
Abstract
Background and purpose
The aim of this retrospective study was to compare volumetric-modulated arc therapy using simultaneous integrated boosts (SIB-VMAT) of 45 Gy/55 Gy in 25 fractions with three-dimensional conformal radiotherapy (3D–CRT) in preoperative chemoradiation for rectal cancers.
Methods and materials
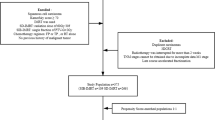
In the propensity score-matching analysis of 1:2, we selected 60 patients from the SIB-VMAT group and 120patients from the 3D–CRT group matched pairings out of 145 patients between 2005 and 2015. The regimen of concurrent combined chemotherapy was oral uracil/tegafur plus leucovorin with/without irinotecan.
Results
There were no significant differences between the two groups, in pathological complete response rates (pCR) (11% in the 3D–CRT group vs. 17% in the SIB-VMAT group, P = 0.39), pathological response rates (44% vs. 60%, P = 0.77), disease-free survival (P = 0.32), or local control (P = 0.52). The SIB-VMAT method marginally improved the rate of pathological grade 2–3 effects and the OS was significantly better in patients with grade 2–3 effects. Recurrence was seen in 36 patients (30%) in the 3D–CRT group and 19 patients (32%) in the SIB-VMAT group. The first distant recurrence site in the SIB-VMAT group was liver in 6 patients and lung in 8 patients. The obvious radiation-induced late toxicity in the SIB-VMAT group was recto-vesical fistula in two patients.
Conclusions
The SIB-VMAT may be a promising method for preoperative CRT of rectal cancer.
Similar content being viewed by others


Introduction
Combination treatment composed of surgery and 5-fluorouracil-based chemotherapy concurrently combined with whole pelvis irradiation is suggested for most patients with stage II-III rectal cancer [1,2,3,4]. The pre- or post-operative pelvis radiation therapy (RT) for these patients also continues to improve [5].
Many randomized phase III studies have estimated the efficacy of adding chemotherapy to preoperative RT in rectal cancer [6]. The estimated advantages of adding chemotherapy to RT include an increase in local RT sensitivity and a better control of the systemic disease by eradicating microscopic distant metastases. Additionally, neoadjuvant chemoradiation therapy (CRT) provides the possibility of improving the proportion of patients with sphincter preservation and/or pathologic complete response (pCR).
If image-guided radiation therapy (IGRT) and volumetric modulated arc therapy (VMAT) are used, normal tissue damage is less likely to occur, and the setup margins can be minimized; in addition, in another advantage of this technique, it may be possible to deliver a simultaneous integrated radiation boost (SIB) to the gross tumor volume [7].
The aim of this retrospective study was to compare SIB-VMAT of 45 Gy/55 Gy in 25 fractions with conventional radiotherapy in preoperative chemoradiation of rectal cancers.
Methods and materials
Patients had to present with histopathologically confirmed rectal adenocarcinoma involving the middle or lower third of the rectum (below the peritoneal reflection) and evidence of T3/T4, any N, M0 disease on MRI or endoluminal ultrasound and normal liver, renal, and bone marrow functions. Patients with unresectable metastatic disease at diagnosis were excluded. Other exclusion criteria were as follows: prior chemotherapy for rectal cancer or any prior pelvic irradiation; severe heart disease, uncontrolled infection or metabolic disorders; or severe neurologic impairment or inflammatory bowel disease.
Three-dimensional conformal radiotherapy (3D–CRT) of 50.4 Gy was performed in 145 patients from February 2005 to December 2011 and from April 2014 to September 2015. SIB-VMAT of 45 Gy/55 Gy in 25 fractions was administered to 60 consecutive patients between January 2012 and March 2014.
Radiotherapy technique
3D–CRT group
RT began on the first day of chemotherapy and was administered 5 times per week with a daily fraction of 1.8 Gy. Initially, the entire pelvis was treated with 3- or 4-field techniques to 50.4 Gy in a supine position using a 10 MV X-ray accelerator. The irradiation field wasn’t changed on the way as one series. The clinical target volume (CTV) included the entire pelvic cavity, the anal canal, the primary tumor, mesorectal and presacral lymph nodes, nodes along the internal iliac artery, lumbar nodes up to the level of the lower border of the fifth lumbar vertebra, and nodes at the obturator foramen. The superior border of the entire pelvis was placed at the bifurcation of internal and external iliac arteries. Uniform planning target volume (PTV) margins of 5 mm in the lateral, the anteroposterior, and the craniocaudal directions were applied. A 3-D conformal technique has been used with planning CT. The same machine had been used for SIB-VMAT groups.
SIB-VMAT group
Preoperative RT was carried out with IMRT–IGRT using the Elekta Synergy linac with Agility collimating device. The details of the SIB-VMAT method was described in our previous report [8]. All patients received a dose of 45 Gy in daily fractions of 1.8 Gy to the primary tumor, the mesorectum, and draining lymph nodes. The 60 patients of the SIB-VMAT group received an SIB of 0.4 Gy per day on the primary tumor, up to a total dose of 10 Gy (Fig. 1). We tried to minimize the volume of small bowel receiving 15 Gy or greater (V15-SB <150 ml) and a mean bladder dose <21 Gy. Before each treatment session, patients underwent daily image guidance using the integrated kV-CT modality and were repositioned after coregistration of these images with the planning kV-CT scan. Patients were advised to drink 250 ml of water 60 min prior to the planning CT and prior to every treatment session.

A dose distribution in the SIB-VMAT group. (sky blue line = GTV, purple = PTV1, orange = CTV, green = PTV2, pink = small bowel)
Chemotherapy
The most common concurrent chemotherapy regimen (89%) was 5-days-on/2-days-off oral uracil/tegafur (UFT) of 300 mg/m2/day plus leucovorin (LV) of 75 mg/body/day. The second most common concurrent chemotherapy regimen (11%) was UFT, LV, and irinotecan (CPT-11). Although CPT-11 is not a standard chemotherapy agent in the management of rectal cancer as a preoperative setting, it has been used for a limited time in preoperative CRT.
Surgical technique
A variety of surgical approaches, depending on the location and extent of disease, were used to treat primary rectal cancer lesions. These methods include invasive procedures such as transabdominal resection as low anterior resection (LAR), intersphincteric resection (ISR), and abdominoperineal resection (APR) [9, 10]. All surgeries were performed by colorectal specialists. The interval between radiotherapy and surgery was planned as not less than 4 weeks. In most patients, surgery has been performed around the 8th week after completing CRT.
Pathological analysis
Analysis of the surgical specimens included determination of the following parameters: a) histologic type of the tumor; b) degree of extension of the tumor through the rectal wall; c) nodal involvement; and d) status of proximal and distal margins. Post-CRT histological tumor regression was graded according to the seventh edition of the Japanese General Rules for Clinical and Pathological Studies on Carcinoma of the Colorectum: Grade 0, neither necrosis nor regression change; Grade 1a, >2/3 viable residual tumor cells; Grade 1b, approximately 1/3 to 2/3 viable residual tumor cells; Grade 2, <1/3 viable tumor cells; and Grade 3, no viable residual tumor cells [11]. In this study, both grades 1a and 1b were classified together as grade 1 in the same manner as many previous studies [7, 12, 6].
Statistical analysis
The primary endpoint of this study is the comparison of pCR rate in the surgery specimen. The secondary endpoints are the comparison of disease-free survival, local control, and late toxicity.
We applied a 1:2 propensity score matching (PSM) ratio to minimize such differences as age, sex, pre-CRT clinical T stage, N stage and pre-CRT serum carcinoembryonic antigen (CEA) value, with/without combined CPT-11, with /without anal canal invasion, and pathological type. The surgical technique and interval between radiotherapy and surgery were not included as matching factors, because we considered that these factors could be influenced greatly by RT method such as 3D–CRT or SIB-VMAT and these were a part of treatment effects due to differences in RT method. In the PSM analysis, we selected 60 patients from the SIB-VMAT group with 120 matched pairings of the 3D–CRT group using a randomized nearest-neighbor algorithm. A 1:2 matching was performed to minimize the effects of small sample size on PSM and because there was a wide difference in the number of patients in each group before PSM (60 and 145 patients). We used “R” as statistics analysis software (http://www.R-project.org/).
With regard to comparison of the background factors of the two groups, the continuous variable examines the difference of means by an unpaired t-test, and a chi square test was performed for the nominal variable. Survival periods were calculated from the start of 3D–CRT or SIB-VMAT. The survival functions were estimated with the Kaplan-Meier method estimator, and log-rank tests were used to compare the survival distributions. The borderline-difference was defined as P < 0.1.
Results
With a median time of 8.1 weeks (range; 4.1–14.5 weeks) after completion of preoperative RT, LAR, ISR, APR, and other operative methods (Hartmann’s operation or pelvic evisceration) were performed in 70, 18, 9, and 3% of patients, respectively. In 96% patients, the interval between preoperative RT end and surgery was more than 5 weeks and in 37% patients, it was more than 9 weeks. There was no significant difference by two groups about this interval by an unpaired t-test (P = 0.69). In one patient in the 3D–CRT group, local resection, which was not standard treatment, had been performed repeatedly at his wish. Since it was thought that whether pCR or not of the primary endpoint can be evaluated, this patient was not excluded.
The clinicopathological characteristics were balanced and evenly distributed between the groups (all P > 0.1) except in those with/without anal canal invasion (P = 0.0040) (Table 1). The median follow-up time was 44.7 months in all 180 patients, 38.1 months (range; 16.6–50.5 months) in the SIB-VMAT group, and 59.2 months (range; 8.6–131.7 months) in the 3D–CRT group. In all 180 patients, there was no significant difference in disease-free survival (DFS), overall survival (OS), and local control (LC) between an radiation-surgery interval ≤ 7 weeks vs. >7 weeks (P = 0.42, 0.55, and 0.56) or between ≤9 weeks vs. >9 weeks (P = 0.54, 0.59, and 0.19), respectively.
The operative method LAR/ISR with sphincter preservation was performed in 95 patients (79%) in the 3D–CRT group and 53 patients (88%) in the SIB-VMAT group (P = 0.13). In both groups, there was no significant difference in either pCR rate (11% in the 3D–CRT group and 17% in the SIB-VMAT group, P = 0.39) or pathological response rate (pRR) of effective grades 2 plus 3 rates (44% and 60%, respectively, P = 0.065). The number of patients with pathological responses grades 0 / 1a / 1b / 2 / 3 were 0% / 21% / 35% / 33% / 11% in the 3D–CRT group and 3% / 11% / 29% / 43% / 17% in the SIB-VMAT group, respectively (P = 0.102). The mean / median interval between radiotherapy and surgery was 13.9 / 13.7 weeks of the patients with grades 2–3 and 14.0 / 13.7 weeks of those with grades 0–1. We could not adjust for numbers with or witho + ut anal canal invasion even after PS matching, and there were significantly more patients with anal canal invasion in the SIB-VMAT group (27% vs. 9%, P = 0.0040). The radial margin (RM) positive ratewas 0% in the SIB-VMAT group and 1.7% (two patients) in the 3D–CRT group.
The Kaplan-Meiersurvival curves for the matched groups are shown in Fig. 2. In the survival analysis of the matched 180 patients, the 2-y and 3-y OS was 98.1% (95% CI; 92.6–99.5%) and 95.7% (95%CI; 88.9–98.4%), respectively, for 3D–CRT patients and 98.3% (95%CI; 88.6–99.38%) and 96.0% (95%CI; 94.5–99.0%), respectively, for SIB-VMAT patients (P = 0.77). The 2-y and 3-y DFS (Fig. 3) was 80.3% (95% CI; 71.6–86.6%) and 76.7% (95%CI; 67.4–83.7%), respectively, for 3D–CRT patients and 75.0% (95%CI; 61.9–84.1%) and 68.9% (95%CI; 55.1–79.2%), respectively, for SIB-VMAT patients (P = 0.32). Since both the more recent cases from 2014 to 2015 and the older cases were included in the 3D–CRT group, there are more censored cases in the first half of the curve. The 2-y and 3-y LC (Fig. 4) was 94.4% (95% CI; 87.8–97.4%) and 92.0% (95%CI; 84.6–96.0%), respectively, for 3D–CRT patients and 93.2% (95%CI; 82.9–97.4%) and 91.1% (95%CI; 79.8–96.2%), respectively, for SIB-VMAT patients (P = 0.52). Pelvic disseminated recurrence was not included as a local recurrence.

Kaplan-Meier overall survival curves for the matched groups. Red line = SIB-VMAT group. Black line = 3D–CRT group

Kaplan-Meier disease-free survival curves for the matched groups. Red line = SIB-VMAT group. Black line = 3D–CRT group

Kaplan-Meier local control curves for the matched groups. Red line = SIB-VMAT group. Black line = 3D–CRT group
The 3-y OS was 97.6% vs. 93.9% in patients less than vs. not less than 65 years old (log-rank P = 0.86); 91.8% vs. 96.7% in patients with less than vs. not less than 20 ng/mL of pre-CRT serum CEA (P = 0.16); 95.8% vs. 95.8% between less than vs. not less than 3/4-circumferential (P = 0.41); 98.5% vs. 93.3% between cN0 vs. cN1–2 (P = 0.50); 100% vs. 95.1% between patients with vs. without CPT-11 (P = 0.86); 100% vs. 95.5% between cT1–2 vs. cT3–4 (P = 0.19); 100% vs. 95.3% between those with effective grade 3 vs. the others (P = 0.21); 94.6% vs. 98.8% between those with effective grade 1 vs. grades 2–3 (P = 0.0067, 84.5% vs. 95.8% in 5-y OS); 97.7% vs. 92.8% between those with well-differentiated adenocarcinoma vs. the others (P = 0.82); 95.8% vs. 95.9% between those with vs. without anal canal invasion (P = 0.26); and 100% vs. 93.9% between female vs. male patients (P = 0.23).
Recurrence was seen in 36 patients (30%) in the 3D–CRT group and 19 patients (32%) in the SIB-VMAT group. Local and distant recurrence occurred in 10 patients (8%) and 26 patients (22%) in the 3D–CRT group and 6 patients (10%) and 13 patients (22%) in the SIB-VMAT group. The first distant recurrence in the SIB-VMAT group was liver metastasis in six patients and lung metastasis in eight patients.
The acute toxicity in the SIB-VMAT group was fatigue in 26%/63%/12% of grades 0/1/2, respectively, appetite loss in 34%/36%/30%, abdominal pain in 26%/60%/15%, anal pain in 4%/17%/79%, nausea in 53%/30%/17%, diarrhea in 19%/38%/42%, and urinary tract symptom in 6%/45%/49%. No grade 3–5 acute toxicity was seen. The late toxicity in the SIB-VMAT group was only radiation-induced recto-vesical fistula in two patients at 15 and 22 months after CRT, respectively.
The acute toxicity in the 3D–CRT group was grade 1–2 diarrhea in 83% and grade 1–2 anal pain in 75%. No grade 3–5 acute toxicity was seen. The late toxicity in the 3D–CRT group was radiation-induced recto-vesical fistula in one patient at 6 months after CRT and recto-vaginal fistula in another patient. Additionally, pelvic suppuration, probably caused by CRT, was seen in one patient.
Discussion
This is a study on rectal cancer patients treated with preoperative chemoradiation with a V-MAT SIB technique, compared with an historical group of patients treated with 3D technique at a single institution. No statistically significant difference could be found for pCR and pRR, DFS and LC. Late toxicity seemed to be acceptable. Although interval between preoperative RT and surgery has been reported an important prognostic factor in treatment of rectal cancer [13,14,15,16], there was no significant difference between both groups in the present study.
The addition of chemotherapy to preoperative radiotherapy has been established as the standard of care for patients with cT3–4 rectal cancer. Current strategies in preoperative treatment of rectal cancer have been based mainly on the combination of oxaliplatin and molecular targeted drugs plus RT in order to improve the pCR rate and to decrease the high incidence of distant recurrences. There have now been seven major trials on oxaliplatin [17,18,19,20,21,22,23] and two of those demonstrated a benefit for oxaliplatin regarding DFS [20, 23]. Meta-analyses have also demonstrated this benefit [24, 25]. In patients receiving neoadjuvant treatment, CRM positivity is one of the strongest predictive factors of local recurrence [26]. In this study, CRM positivity or negativity in the surgical specimens were not adjusted between the two groups because only pre-CRT factors were adjusted.
About 20% of patients showed a pCR after preoperative treatment [27, 28]. Some reports have claimed that patients with pCR improve survival compared with those with intermediate or poor regression after preoperative CRT in rectal cancer [12, 6, 29]. In the present study, however, the pathologically determined response to preoperative CRT was not correlated with long-term prognosis, and the 3-year OS was 100 and 96% for patients with complete response and the others, respectively (P = 0.21), though the OS of patients with effective grades 2–3 was significantly better than those with grade 1 (P = 0.0067). Additionally, since there was a borderline-difference in effective grades 2 plus 3 rates (60% in the SIB-VMAT group vs. 44% in the 3D–CRT group, P = 0.065), if the more patients are compared, the SIB-VMAT method may lead to the benefit of survival.
The 3D–CRT group contains the patients in older time from 2005 and we think that a difference in the LAR/ISR rate is mainly related to the period, not to the effect of CRT. Additionally, the reason that we could not adjust for the presence or absence of anal canal invasion was likely because cases with anal canal invasion already comprised a significant proportion of the 27% in the SIB-VMAT group, and in the 3D–CRT group the invasion did not reach this value even if a lot of cases with invasion were selected.
In the present study, the 3-year LC, DFS, and OS in the SIB-VMAT group were 91, 69, and 96%, respectively. It seems that our results were not inferior to the previous other studies [6, 30,31,32].
Patients with locally advanced rectal cancer receive preoperative CRT as the standard of care, producing a pCR in 10–20% and a complete clinical response in 20–30% of patients [33]. In the phase II SHOGUN trial that our institution took part in, the pCR rate in 45 patients was very high, 27.3%, after preoperative CRT with S-1 plus oxaliplatin plus radiotherapy with 50.4 Gy in 28 fractions for clinical stage T3 or T4 (any N, M0) locally advanced rectal carcinoma [34].
Treatment-related toxicity was decreased by the creation of steep dose gradients and reduction of the CTV to the PTV margin, and the implementation of IMRT and IGRT results in a minimization of the irradiated volume of the surrounding healthy tissues such as the small bowel and bladder. In the present study, 2 out of 60 patients (3.3%) in the SIB-VMAT group experienced late grade 3–4 GI toxicity but no severe genitourinary (GU) toxicity. This rate is similar in the previous reports and is well-tolerated [31, 32, 35,36,37,38,39].
A larger volume of normal tissue will be exposed to low-dose radiation by VMAT. The resulting steep dose gradients of VMAT decrease the volume of normal tissue exposed to high doses. The effect of both factors on the incidence of radiation-induced second malignancies is still left open [40, 41]. For rectal cancer patients receiving short-course preoperative RT, the Swedish Rectal Cancer Trial and the Dutch TME trial reported 11.7 and 14% secondary cancers after a median follow-up time of 14 years and 12 years, respectively [42, 43].
The majority of RCTs on the addition of oxaliplatin to standard CRT reported almost the same difference in pCR as in this study and, in all but one study, the difference was not significant [17,18,19]. In this study, the significantly higher number of patients with anal canal infiltration (27% vs. 9%) in the VMAT-SIB group might have negatively influenced tumor response as well as DFS and could explain, at least in part, the lack of a pCR difference between the two RT modalities, since rectal adenocarcinoma with infiltration of the anal canal is generally more aggressive tumors. The median follow-up was significantly longer in the 3D–CRT arm compared to that in the VMAT-SIB arm, and this difference automatically generates a major statistical bias as a limitation of this study. Additionally, the heterogeneous chemotherapy regimens constitute a limitation of the study.
Conclusion
Although the follow-up time in the SIB-VMAT group was shorter than that in the 3D–CRT group, the rate of pCR did not increase significantly even when using the SIB-VMAT method. The SIB-VMAT method marginally improved the rate of pathological grade 2–3 effects and the OS was significantly better in patients with grade 2–3 effects. The SIB-VMAT may be a promising method for preoperative CRT of rectal cancer.
Abbreviations
- 3D–CRT:
-
Three-dimensional conformal radiotherapy
- APR:
-
Abdominoperineal resection
- CEA:
-
carcinoembryonic antigen
- CPT-11:
-
Irinotecan
- CRT:
-
Chemoradiation therapy
- CTV:
-
clinical target volume
- DFS:
-
Disease-free survival
- GU:
-
genitourinary
- IGRT:
-
Image-guided radiation therapy
- ISR:
-
Intersphincteric resection
- LAR:
-
Low anterior resection
- LC:
-
Local control
- LV:
-
Leucovorin
- OS:
-
Overall survival
- PCR:
-
Pathologic complete response
- pRR:
-
Pathological response rate
- PSM:
-
Propensity score matching
- PTV:
-
Panning target volume
- RM:
-
Radial margin
- RT:
-
Radiation therapy
- SIB:
-
Simultaneous integrated radiation boost
- UFT:
-
Oral uracil/tegafur
- VMAT:
-
Volumetric modulated arc therapy
References
Schmoll HJ, Van Cutsem E, Stein A, Valentini V, Glimelius B, Haustermans K, et al. ESMO consensus guidelines for management of patients with colon and rectal cancer. a personalized approach to clinical decision making. Ann Oncol. 2012;23:2479–516.
Sauer R, Becker H, Hohenberger W, Rödel C, Wittekind C, Fietkau R, et al. German rectal cancer study group. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004;351:1731–40.
Bosset JF, Collette L, Calais G, Mineur L, Maingon P, Radosevic-Jelic L, , et al.; EORTC radiotherapy group trial 22921. Chemotherapy with preoperative radiotherapy in rectal cancer. N Engl J Med 2006; 355: 1114–1123.
Sainato A, Cernusco Luna Nunzia V, Valentini V, De Paoli A, Maurizi ER, Lupattelli M, et al. No benefit of adjuvant fluorouracil Leucovorin chemotherapy after neoadjuvant chemoradiotherapy in locally advanced cancer of the rectum (LARC): long term results of a randomized trial (I-CNR-RT). Radiother Oncol. 2014;113:223–9.
National Comprehensive Cancer Network Guidelines, Rectal Cancer, Version 3. 2017. https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf.
Gérard JP, Conroy T, Bonnetain F, Bouché O, Chapet O, Closon-Dejardin MT, et al. Preoperative radiotherapy with or without concurrent fluorouracil and leucovorin in T3-4 rectal cancers: results of FFCD 9203. J Clin Oncol. 2006;24(28):4620–5.
Picardi V, Macchia G, Guido A, Giaccherini L, Deodato F, Farioli A, et al. Preoperative chemoradiation with VMAT-SIB in rectal cancer: a phase II study. Clin Colorectal Cancer. 2017;16(1):16-22. doi:10.1016/j.clcc.2016.06.004. Epub 2016 Jun 23. PMID:27435759
Yamashita H, Takenaka R, Sakumi A, Haga A, Otomo K, Nakagawa K. Analysis of motion of the rectum during preoperative intensity modulated radiation therapy for rectal cancer using cone-beam computed tomography. Radiat Oncol. 2015;10:2.
Guillem JG, Cohen AM. Current issues in colorectal cancer surgery. Semin Oncol. 1999;26(5):505–13.
Lindsetmo RO, Joh YG, Delaney CP. Surgical treatment for rectal cancer: an international perspective on what the medical gastroenterologist needs to know. World J Gastroenterol. 2008;14(21):3281–9.
Watanabe T, Itabashi M, Shimada Y, Tanaka S, Ito Y, Ajioka Y, et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) Guidelines 2014 for treatment of colorectal cancer. Int J Clin Oncol. 2015;20(2):207–39. Published online 2015 Mar 18. doi:10.1007/s10147-015-0801-z.
Fokas E, Liersch T, Fietkau R, Hohenberger W, Beissbarth T, Hess C, et al. Tumor regression grading after preoperative chemoradiotherapy for locally advanced rectal carcinoma revisited: updated results of the CAO/ARO/AIO-94 trial. J Clin Oncol 2014; 32: 1554-1562. doi: 10.1200/JCO.2013.54.3769. http://www.R-project.org/. PMID: 24752056.
Cotte E, Passot G, Decullier E, Maurice C, Glehen O, François Y, et al. Pathologic response, when increased by longer interval, is a marker but not the cause of good prognosis in rectal cancer: 17-year follow-up of the Lyon R90-01 randomized trial. Int J Radiat Oncol Biol Phys. 2016;94:544–53.
Francois Y, Nemoz CJ, Baulieux J, Vignal J, Grandjean JP, Partensky C, et al. Influence of the interval between preoperative radiation therapy and surgery on downstaging and on the rate of sphincter-sparing surgery for rectal cancer: the Lyon R90-01 randomized trial. J Clin Oncol. 1999;17:2396.
Huntington CR, Boselli D, Symanowski J, Hill JS, Crimaldi A, Salo JC. Optimal timing of surgical resection after radiation in locally advanced rectal adenocarcinoma: an analysis of the national cancer database. Ann Surg Oncol. 2016;23:877–87.
Tulchinsky H, Shmueli E, Figer A, Klausner JM, Rabau M. An interval >7 weeks between neoadjuvant therapy and surgery improves pathologic complete response and disease-free survival in patients with locally advanced rectal cancer. Ann Surg Oncol. 2008;15:2661–7.
Park IJ, You YN, Agarwal A, Skibber JM, Rodriguez-Bigas MA, Eng C, et al. Neoadjuvant treatment response as an early response indicator for patients with rectal cancer. J Clin Oncol. 2012;30:1770–6. doi: 10.1200/JCO.2011.39.7901. PMID: 22493423 PMCID: PMC3383178
Gérard JP, Azria D, Gourgou-Bourgade S, et al. Comparison of two neoadjuvant chemoradiotherapy regimens for locally advanced rectal cancer: results of the phase III trial ACCORD 12/405-Prodige 2. J Clin Oncol. 2010;28:1638–44.
Russell MM, Ganz PA, Lopa S, Yothers G, Ko CY, Arora A, Atkins JN, Bahary N, Soori GS, Robertson JM, Eakle J, Marchello BT, Wozniak TF, Beart RW Jr, Wolmark N. Comparative effectiveness of sphincter-sparing surgery versus abdominoperineal resection in rectal cancer: patient-reported outcomes in National Surgical Adjuvant Breast and Bowel Project randomized trial R-04. Ann Surg. 2015;261(1):144-8. PMID:24670844 PMCID:PMC4379325 doi:10.1097/SLA.0000000000000594.
Rödel C, Graeven U, Fietkau R, Hohenberger W, Hothorn T, Arnold D, et al. Oxaliplatin added to fluorouracil-based preoperative chemoradiotherapy and postoperative chemotherapy of locally advanced rectal cancer (the German CAO/ARO/AIO-04 study): final results of the multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2015;16:979–89.
Jiao D, Zhang R, Gong Z, Liu F, Chen Y, Yu Q, et al. Fluorouracil-based preoperative chemoradiotherapy with or without oxaliplatin for stage II/III rectal cancer: a 3-year follow-up study. Chin J Cancer Res. 2015;27:588–96.
O'Connell MJ, Colangelo LH, Beart RW, Petrelli NJ, Allegra CJ, Sharif S, et al. Capecitabine and oxaliplatin in the preoperative multimodality treatment of rectal cancer: surgical end points from National Surgical Adjuvant Breast and Bowel Project trial R-04. J Clin Oncol. 2014;32:1927–34.
Allegra CJ, Yothers G, O'Connell MJ, Beart RW, Wozniak TF, Pitot HC, et al. Neoadjuvant 5-FU or Capecitabine plus radiation with or without oxaliplatin in rectal cancer patients: a phase iii randomized clinical trial. J Natl Cancer Inst. 2015;107(11):djv248. doi:10.1093/jnci/djv248. Print 2015 Nov. Erratum in: J Natl Cancer Inst. 2016;108(4):djw057. doi:10.1093/jnci/djw057. PMID:26374429.
An X, Lin X, Wang FH, Goodman K, Cai PQ, Kong LH, et al. Short term results of neoadjuvant chemoradiotherapy with fluoropyrimidine alone or in combination with oxaliplatin in locally advanced rectal cancer: a meta analysis. Eur J Cancer. 2013;49(4):843-51. doi:10.1016/j.ejca.2012.09.026. Epub 2012 Oct 11.
De Felice F, Benevento I, Magnante AL, Musio D, Bulzonetti N, Caiazzo R, Tombolini V. Clinical benefit of adding oxaliplatin to standard neoadjuvant chemoradiotherapy in locally advanced rectal cancer: a meta-analysis : Oxaliplatin in neoadjuvant treatment for rectal cancer. BMC Cancer. 2017;17(1):325.
Nagtegaal ID, Quirke P. What is the role for the circumferential margin in the modern treatment of rectal cancer? J Clin Oncol. 2008;26(2):303–12.
Fokas E, Liersch T, Fietkau R, Smith KD, Tan D, Das P, et al. Clinical significance of acellular mucin in rectal adenocarcinoma patients with a pathologic complete response to preoperative chemoradiation. Ann Surg. 2010;251(2):261–4.
Silberfein EJ, Kattepogu KM, Hu CY, Skibber JM, Rodriguez-Bigas MA, Feig B, et al. Long-term survival and recurrence outcomes following surgery for distal rectal cancer. Ann Surg Oncol. 2010;17(11):2863–9.
Patel UB, Taylor F, Blomqvist L, George C, Evans H, Tekkis P, et al. Magnetic resonance imaging-detected tumor response for locally advanced rectal cancer predicts survival outcomes: MERCURY experience. J Clin Oncol. 2011;29(28):3753–60.
Engels B, Platteaux N, Van den Begin R, Gevaert T, Sermeus A, Storme G, et al. Preoperative intensity-modulated and image-guided radiotherapy with a simultaneous integrated boost in locally advanced rectal cancer: report on late toxicity and outcome. Radiother Oncol. 2014;110(1):155–9.
Bosset JF, Collette L, Calais G, et al. Chemotherapy with preoperative radiotherapy in rectal cancer. N Engl J Med. 2006;355:1114–23.
Aschele C, Cionini L, Lonardi S, et al. Primary tumor response to preoperative chemoradiation with or without oxaliplatin in locally advanced rectal cancer: pathologic results of the STAR-01 randomized phase III trial. J Clin Oncol. 2011;29:2773–80.
Glynne-Jones R, Hughes R. Complete response after chemoradiotherapy in rectal cancer (watch-and-wait): have we cracked the code? Clin Oncol (R Coll Radiol). 2016;28(2):152–60.
Matsusaka S, Ishihara S, Kondo K, Horie H, Uehara K, Oguchi M, et al. A multicenter phase II study of preoperative chemoradiotherapy with S-1 plus oxaliplatin for locally advanced rectal cancer (SHOGUN trial). Radiother Oncol. 2015;116(2):209–13.
Engels B, De Ridder M, Tournel K, et al. Preoperative helical tomotherapy and megavoltage computed tomography for rectal cancer: impact on the irradiated volume of small bowel. Int J Radiat Oncol Biol Phys. 2009;74:1476–80.
Tournel K, De Ridder M, Engels B, et al. Assessment of intrafractional movement and internal motion in radiotherapy of rectal cancer using megavoltage computed tomography. Int J Radiat Oncol Biol Phys. 2008;71:934–9.
Engels B, Tournel K, Everaert H, et al. Phase II study of preoperative helical tomotherapy with a simultaneous integrated boost for rectal cancer. Int J Radiat Oncol Biol Phys. 2012;83:142–8.
Sauer R, Liersch T, Merkel S, et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J Clin Oncol. 2012;30:1926–33.
Bujko K, Nowacki MP, Nasierowska-Guttmejer A, et al. Long-term results of a randomized trial comparing preoperative short-course radiotherapy with preoperative conventionally fractionated chemoradiation for rectal cancer. Br J Surg. 2006;10:1215–23.
Hall EJ, Wu C-S. Radiation-induced second cancers: the impact of 3D-CRT and IMRT. Int J Radiat Oncol Biol Phys. 2003;56:83–8.
Berrington de Gonzalez A, Curtis RE, Kry SF, et al. Proportion of second cancers attributable to radiotherapy treatment in adults: a cohort study in the US SEER cancer registries. Lancet Oncol. 2011;12:353–60.
Birgisson H, Pahlman L, Gunnarsson U, Glimelius B. Occurrence of second cancers in patients treated with radiotherapy for rectal cancer. J Clin Oncol. 2005;23:6126–31.
van Gijn W, Marijnen CA, Nagtegaal ID, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-years follow-up of the multicentre, randomised controlled TME trial. Lancet Oncol. 2011;12:575–82.
Acknowledgements
Not applicable.
Funding
This study was not funded by any organizations or companies.
Availability of data and materials
Raw data may be available on request from the corresponding author.
Author information
Authors and Affiliations
Contributions
Conception and design of the study: HY Acquisition of data: HY, SI, and KO Analysis and interpretation of the data: HY and SI Writing and revision of the manuscript: HY, HN, KK, TK, OA, TW, and KN. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The present study was approved by Institutional Review Board (IRB) of University of Tokyo Hospital (IRB number: 3372–3).
Consent for publication
Not applicable because this analysis has retrospective nature.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Yamashita, H., Ishihara, S., Nozawa, H. et al. Comparison of volumetric-modulated arc therapy using simultaneous integrated boosts (SIB-VMAT) of 45 Gy/55 Gy in 25 fractions with conventional radiotherapy in preoperative chemoradiation for rectal cancers: a propensity score case-matched analysis. Radiat Oncol 12, 156 (2017). https://doi.org/10.1186/s13014-017-0894-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13014-017-0894-9