
Abstract
Background
Idiopathic pulmonary fibrosis (IPF) is associated with fatal complications after radiotherapy (RT) for lung cancer patients; however, the role of proton therapy to reduce the incidence of life-threatening complications is unclear. Herein, we present the preliminary results of early-stage lung cancer patients having IPF and treated with RT, with a focus on the comparison between X-ray and proton therapy.
Methods
From January 2010 to October 2017, we retrospectively reviewed the medical records of 264 patients with stage I-II non-small cell lung cancer (NSCLC) treated with definitive RT alone. Ultimately, 30 patients (11.4%) who had underlying IPF were analyzed. Among these, X-ray and proton RT were delivered to 22 and 8 patients, respectively. Treatment-related complications and survival outcomes were compared between X-ray and proton therapy.
Results
The median follow-up duration was 11 months (range, 2 to 51 months). All living patients were followed-up at least 9 months. Treatment-related death occurred in four patients (18.2%) treated with X-ray but none with proton therapy. Most patients died within one month after the onset of pulmonary symptoms in spite of aggressive treatment. In addition, the 1-year overall survival (OS) rate in patients treated with X-ray and proton was 46.4 and 66.7%, respectively, and patients treated with proton therapy showed a tendency of better survival compared to X-ray (p = 0.081). Especially, in GAP stage II and III subgroups, patients treated with proton therapy showed significantly increased survival outcomes compared to X-ray (1-year OS rate; 50.0% versus 26.4%, p = 0.036) in univariate analysis.
Conclusions
RT is associated with serious treatment-related complications in patients with IPF. Proton therapy may be helpful to reduce these acute and fatal complications.
Trial registration
retrospectively registered.
Similar content being viewed by others


Background
Surgical resection is the standard of care in the treatment of patients with early-stage non-small cell lung cancer (NSCLC). However, a significant number (30–60%) of patients are medically inoperable due to the reasons including; old age, poor performance status, medical co-morbidities, and inadequate cardio-pulmonary function. Patients deemed unsuitable for surgery are often referred for definitive radiation therapy (RT). For the patients with poor pulmonary function or pulmonary diseases such as interstitial lung disease (ILD), even RT can result in significant complications; however, no universally accepted criteria to define patient suitability for RT have been described.
Pulmonary toxicity is one of the most common treatment-related complications after RT, and can affect the morbidity and mortality of patients with lung cancer [1,2,3,4]. Severe pulmonary toxicity occurs at a rate of 1.5–20% in patients who undergo stereotactic body radiation therapy (SBRT) or at a rate of 5.0–25% after conventionally fractionated RT [5]. Several studies suggest that idiopathic pulmonary fibrosis (IPF) increases the risk of serious, sometimes life-threatening, treatment-related pulmonary complications such as acute exacerbation of IPF and/or pneumonia following RT [6,7,8]. Recently, a few clinical results suggest that proton therapy can be performed more safely in patients with IPF than surgery or X-ray treatment [9,10,11]. However, the role of proton therapy for these vulnerable patients to reduce the incidence of severe RT-related pulmonary complications is still unclear.
Proton therapy for lung cancer patients has started from January 2016 at authors’ institution. Herein, we present the preliminary result of early-stage lung cancer patients who had underlying IPF and were treated with definitive RT, focusing on the comparison between X-ray and proton therapy.
Methods
Patients
After Institutional Review Board approval (#2018–08-108), we retrospectively reviewed the medical records of 264 patients with stage I-II NSCLC treated with definitive RT alone at Samsung Medical Center from January 2010 to October 2017. They were determined to be unsuitable for surgery due to various reasons including old age, poor pulmonary function, and poor performance status. All the diagnosis of underlying pulmonary diseases was confirmed by experienced pulmonologists (H.Y.P. and H.S.Y.). Among these, patients who had no underlying pulmonary disease (65 patients, 24.6%) or other than IPF, such as chronic obstructive pulmonary disease (COPD; 152, 57.6%) or combined pulmonary fibrosis and emphysema (CPFE; 17, 6.4%) were excluded. Ultimately, 30 patients (11.4%) that had underlying IPF were analyzed in the current study. The RT technique (X-ray or proton therapy) was selected individually by the discretion of radiation oncologists. Most of all, patients with severely compromised pulmonary function and/or underlying disease, such as COPD, CPFE, and IPF, were mainly treated with proton therapy. And large tumor size and multiple lesions were also considered. In this study, X-ray and proton RT were delivered to 22 (73.3%) and eight (26.7%) patients, respectively. Treatment-related complications and survival outcomes were compared between X-ray and proton therapy.
Diagnostic and staging scheme for lung cancer and IPF
All tumors were staged based on the seventh edition of the American Joint Committee on Cancer tumor staging criteria. Tumor assessment consisted of complete history taking, physical examination, complete blood counts, chemistry profiles, pulmonary function test (PFT), chest X-ray, computed tomography (CT) scan of the chest and upper abdomen, whole-body 18F-fluorodeoxyglucose positron emission tomography with CT (FDG-PET-CT) scan, and magnetic resonance imaging of the brain as a routine staging work-up. The PFT including both spirometry and diffusing capacity were performed before treatment. Detailed measurements included (1) forced expiratory volume in one second (FEV1), (2) forced vital capacity (FVC), (3) ratio of the two volumes (FEV1/FVC), (4) diffusing capacity of the lung for carbon monoxide (DLCO), and (5) DLCO divided by alveolar ventilation (DLCO/VA). For the diagnosis of IPF, the presence of a typical radiological pattern, which is the coarse reticulation with honeycombing appearance in peripheral and predominantly basal lung area, was seen on high-resolution CT (HRCT). Spirometry typically revealed a reduction in the vital capacity and DLCO. The patients with IPF also showed oxygen desaturation with a six-minute walk test. The GAP model, including four baseline variables (sex, age, and two lung physiology variables; FVC and DLCO) was used for IPF staging [12].
Radiation treatment
The gross tumor volume (GTV) was delineated under the lung window setting. The internal target volume (ITV) was delineated following four-dimensional CT with consideration of respiratory tumor motion. The clinical target volume (CTV) was generated with a 5 mm expansion of the GTVs in all directions, and was then modified considering the adjacent anatomic structures. The planning target volume (PTV) was generated with 5 mm expansion of the CTVs. The percentage volume of lung receiving ≥20 Gy (V20) of the lung was tried to be kept ≤35% and the mean lung dose was ≤20 Gy. Maximum doses to the spinal cord and esophagus were not to exceed 45 Gy and 60 Gy, respectively. The prescription policy was to deliver at least 97% of the prescribed dose to 95% of the CTVs.
Treatment planning for X-ray, Pinnacle treatment planning system, version 9.2 (Royal Phillips Electronics, Miami, FL) was used to calculate the dose distributions, and two different dose-fractionation schedules were used to deliver 60 Gy in either 20 fractions over 4 weeks or 15 fractions over 3 weeks. The biologically equivalent doses at α/β of 10 Gy (BED10) were 78 Gy and 84 Gy, respectively. Dose selection depended on the location, size, and geometry of the tumor in relation to the esophagus. If the shortest distance between the CTV margin and the esophagus was ≥1.5 cm, 60 Gy in 15 fractions was preferred to 60 Gy in 20 fractions. For SBRT for small size and peripherally located tumors, 60 Gy in 4 fractions was delivered. Eleven patients were treated with SBRT, 10 with 3-dimensional conformal RT (3DCRT), and one with intensity-modulated RT (IMRT) as it was difficult to safely cover the whole disease extent while satisfying the dose-volume constraints using the 3DCRT technique.
Treatment planning for proton, RayStation treatment planning system, version 6.2 (Raysearch Laboratories AB, Stockholm, Sweden) was used. Line scanning method was used for the proton therapy in all patients with the proton therapy system at our institute (Sumitomo, Japan). Six patients were treated with stereotactic body proton therapy (SBPT, 60–64 CcGE in 4–8 fractions) and two with intensity-modulated proton therapy (IMPT, 60 CcGE in 20 fractions).
Follow-up
Physical examination, blood tests, chest CT scan, and/or PET-CT were performed every 3 months for 2 years after RT and then every 6 months thereafter to detect disease progression during follow-up. Revised Response Evaluation Criteria In Solid Tumors (RECIST) guidelines (Version 1.1) were used for tumor response evaluation. Treatment-related pulmonary complications, excluding infection-related cases, were evaluated using the Common Terminology Criteria for Adverse Events version 4.0.
Statistical analysis
Overall survival (OS) was defined as the time from the start date of the RT until the date of death from any cause or the latest documented follow-up. The 1-year rate of OS was calculated using the Kaplan–Meier method and was compared using the log-rank test. Factors that were thought to be relevant were entered into a Cox proportional hazard regression analysis to account for potential confounding factors and to determine independent prognostic factors. To compare the clinical characteristics and dose-volume parameters, Chi-square or Fisher’s exact test was used to assess categorical variables and independent-sample t test was used to assess continuous variables. A p value< 0.05 was regarded as statistically significant in two-tailed tests. Statistical analysis was performed using SPSS software, standard version 24.0 (IBM Corporation, Armonk, NY, USA).
Results
Patient and tumor characteristics
Overall clinical characteristics according to treatment were described in Table 1. The median age of the population was 76 years (range, 62 to 85 years). Clinical characteristics were similar between the X-ray and proton groups, except for ECOG performance status. Patients who underwent proton therapy showed poorer pulmonary function compared to those undergoing X-ray, although the difference was not statistically significant. When the DLCO were stratified into two categories (> 60% vs. ≤ 60%), the numbers of patients that had poor diffusing capacity in X-ray and proton group were 13/22 (59.1%) and 6/8 (75.0%), respectively. In addition, in the aspect of GAP index, the numbers of patients that presented with high scores (GAP stage II and III) in X-ray and proton groups were 13/22 (59.1%) and 7/8 (87.5%), respectively. In terms of planning dose-volume parameters (Table 2), the CTV was significantly larger in the proton group than in the X-ray group (p = 0.007), while the normal tissue doses generally met the constraints and dose-volume parameters for lung, heart, esophagus, and spinal cord were generally similar. Of note, the mean lung dose and the percentage volumes of lung receiving ≥5 Gy and ≥ 20 Gy were similar between the two groups.
Survival outcomes and treatment-related complications
The median follow-up duration was 11 months (range, 2 to 51 months). The 6-month OS rates in patients treated with X-ray and proton were 67.9 and 100%, and the 1-year OS rate was 46.4 and 66.7%, respectively (Table 3). Patients treated with proton therapy showed a tendency of better survival compared to X-ray (p = 0.081) (Fig. 1). And only the occurrence of severe pulmonary complication was significantly associated with decreased OS (73.7% vs. 24.0%, p = 0.009), while performance status (p = 0.986) and RT technique (p = 0.318) were not associated with OS in univariate analysis. There was no statistically significant prognostic factors for OS in multivariate analysis after adjusting confounding factors.

Overall survival curves according to treatment; 1-year OS rate in patients of X-ray and proton groups were 46.4 and 66.7%, respectively
A statistically significant difference of survival was shown based on GAP stage, and the 1-year OS rate in stage I, II, and III was 78.8, 46.3, and 0%, respectively (p = 0.024). In subgroup analysis based on GAP stage, patients treated with proton therapy showed significantly increased survival outcome compared to X-ray in GAP stage II and III groups (1-year OS rate; 50.0% versus 26.4%, p = 0.036, Fig. 2). However, there was no statistically significant prognostic factors for OS in multivariate analysis after adjusting confounding factors.

Overall survival curves according to treatment in GAP stage II and III subgroups; 1- year OS rate in patients of X-ray and proton groups were 26.4 and 50.0%, respectively
The incidence of severe treatment-related pulmonary complications did not differ significantly between X-ray and proton groups, although it was observed less frequently in the proton group (40.9% vs. 12.5%, p = 0.222). All living patients were followed-up at least 9 months, and treatment-related death occurred in four patients (18.2%) treated with X-ray but none with proton therapy (Table 3). Most patients died within one month after the onset of symptom in spite of aggressive treatment. The clinical courses of patients are described in Table 4.
Discussion
IPF is a pulmonary disease associated with a dismal prognosis. The median survival of patients with IPF ranges from 2.5 years to 3.5 years and the 5-year survival ranges between 20 and 40% [13]. The condition can be acutely exacerbated by a range of triggering factors, including infection, surgery, and RT. Yamashita et al. [6] demonstrated that severe pulmonary toxicity was observed in nine out of thirteen patients with IPF after SBRT, and seven of these cases were fatal. The presence of IPF shadow on CT was found to correlate well with the severe pulmonary toxicity. However, there was no correlation between the DVH parameters and the severe pulmonary toxicity. This may imply that even a small volume of RT including SBRT is not safe. Accordingly, they suggested that pre-screening for an IPF pattern on CT should be performed before SBRT in patients with lung cancer and underlying IPF. Lee et al. [7] evaluated the relationship between interstitial lung changes in the pre-radiotherapy CT and symptomatic pulmonary toxicity. The risk of pulmonary toxicity grade ≥ 2, ≥3, or ≥ 4 was higher in patients with interstitial lung change than patients without (grade 2, 15.6 to 46.7%, p = 0.03; grade 3, 4.4 to 40%, p = 0.002; grade 4, 4.4 to 33.3%, p = 0.008). Four out of the five patients with grade 5 pulmonary toxicity had diffuse interstitial changes on pre-radiotherapy CT. Recently, Ono et al. [9] reported the clinical results of proton RT in patients with IPF. The cumulative incidence of pulmonary toxicity was 19.8%, including one case of treatment-related death. This study was the first report on the incidence of pulmonary toxicity after proton RT in IPF patients. They showed that grade 4 or 5 pulmonary toxicity occurred at a rate of 6.3%, which was lower than that reported in previous studies with X-ray treatment. This result suggests that proton RT may reduce the incidence of life-threatening pulmonary complications in patients with IPF compared to that with X-ray irradiation.
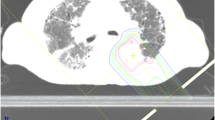
Current study has several limitations. First, it is a retrospective analysis and there may be some selection biases. Second, the sample size is too small to show a statistical significance of difference between the two groups. Despite the lack of statistical significance due to small number of cases, our preliminary analysis is the first one to directly compare X-ray and proton therapy for lung cancer patients with IPF, and shows a promising result that is concordant with previous studies (summarized in Table 5). Although patients that received proton therapy had poorer diffusing capacity and higher GAP stages compared to X-ray, the incidence of severe treatment-related pulmonary complications was observed less frequently in the proton group (40.9% in X-ray vs. 12.5% in proton), and the incidence of treatment-related death occurred in four patients (18.2%) treated with X-ray (Fig. 3) but none with proton therapy. In addition, patients treated with proton therapy showed a tendency of better overall one-year survival compared to X-ray. Especially, proton therapy showed significantly increased survival outcomes compared to X-ray in patients with higher GAP stage (II and III) subgroups (1-year OS rate; 50.0% versus 26.4%, p = 0.036). These promising results with proton therapy may be because proton therapy could affect a smaller lung volume than X-ray irradiation. However, there were no statistically significant differences in the dosimetric factors of the patients, including MLD, V5, V10 and V20 of lung although CTV was significantly larger in the proton RT group. We hope our ongoing prospective study with a large number of patients and systematic evaluation of pre- and post-treatment lung functions could confirm the benefit of proton therapy for patients with severely compromised pulmonary function and/or IPF.

Chest CT axial imaging of the patient who showed grade 5 radiation pneumonitis after radiotherapy; (3a) Pretreatment chest CT image, (3b) At 1 month follow-up, and (3c) At 2 months follow-up
Conclusions
Our retrospective analysis showed that RT is associated with serious treatment-related complications in patients with IPF. Proton therapy may be helpful to reduce these acute and fatal pulmonary complications in these vulnerable patients. Currently, a phase 2 prospective trial with proton RT in patients with severely compromised pulmonary function and/or IPF is ongoing at authors’ institution.
Abbreviations
- 3DCRT:
-
3-Dimensional conformal RT
- COPD:
-
Chronic obstructive pulmonary disease
- CPFE:
-
Combined pulmonary fibrosis and emphysema
- CT:
-
Computed tomography
- CTV:
-
Clinical target volume
- DLCO:
-
Diffusing capacity of the lung for carbon monoxide
- DLCO/VA:
-
DLCO divided by alveolar ventilation
- FDG-PET-CT:
-
18F-fluorodeoxyglucose positron emission tomography with CT
- FEV1 :
-
Forced expiratory volume in one second
- FVC:
-
Forced vital capacity
- GTV:
-
Gross tumor volume
- HRCT:
-
High-resolution CT
- ILD:
-
Interstitial lung disease
- IMRT:
-
Intensity-modulated RT
- IPF:
-
Idiopathic pulmonary fibrosis
- ITV:
-
internal target volume
- NSCLC:
-
Non-small cell lung cancer
- OS:
-
Overall survival
- PFT:
-
Pulmonary function test
- PTV:
-
Planning target volume
- RT:
-
Radiotherapy
- SBRT:
-
Stereotactic body radiation therapy
- V20 :
-
Percentage volume of lung receiving ≥ 20 Gy
References
Claude L, Perol D, Ginestet C, Falchero L, Arpin D, Vincent M, et al. A prospective study on radiation pneumonitis following conformal radiation therapy in non-small-cell lung cancer: clinical and dosimetric factors analysis. Radiother Oncol. 2004;71:175–81.
Shi A, Zhu G, Wu H, Yu R, Li F, Xu B. Analysis of clinical and dosimetric factors associated with severe acute radiation pneumonitis in patients with locally advanced non-small cell lung cancer treated with concurrent chemotherapy and intensity-modulated radiotherapy. Radiat Oncol. 2010;5:35.
Robnett TJ, Machtay M, Vines EF, McKenna MG, Algazy KM, McKenna WG. Factors predicting severe radiation pneumonitis in patients receiving definitive chemoradiation for lung cancer. Int J Radiat Oncol Biol Phys. 2000;48:89–94.
Park YH, Kim JS. Predictors of radiation pneumonitis and pulmonary function changes after concurrent chemoradiotherapy of non-small cell lung cancer. Radiat Oncol J. 2013;31:34–40.
Stanic S, Paulus R, Timmerman RD, Michalski JM, Barriger RB, Bezjak A, et al. No clinically significant changes in pulmonary function following stereotactic body radiation therapy for early- stage peripheral non-small cell lung cancer: an analysis of RTOG 0236. Int J Radiat Oncol Biol Phys. 2014;88:1092–9.
Yamashita H, Kobayashi-Shibata S, Terahara A, Okuma K, Haga A, Wakui R, et al. Prescreening based on the presence of CT-scan abnormalities and biomarkers (KL-6 and SP-D) may reduce severe radiation pneumonitis after stereotactic radiotherapy. Radiat Oncol. 2010;5:32.
Lee YH, Kim YS, Lee SN, Lee HC, Oh SJ, Kim SJ, et al. Interstitial lung change in pre-radiation therapy computed tomography is a risk factor for severe radiation pneumonitis. Cancer Res Treat. 2015;47:676–86.
Yamaguchi S, Ohguri T, Ide S, Aoki T, Imada H, Yahara K, et al. Stereotactic body radiotherapy for lung tumors in patients with subclinical interstitial lung disease: the potential risk of extensive radiation pneumonitis. Lung Cancer. 2013;82:260–5.
Ono T, Hareyama M, Nakamura T, Kimura K, Hayashi Y, Azami Y, et al. The clinical results of proton beam therapy in patients with idiopathic pulmonary fibrosis: a single center experience. Radiat Oncol. 2016;11:56.
Harada H, Murayama S. Proton beam therapy in non-small cell lung cancer: state of the art. Lung Cancer (Auckl). 2017;8:141–5.
Berman AT, James SS, Rengan R. Proton beam therapy for non-small cell lung Cancer: current clinical evidence and future directions. Cancers (Basel). 2015;7:1178–90.
Kolb M, Collard HR. Staging of idiopathic pulmonary fibrosis: past, present and future. Eur Respir Rev. 2014;23:220–4.
King TE Jr, Pardo A, Selman M. Idiopathic pulmonary fibrosis. Lancet. 2011;378:1949–61.
Acknowledgements
Not applicable
Funding
This study was supported by a grant from the Creative Research Program (#OTC1180381), which was funded by the Samsung Medical Center, Sungkyungkwan University School of Medicine, Korea.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
HRP provided the conception and design of this study, HKK, WJL, and BSP analyzed and interpreted the patient data, HKK, HYP, and HSY have been involved in drafting the manuscript. HRP, HYP, and HSY have been involved in revising it critically for important intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Institutional Review Board (#2018–08-108).
Consent for publication
Written informed consent for publication of their clinical details and/or clinical images was obtained from the patient.
Competing interests
The authors declared that the they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kim, H., Pyo, H., Noh, J.M. et al. Preliminary result of definitive radiotherapy in patients with non-small cell lung cancer who have underlying idiopathic pulmonary fibrosis: comparison between X-ray and proton therapy. Radiat Oncol 14, 19 (2019). https://doi.org/10.1186/s13014-019-1221-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13014-019-1221-4