goals were as follows: 1) reduction in CAS score (n = 13), 2) disappearance of CON (n = 6), and 3) improvement in EOM limitation or diplopia (n = 13). There were no significant differences in baseline demographics or biochemical characteristics between the early-active and late-active phase groups.
Six months after orbital RT, 22 (68.8%) patients in the late-active phase group and 24 (80.0%) patients in the early-active phase group showed improvement in GO. CAS improved in both groups, but proptosis improved only in the early phase group. Of patients with EOM movement ≤30°, 8 of 21 patients in the early phase group improved after RT, but only 1 in 13 patients in the late phase group improved. VA improved significantly in both groups, and the number of patients with CON decreased in both groups (Table 5).
Discussion
Orbital RT has been used for GO patients as a treatment modality for around 60 years [23], but there have been conflicting reports on its effectiveness. Therefore, we attempted to assess the response rate for RT in patients with GO and tried to determine factors predicting treatment response. Our data demonstrate that 74.1% of patients with GO improved within 6 months of RT. This finding is comparable with responses to high-dose IV steroid treatment, which yields a response rate of 70–80% [24]. Although the patients in our study had limited conditions, which were refractory to high-dose IV steroids or were not eligible for treatment with high-dose IV steroids, our study confirmed that orbital RT is likely to be as effective as steroid therapy, which is the primary treatment for GO. Interestingly, only 64.5% of GO patients treated with RT showed an improvement in response after 3 months, lower than the response rate after 6 months. This indicates that there may be patients improving slowly even after 3 months post-RT, so it is necessary to take at least 6 months to judge the treatment outcome. The slow and long-lasting effect of RT may be a reason for the conflicting reports on the efficacy of RT.
Previous studies have reported that RT is more effective in treating EOM impairment and diplopia than in treating proptosis or soft tissue swelling [13, 15]. However, we found that orbital inflammation and proptosis, as well as EOM impairment and CON, improved after RT. Since orbital RT is recommended as second-line therapy in clinical practice, improvements in CAS and proptosis suggest that it may be an alternative to primary therapy instead of steroid treatment. The presence of fewer side effects in our study provided further support for the wider use of RT. Indeed, a recent study reported that a combination of high-dose IV steroid treatment and RT improved EOM limitation and decreased the reactivation of inflammation to a significantly greater extent than steroid treatment alone [25].
We found that ≤30° EOM limitation and larger EOM volume are good predictors of response to RT. During GO progression, soft tissue swelling and enlargement of EOM occur due to the inflammatory responses of orbital fibroblasts and lymphocytic infiltration. Our findings suggest that RT is effective for relieving edematous changes of EOM in patients with GO. Volumes of all EOM and orbital fat decreased significantly, and EOM limitation improved after RT. A previous study using MRI measurements also found that RT is effective in reducing the EOM volume in GO patients [26].
Several studies have reported that orbital RT is effective in restoring VA impairment and relieving CON [27]. We observed that 10 of 13 CON patients (76.9%) improved within 6 months of treatment and recovered to near-normal vision. Therefore, although our results did not indicate that decreased VA and CON were predictive of a good response to RT, RT should be considered as the preferred treatment modality in patients with CON. A favorable treatment outcome for patients with CON may be relevant to our findings that greater EOM volume predicts a good response to RT. All patients with CON also had enlarged EOM. In a multivariable analysis, variables strongly correlated with CON and VA impairment, such as EOM volume and EOM limitation, may cause an underestimation of the contributions of VA impairment and CON due to multicollinearity, despite statistical controls.
The efficacy of RT remains debatable, even in cases with prolonged GO. The natural course of GO is incompletely defined since it is impossible to determine in patients with moderate-to-severe GO who require immediate disease-modifying therapies [28]. Rundle’s curve, widely used as a descriptor of GO’s putative natural history, depicts progressive deterioration occurring over 6–24 months due to developing autoimmune processes [29]. Orbital RT can be expected to be effective only during the progressive deterioration phase since the underlying mechanism may be correlated with the inflammation process. With a longer GO period, inflammatory infiltration can be replaced by fibrosis, and thus, RT may be less effective. Several studies have emphasized that the selection of patients is important because patients with inactive GO are unlikely to respond to RT or glucocorticoids; thus, orbital RT is recommended in the early stages of the GO [15, 27]. A recent study also reported that a duration of symptoms longer than 18 months was significantly predictive of non-response to RT. [30] However, symptoms according to GO duration are very different in each patient. The active phase of GO can be prolonged or the disease can be reactivated by certain risk factors, including smoking [31]. In some patients, GO changes little in the early stages but may worsen during a prolonged GO period. These long-lasting active GO patients are not in the early phase but may remain in the progressive deterioration phase. Therefore, we separated active GO patients into two groups arbitrarily on the basis of a 24-month GO duration to verify the effect of RT according to duration. Of the patients included in our study, 32 remained in the late-active phase with a distinct deterioration of symptoms or resistant to long-term steroid therapy even after a GO duration of over 24 months. The improvement in CAS and VA after RT in these patients suggests that active treatment is still necessary to suppress inflammatory reactions after more than 24 months of GO duration. We found that a longer GO duration was not a poor prognostic factor. In contrast, only 1 of 13 patients with EOM limitation improved after RT. Fibrosis after prolonged inflammation may be responsible for a poor response to RT. Though diplopia seemed to improve after RT in these patients, the subjective nature of Gorman scoring for the assessment of diplopia may contradict the objective evaluation of ocular motility. In summary, irrespective of the length of GO duration, orbital RT in active GO patients with high CAS or visual disturbance may be a useful treatment for the relief of GO symptoms. Nevertheless, RT may not be effective in patients with an EOM limitation of ≤30° with more than 24 months’ GO duration.
Our study is limited by the relatively small number of patients localized to one tertiary hospital. Due to the nature of this hospital, some patients with a relatively longer GO duration due to previous treatment failures in other hospitals were also included in the study. There may also have been selection bias due to the nature of the retrospective observational study, which could have influenced the results. Prospective randomized studies are required to ascertain the effect of orbital RT on late-active GO.
Conclusions
The efficacy of orbital RT was comparable with that of high-dose IV steroid therapy in treating GO patients who were refractory to high-dose IV steroids or who were not suitable for high-dose IV steroid treatment. In moderate-to-severe active GO patients, orbital RT may help improve high CAS, proptosis, EOM limitation, and CON. Enlargement of EOM and EOM limitation were predictive of a good response to RT. Orbital RT in long-lasting active GO patients may be a suitable therapy for the relief of symptoms including high CAS and poor VA.
Availability of data and materials
Research data are stored in an institutional repository and will be shared upon request to the corresponding author.
Abbreviations
- GO:
-
Graves’ orbitopathy
- GD:
-
Graves’ disease
- EOM:
-
Extraocular muscles
- RT:
-
Radiotherapy
- IV:
-
Intravenous
- EUGOGO:
-
European Group on Graves’ Orbitopathy
- TSH:
-
Thyroid stimulating hormone
- FT4:
-
Free thyroxine
- TBII:
-
Thyroxine binding inhibitory immunoglobulin
- MRD1:
-
Margin reflex distance 1
- PFH:
-
Palpebral fissure height
- IOP:
-
Intraocular pressure
- VA:
-
Visual acuity
- CON:
-
Compressive optic neuropathy
- CAS:
-
Clinical activity score
- HU:
-
Hounsfield units
- CTV:
-
Clinical target volume
References
Wemeau JL, Klein M, Sadoul JL, Briet C, Vélayoudom-Céphise FL. Graves’ disease: introduction, epidemiology, endogenous and environmental pathogenic factors. Ann Endocrinol. 2018;79:599–607.
Yang D, Hiromatsu Y, Hoshino T, Inoue Y, Itoh K, Nonaka K. Dominant infiltration of T(H)1-type CD4+ T cells at the retrobulbar space of patients with thyroid-associated ophthalmopathy. Thyroid. 1999;9:305–10.
Rundle FF. Management of exophthalmos and related ocular changes in graves’ disease. Metabolism. 1957;6:36–48.
Dolman PJ, Rath S. Orbital radiotherapy for thyroid eye disease. Curr Opin Ophthalmol. 2012;23:427–32.
Aktaran S, Akarsu E, Erbagci I, Araz M, Okumuş S, Kartal M. Comparison of intravenous methylprednisolone therapy vs. oral methylprednisolone therapy in patients with graves’ ophthalmopathy. Int J Clin Pract. 2007;61:45–51.
Wang Y, Zhang S, Zhang Y, Liu X, Gu H, Zhong S, et al. A single-center retrospective study of factors related to the effects of intravenous glucocorticoid therapy in moderate-to-severe and active thyroid-associated ophthalmopathy. BMC Endocr Disord. 2018;18:13.
Xu L, Li L, Xie C, Guan M, Xue Y. Thickness of Extraocular muscle and orbital fat in MRI predicts response to glucocorticoid therapy in graves’ Ophthalmopathy. Int J Endocrinol. 2017;2017:3196059.
Matthiesen C, Thompson JS, Thompson D, Farris B, Wilkes B, Ahmad S, et al. The efficacy of radiation therapy in the treatment of graves’ orbitopathy. Int J Radiat Oncol Biol Phys. 2012;82:117–23.
Ohtsuka K, Sato A, Kawaguchi S, Hashimoto M, Suzuki Y. Effect of steroid pulse therapy with and without orbital radiotherapy on graves’ ophthalmopathy. Am J Ophthalmol. 2003;135:285–90.
Marquez SD, Lum BL, McDougall IR, Katkuri S, Levin PS, MacManus M, et al. Long-term results of irradiation for patients with progressive graves’ ophthalmopathy. Int J Radiat Oncol Biol Phys. 2001;51:766–74.
Wakelkamp IM, Tan H, Saeed P, Schlingemann RO, Verbraak FD, Blank LE, et al. Orbital irradiation for graves’ ophthalmopathy: is it safe? A long-term follow-up study. Ophthalmology. 2004;111:1557–62.
Gorman CA, Garrity JA, Fatourechi V, Bahn RS, Petersen IA, Stafford SL, et al. A prospective, randomized, double-blind, placebo-controlled study of orbital radiotherapy for graves’ Ophthalmopathy. Ophthalmology. 2020;127:S160–71.
Mourits MP, van Kempen-Harteveld ML, Garcia MB, Koppeschaar HP, Tick L, Terwee CB. Radiotherapy for graves’ orbitopathy: randomised placebo-controlled study. Lancet. 2000;355:1505–9.
Prummel MF, Mourits MP, Blank L, Berghout A, Koornneef L, Wiersinga WM. Randomized double-blind trial of prednisone versus radiotherapy in graves’ ophthalmopathy. Lancet. 1993;342:949–54.
Tanda ML, Bartalena L. Efficacy and safety of orbital radiotherapy for graves’ orbitopathy. J Clin Endocrinol Metab. 2012;97:3857–65.
Bartalena L, Marcocci C, Tanda ML, Rocchi R, Mazzi B, Barbesino G, et al. Orbital radiotherapy for graves’ ophthalmopathy. Thyroid. 2002;12:245–50.
Bartalena L, Baldeschi L, Boboridis K, Eckstein A, Kahaly GJ, Marcocci C, et al. The 2016 European thyroid association/European group on Graves' Orbitopathy guidelines for the Management of Graves’ Orbitopathy. Eur Thyroid J. 2016;5:9–26.
Chun YS, Park HH, Park IK, Moon NJ, Park SJ, Lee JK. Topographic analysis of eyelid position using digital image processing software. Acta Ophthalmol. 2017;95:e625–32.
Bahn RS, Gorman CA. Choice of therapy and criteria for assessing treatment outcome in thyroid-associated ophthalmopathy. Endocrinol Metab Clin N Am. 1987;16:391–407.
Dolman PJ, Cahill K, Czyz CN, Douglas RS, Elner VM, Feldon S, et al. Reliability of estimating ductions in thyroid eye disease: an international thyroid eye disease society multicenter study. Ophthalmology. 2012;119:382–9.
Mourits MP, Prummel MF, Wiersinga WM, Koornneef L. Clinical activity score as a guide in the management of patients with graves’ ophthalmopathy. Clin Endocrinol. 1997;47:9–14.
Regensburg NI, Kok PH, Zonneveld FW, Baldeschi L, Saeed P, Wiersinga WM, et al. A new and validated CT-based method for the calculation of orbital soft tissue volumes. Invest Ophthalmol Vis Sci. 2008;49:1758–62.
Bartalena L, Marcocci C, Chiovato L, Laddaga M, Lepri G, Andreani D, et al. Orbital cobalt irradiation combined with systemic corticosteroids for Graves' ophthalmopathy: comparison with systemic corticosteroids alone. J Clin Endocrinol Metab. 1983;56:1139–44.
Zang S, Ponto KA, Kahaly GJ. Clinical review: intravenous glucocorticoids for graves’ orbitopathy: efficacy and morbidity. J Clin Endocrinol Metab. 2011;96:320–32.
Kim JW, Han SH, Son BJ, Rim TH, Keum KC, Yoon JS. Efficacy of combined orbital radiation and systemic steroids in the management of graves’ orbitopathy. Graefes Arch Clin Exp Ophthalmol. 2016;254:991–8.
Wu Y, Tong B, Luo Y, Xie G, Xiong W. Effect of radiotherapy on moderate and severe thyroid associated ophthalmopathy: a double blind and self-controlled study. Int J Clin Exp Med. 2015;8:2086–96.
Viani GA, Boin AC, De Fendi LI, Fonseca EC, Stefano EJ, Paula JS. Radiation therapy for graves’ ophthalmopathy: a systematic review and meta-analysis of randomized controlled trials. Arq Bras Oftalmol. 2012;75:324–32.
Piantanida E, Tanda ML, Lai A, Sassi L, Bartalena L. Prevalence and natural history of graves’ orbitopathy in the XXI century. J Endocrinol Investig. 2013;36:444–9.
Rundle FF, Wilson CW. Development and course of exophthalmos and ophthalmoplegia in graves’ disease with special reference to the effect of thyroidectomy. Clin Sci. 1945;5:177–94.
Li YJ, Luo Y, Xie XQ, He WM, Yi C, Li P, et al. The efficacy of intensity modulated radiation therapy in treating thyroid-associated ophthalmopathy and predictive factors for treatment response. Sci Rep. 2017;7:17533.
Cawood TJ, Moriarty P, O’Farrelly C, O'Shea D. Smoking and thyroid-associated ophthalmopathy: a novel explanation of the biological link. J Clin Endocrinol Metab. 2007;92:59–64.
Acknowledgements
Not applicable.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
JHC performed data curation, contributed to the methodology, and was a major contributor in writing the manuscript. JKL analyzed and interpreted the patient data and was a major contributor in reviewing and editing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The institutional review board of Chung-Ang University Hospital approved this study (IRB No 2003–009-19308), and the requirement for informed consent was waived considering its retrospective design. This study adheres to the guidelines of the Declaration of Helsinki. We have read and understood your journal’s policies, and we believe that neither the manuscript nor the study violates any of these.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Choi, J., Lee, J. Efficacy of orbital radiotherapy in moderate-to-severe active graves’ orbitopathy including long-lasting disease: a retrospective analysis. Radiat Oncol 15, 220 (2020). https://doi.org/10.1186/s13014-020-01663-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13014-020-01663-8