
Abstract
Background
Knowledge of health-related quality of life (HRQOL) of patients receiving opioid substitution treatment (OST) is limited and fragmented. The present study examines the HRQOL of a large national sample of OST patients in Germany and sociodemographic and clinical correlates.
Methods
Cross-sectional data on the HRQOL of 2176 OST patients was compared with German general population norms. Patients were recruited from 63 OST practices across Germany. To identify correlates of HRQOL, as measured with the SF-12, we performed bi- and multivariate analyses with sociodemographic and clinical variables, including patient- and clinician-reported outcomes on physical and mental health.
Results
Patients’ HRQOL was significantly poorer than in the general population, especially their mental HRQOL. Factors associated with lower physical HRQOL were older age, longer duration of opioid dependence, hepatitis C virus infection, and HIV infection. Benzodiazepine use was associated with lower mental HRQOL, and amphetamine use with higher physical HRQOL, compared to non-use of these substances. For both mental and physical HRQOL, the factor with the strongest positive association was employment and the factors with the strongest negative associations were physical and mental health symptom severity, psychiatric diagnosis, and psychopharmacological medication.
Conclusions
Compared to the general population, we found substantially lower HRQOL in OST patients, especially in their mental HRQOL. OST programs can benefit from further improvement, particularly with regard to mental health services, in order to better serve their patients’ needs. Clinicians may consider the use of patient-reported outcome measures to identify patients’ subjective physical and psychological needs. Further research is needed to determine if employment is a cause or consequence of improved HRQOL.
Trial registration
ClinicalTrials.gov: NCT02395198, retrospectively registered 16/03/2015
Similar content being viewed by others

Background
Opioid substitution treatment (OST) is an evidence-based intervention for opioid dependence that improves patients’ health and reduces the mortality rate [1,2,3]. The proportion of people who inject drugs (PWID) who receive OST varies greatly between countries. While coverage is estimated to be greater than 40 OST recipients per 100 PWID in western Europe and Australia, estimates for the USA, China, India, and Eastern Europe vary between 1 and 20 OST recipients per 100 PWID, and in most parts of the world OST is still not even available [4]. There are also large differences in sociodemographic and drug use characteristics in PWID worldwide. For example, PWID who are younger than age 25 make up less than 20% of PWID in North America, Australasia, Central Asia, and the Caribbean, but more than 40% of PWID in Eastern Europe and Latin America [5]. In Europe, the proportion of patients aged over 40 entering treatment for opioid use increased from 1 in 5 in 2006 to 1 in 3 in 2013 [6, 7]. This reflects an ageing cohort of opioid users who started injecting during the heroin “epidemics” of the 1980s and 1990s and who have shaped and characterized the current European treatment systems [6, 7]. A steadily increasing age of the OST population is also observed in many other regions in the world with a longer history of OST implementation, such as New York City [8] and Australia [9]. Thus, long-term OST patients are getting older and few young people are entering OST. An ageing population places increasing demands on the health care system [10, 11]. Especially the next two decades will pose a challenge, as the large cohorts of opioid users who initiated use in the eighties and nineties are growing old.
Understanding the needs of OST patients is critical to providing the right care. Health-related quality of life (HRQOL) is a valuable outcome measure in this regard. It is a concept that includes subjective physical and mental wellbeing, and can be useful in the evaluation of treatment programs and patient progress by providing insight from the patient’s perspective. [12].
Over the past two decades, there has been an increasing interest in the HRQOL of OST patients. Research consistently shows that OST patients’ HRQOL is significantly lower at treatment entry compared to the general population or people with psychiatric disorders [10, 13,14,15] and that HRQOL improves in the first months of OST [16,17,18,19]. However, comparatively little is known about the HRQOL of long-term OST patients. A few cross-sectional studies suggest that OST patients continue to have poor HRQOL in OST, but these studies are limited by small sample sizes and partially conflicting outcomes [10, 13, 20, 21]. Only Wittchen et al. (2011) assessed the HRQOL of a large sample of OST patients – although only as a secondary outcome – and found significantly lower HRQOL compared to the general population and no improvements over a one-year period [22].
In fact, while HRQOL improves at treatment uptake, the effect seems short-lived. Wang et al. (2012) conducted an 18-month study in which they assessed quality of life (QOL) every 3 months [23]. They found that QOL improved rapidly in the first 3 months of OST, but then the effect slowed down. Likewise, Ponizovsky et al. (2007) detected an improvement of QOL only in the first month of OST [24]. Habrat et al. (2002) demonstrated that while HRQOL improved significantly the first 6 months of OST, it then decreased again [25]. Karow et al. (2011) found that QOL increased more during the first 6 months of OST than the following 6 months and that it did not reach the level of healthy individuals [15]. Taken together, the literature suggests that OST is effective in enhancing QOL and HRQOL at treatment entry but may have shortcomings in the long-term.
Understanding the needs of subgroups of patients is essential to be able to provide appropriate care. Research consistently shows that female OST patients have poorer overall HRQOL than male patients [15, 21]. However, some studies found an association of gender with mental HRQOL, some with physical HRQOL, and others with both physical and mental HRQOL or neither [20, 26,27,28,29]. Similarly, there is conflicting evidence with regard to other factors, such as active drug use and hepatitis C virus (HCV) infection [13, 15, 30,31,32]. The present study aims to provide the first comprehensive data on the HRQOL of a large national sample of patients in OST including sociodemographic and clinical correlates.
Methods
Study design
This investigation is part of the larger study ‘Epidemiology Of Hepatitis C Virus Infection Among People Receiving Opioid Substitution Therapy (ECHO)’, an observational longitudinal multicentre study, which aims to estimate the national prevalence and incidence of HCV infection among OST patients in Germany. Stratified random sampling was performed to obtain a representative sample of OST clinicians based on their distribution according to German Federal State and the number of patients per clinician. For patients to be eligible to participate in the study they had to be diagnosed with opioid dependence according to the ICD-10, be currently in OST, be at least 18 years of age, and have sufficient German literacy skills. Patients were eligible to participate with any form of OST (e.g. liquid, pills, capsules) and any type of OST medication (e.g. methadone, buprenorphine, pharmaceutical heroin). OST physicians invited their patients to participate in the study; participation was voluntary and remuneration was provided. Once patients completed the questionnaire, they placed it in an envelope and sealed it so that physicians could not access the data. The study design is described in full detail elsewhere [33]. Ethical approval for the ECHO study was granted by the Ethics Committee of the Medical Association of Hamburg, Ref. PV4603, and by each local Ethics Committee in Germany.
Study sample
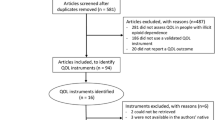
From July 2014 to October 2016, epidemiological cross-sectional data was collected from a large national sample of 2474 outpatients receiving OST from 63 OST clinicians in Germany. A good regional distribution of clinicians across Germany was obtained, although smaller clinics were somewhat underrepresented in our sample. Of the 2474 patients, a total of 298 (12.1%) were excluded because they did not fill in the patient questionnaire (N=239, 9.7%) or because the HRQOL instrument had more than two missing values per participant (N=59, 2.4%; [34]). Of the final 2176 patients included in the analyses, clinician data was not available for 79 patients.
Measures
HRQOL was measured with the 12-Item Short Form Health Survey (SF-12; [35,36,37]). The 12 items are a subset of the 36-item Short Form Health Survey (SF-36; [38]), and assess subjective functional health and wellbeing (e.g. “Does your health limit you in climbing several flights of stairs? If so, how much?” or “In the past week, how often were you calm and relaxed?”). Physical and Mental Component Summary Scores (PCS and MCS) are calculated. We chose the SF-12 because it is one of the most widely used HRQOL instruments in the addiction literature [39, 40] and because country-specific general population norms are available for it [36]. Good psychometric properties of PCS and MCS are reported for both the original American version and the German version used in this study (e.g. test-retest (2-week) correlations of 0.89 and 0.76 [37], and internal consistency (Cronbachs alpha) > .70 [36]). The SF-12 has a high construct validity in discriminating between patient groups known to differ in physical and mental conditions, and it is also sensitive to change [36, 37]. Correlations between the 12-item and the 36-item PCS and MCS are very high, ranging from 0.94–0.96 for PCS and 0.94–0.97 for MCS across different countries and languages [35].
Patients and clinicians completed questionnaires independently from one another.
Patients provided sociodemographic data (gender, age, employment, children, relationship, housing, and migration background) and completed the SF-12, the Brief Symptom Inventory-18 (BSI-18; [41]), and the Opiate Treatment Index Health Symptoms Scale (OTI-HSS; [42, 43]). The BSI-18 is a self-report measure of psychological distress, comprising a symptom checklist and yielding three sub-scores (Depression, Anxiety, and Somatization), as well as the Global Severity Index (GSI). The OTI-HSS is a self-report measure of physical health, comprising a checklist of 50 symptoms that opioid users often experience.
Clinicians provided clinical data (duration of current OST, substitution medication, years of opioid dependence, active drug use, HCV infection, human immunodeficiency virus (HIV) infection, psychiatric diagnosis, and psychopharmacological medication during the past 6 months) and rated patients’ functioning and illness severity using the Global Assessment of Functioning scale (GAF; [44]) and the Clinical Global Impression scale (CGI; [45]). Active drug use was defined as the consumption of at least one illegal substance (cocaine, benzodiazepines, heroin or amphetamine) once during the past three months. The last three urine samples from the past three months were tested for the four substances, thus creating 12 possible data sets per patient. Information on psychiatric diagnosis and psychopharmacological medication, as well as HCV and HIV status, was taken from the patients’ medical records. Clinicians were encouraged to perform HCV diagnoses in accordance with the German HCV testing-guidelines (i.e. yearly antibody tests for patients with negative serostatus). However, due to the non-interventional nature of our study, clinicians were not obliged to do this. The time of testing was therefore individual for each participant.
Statistical Analysis
We calculated the two component summary scales of the SF-12 (PCS and MCS) in accordance with the German test manual [36], using US-derived item weights. Up to two missing values per participant were imputed in the SF-12 (method proposed by Perneger et al. [34]). Participants with more than 2 missing items were excluded from analysis. To compare the SF-12 scores of our sample with the general population, we calculated independent sample t-tests using PCS/MCS means, standard deviations and sample sizes of the German normative sample from 1998 [36]. In addition, we determined the percentages of patients scoring lower or higher than one standard deviation below or above the German general population mean. Bivariate associations between PCS/MCS and our variables of interest were assessed using Pearson’s correlations for continuous variables (e.g. age, BSI-18), independent samples t-tests for dichotomous variables (e.g. gender), and one-way ANOVAs for categorical outcomes (e.g. partnership, age groups). For each statistically significant association, we determined effect sizes (standardized mean difference (d) and partial eta2). In addition, we calculated multiple linear regression models to predict PCS and MCS based on sociodemographic and clinical characteristics. We included the variables gender, duration of opioid dependence, employment, living together with children, relationship, migration background, percentage of positive urine samples, duration of current OST, HIV status, and HCV status. The variables were selected based on considerations of relevance and multicollinearity. We first included all sociodemographic and clinical variables (Table 1) in one regression model (simultaneous entry), and then removed predictors that were either redundant in content or demonstrated intercorrelations higher than r = .6.
Results
Sample characteristics
Respondents (N = 2176) were predominantly male (72.2%) with a mean age of 41.8 (± 8.94) years. They were opioid dependent for an average of 20.4 (± 9.11) years and in their current OST for an average of 6.3 (±5.21) years. Of the total sample, 83.1% reported stable housing, 52.4% had children, 44.8 % were in a relationship, 34.5% were employed, and 23.8% had a migration background. Most respondents received methadone (76.6%), followed by buprenorphine (22.6%) and other substitution medications (0.8%). Moreover, 27.2% of participants were HCV-RNA positive, 3.7% were HIV-positive, and 2.2% were HCV/HIV co-infected. Thirty-six percent had consumed drugs within the past 12 weeks (Table 1).
To test for selection bias, we compared sample characteristics of the 2176 included patients with the 298 non-included patients, using data provided by the clinicians. Significant differences but with small effect sizes (around d = 0.3) emerged between the included and the non-included sample in (non-German) citizenship (10.0% vs. 18.9%), mean GAF ratings (65.7 ± 18.8 vs. 59.7 ± 19.1), mean CGI-S ratings (2.9 ± 1.6 vs. 3.5 ± 1.6), and past 4 weeks benzodiazepine use (15.7% vs. 23.9%). Only very small differences (d < 0.3) were found in age, gender, duration of current OST, and CGI-I ratings. No differences were found in psychiatric diagnosis, psychopharmacological medication, substitution medication, duration of opioid dependence, and use of heroin, cocaine or amphetamine.
HRQOL of OST patients compared to the German normative sample
OST patients had a mean PCS of 44.63 (SD 9.75, range 11.04 - 64.08) and a mean MCS of 41.76 (SD 11.40, range 10.83 - 69.06; Table 2). Respondents scored significantly lower on the PCS than the German normative sample (M = 48.22, SD = 8.77; t(8850) = -15.270, p<0.001, d = -0.40). This effect was even more pronounced for the MCS (M = 51.41, SD = 8.55; t(8850) = -36.275, p<0.001, d = -1.03).
The distributions of PCS and MCS scores in our sample are not bell-shaped. The PCS distribution is left-skewed, with a peak at about 55 points (Fig. 1). The MCS has a bimodal distribution with peaks at about 30 and 55 points (Fig. 2). For PCS, 30.4% of patients scored lower than one standard deviation (SD) below the German normative sample mean and 5.9% of patients scored higher than one SD above the mean (Fig. 1). For MCS, 51.7% of patients scored lower than one SD below the German normative sample mean and 1.8% of patients scored higher than one SD above the mean (Fig. 2). Regarding PCS and MCS together, 1362 patients (62.6% of the total sample) scored lower than one SD in at least one scale and, of this group, 425 patients (19.5% of the total sample) scored lower than one SD in both scales.

Distribution of the SF-12 Physical Component Summary score (PCS) compared with German general population norms. ECHO study sample (n = 2176) statistics: mean = 44.63, standard deviation = 9.75, range 11.04 – 64.08; skewness = -0.50, SE = 0.05; kurtosis = -0.56

Distribution of the SF-12 Mental Component Summary score (MCS) compared with German general population norms. ECHO study sample (n = 2176) statistics: mean = 41.76, standard deviation = 11.40, range 10.83 – 69.06; skewness = -0.18, SE = 0.05; kurtosis = -0.95
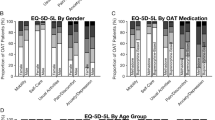
Both male and female OST patients had lower SF-12 scores than the general population (Men PCS 44.58 ± 9.61 vs. 49.12 ± 8.20, d = -0.52; Men MCS 42.29 ± 11.13 vs. 52.54 ± 7.81, d = -1.14; Women PCS 44.79 ± 10.10 vs. 47.34 ± 9.19, d = -0.54; Women MCS 40.39 ± 11.98 vs. 50.30 ± 9.08, d = -1.07; all p <.001). Moreover, SF-12 scores were lower in all age groups compared to the general population (Fig. 3).

SF-12 scores by age groups, compared with the German general population. Means and standard errors of A: Physical Component Summary scores (PCS) and B: Mental Component Summary scores (MCS) by age groups for the study sample of OST patients (n = 2176) and the German normative sample (n = 6676)
Sociodemographic and clinical correlates of HRQOL in OST patients
Bivariate associations of sociodemographic and clinical variables with SF-12 scores are shown in Table 3. Relevant associations (effect sizes d > 0.35, r > 0.2, partial eta 2 > 0.04; Ferguson, 2009 [46]) are described first. Older age, longer duration of opioid dependence, methadone as substitution medication, HCV infection, and HIV infection were associated with lower PCS. Having a psychiatric diagnosis, being in psychopharmacological treatment, and current drug use were associated with lower MCS. Although, more specifically, only benzodiazepine use was associated with lower MCS, while amphetamine use was associated with higher PCS (no association with heroin or cocaine use). Unemployment was associated with lower PCS and MCS.
Other significant associations but with very small effect sizes emerged (d < 0.35, r < 0.2, partial eta 2 < 0.04). Women exhibited slightly lower MCS than men, patients receiving methadone had lower MCS than those receiving buprenorphine, and patients with HCV infection had slightly lower MCS than those without. Psychiatric diagnosis, psychopharmacological treatment, longer duration of current OST and migration background was weakly associated with lower PCS. There was also a very small association between drug use and lower PCS. More specifically, only amphetamine use and benzodiazepine use was associated with lower PCS (and not the other two substances we measured, heroin and cocaine). Being in a relationship and living in stable housing was associated with slightly higher PCS and MCS. Participants who lived together with their children had slightly higher PCS and MCS than those who did not.
In the multivariate models (n = 1703; Table 4), higher PCS was predicted by (highest regression weights mentioned first) stable employment, shorter duration of opioid dependence, negative HCV status, the absence of a psychiatric diagnosis, and being substituted with buprenorphine. Higher MCS was predicted by (highest regression weights mentioned first) the absence of a psychiatric diagnosis, stable employment, not being in psychopharmacological treatment, less drug use, male gender, being substituted with buprenorphine and living together with children. As 473 patients were excluded from the multivariate model due to missing values, we checked for possible selection bias. The 1703 patients included in the regression model were slightly younger (41.5 years (± 8.8) vs. 42.9 (± 9.3) years, p = .004), reported less physical impairments (better PCS and BSI somatization subscale), were slightly longer in their current OST, and had higher CGI-I ratings (all differences d < .2). No differences in other variables emerged.
HRQOL and measures of physical and mental health
Better self-reported mental health (BSI-18) correlated moderately with better PCS (r = -.41) and strongly with better MCS (r = -.67). More specifically, the BSI-18 subscale Somatization correlated moderately with PCS and MCS, while the subscales Depression and Anxiety correlated weakly with PCS and strongly with MCS. The OTI-HSS score correlated moderately with PCS (r = -.48) and MCS (r = -.50), such that participants with a higher OTI-HSS score demonstrated lower PCS and MCS (Table 3). Clinicians’ ratings of patients’ mental illness severity (CGI-S: M=2.91, SD=1.59, range 1-7) and functioning (GAF: M=65.72, SD=18.81, range 0-100) were weakly correlated with patients’ self-reported physical and mental HRQOL (Table 2 and 3).
Discussion
This study presents a comprehensive and differentiated assessment of the physical and mental HRQOL of a large national sample of OST patients in Germany. Substantial impairments were found in OST patients’ HRQOL, especially in their mental HRQOL. However, there was also a smaller subgroup of patients with considerably better HRQOL than the rest of the sample, indicating that it is possible for patients to attain a relatively good HRQOL. This suggests that there is room for improvement in OST programs, particularly relating to patients’ mental wellbeing.
Our findings may inform tailored interventions for subgroups of patients and have implications for drug policies. For example, age was one of the most important correlates of poor physical HRQOL, suggesting that older OST patients may benefit from enhanced health care services. Moreover, the association of chronic HCV infection with low physical HRQOL highlights the importance of providing antiviral HCV treatment to OST patients. Many clinicians still hesitate to provide HCV treatment to drug users, because they fear reinfection or non-adherence to treatment, and also drug-users are frequently unwilling to take up HCV treatment [47]. However, especially in this new era of direct-acting antiviral (DAA) treatment with reduced side effects and high rates of sustained virologic response (SVR), it is important to reduce the barriers to HCV diagnosis and treatment and to educate clinicians and patients about treatment benefits beyond SVR, such as increased subjective wellbeing and reduced symptoms of extra-hepatic manifestations [48, 49]. While it makes sense that older age, HCV and HIV infection are associated with lower physical HRQOL, it should be noted that these factors have a greater impact on drug users than non-drug users [50, 51], highlighting the need for additional support specifically for older drug users.
While OST briefly improves mental health outcomes at the beginning of treatment [52], it does not appear to address patients’ mental health adequately in the long run. Opioid dependent individuals have high levels of psychiatric symptoms [22, 53]. Past-year prevalence estimates of co-occurring psychiatric disorders range between 30% and 50% for mood disorders (e.g. depression) and 10% to 20% for anxiety disorders [54, 55]. However, our study and a recent 6-year follow up cohort study demonstrate that this high psychiatric comorbidity persists in long-term OST patients [56]. More than half of the patients in our sample had at least one psychiatric diagnosis. This is an important finding, because patients with dual diagnosis face barriers to adequate mental health treatment, including insufficient cooperation between mental and medical health institutions and the under-identification of dual diagnosis, which is in part due to the lack of mental health training in physicians [57,58,59]. As our study finds that psychiatric diagnosis and psychopharmacological treatment are associated with both mental and physical HRQOL, one may argue that it is particularly important to address OST patients’ mental health, as it is not only associated with mental but also physical wellbeing.
Gender was only weakly associated with HRQOL. This may explain the mixed findings in the literature from smaller studies, which show associations of gender with mental or physical HRQOL or neither or both [15, 20, 21, 26,27,28,29]. Similarly, there were mixed findings in the literature on the association of HRQOL with active drug use. Our results show that only benzodiazepine and amphetamine use was associated with HRQOL and not heroin or cocaine use. Benzodiazepine users might be self-medicating, considering that they often have a more complicated course of OST and exhibit more poly drug use [60]. Moreover, the regular and long-term use of benzodiazepines itself reduces quality of life and has adverse effects like cognitive or psychomotor impairment [61, 62].
While we found an association of HRQOL with substitution medication, the differences between methadone and buprenorphine are likely confounded with other factors that correlate with buprenorphine prescription, such as age, duration of opioid dependence, and preexisting physical and mental health. Buprenorphine is less sedating than methadone, but it is also more often prescribed to younger and more stable patients. The complexity of these interrelations needs to be considered when interpreting the results, and is also reflected in the multivariate model where the association between OST medication and HRQOL becomes much smaller when controlling for the above-mentioned factors.
In the multivariate model, we only included sociodemographic and clinical predictors, because bivariate associations of PCS and MCS with self-reported physical and mental health were already demonstrated. Consequently, the percentage of variance explained was relatively low (21% for PCS, 18% for MCS), which is however not surprising, given that HRQOL is influenced by a range of factors that cannot all be measured in a study. With regard to a potential selection bias that may have resulted from the listwise inclusion in our multivariate analyses, we consider the subsample included in the regression models highly representative for the total sample; differences in age and health are only marginal and no other relevant differences emerged. Results of bivariate and multivariate analyses are highly comparable. The most important bivariate correlations were also found as predictors in the multivariate model, and the relative importance of each predictor (expressed by standardized beta weights) reflects the effect sizes determined via bivariate comparisons. The most important predictors for both PCS and MCS were employment and mental health, followed by duration of opioid dependence for PCS.
Another interesting observation is that, even though patients and clinicians provided ratings for HRQOL and functioning independently, the scores correlated. Patients’ self-reported mental and physical HRQOL correlated with clinician-rated patient functioning (GAF) and clinician-rated mental illness severity (CGI-S) (Table 3). The literature often reports a discrepancy between the perspectives of patients and clinicians [63, 64], but our findings suggest that in patients with an opioid use disorder, clinicians’ ratings of functioning and mental illness severity are good indicators of patients’ HRQOL.
HRQOL correlated with patient-reported measures of physical and mental health. These “cross-over” associations between the physical and mental domains (i.e. MCS with OTI-HSS, and PCS with BSI-18) suggest that there is not a strict division between physical and mental health with regard to their impact on a person’s subjective wellbeing. Nevertheless, brief symptom-based psychiatric screening tools should be implemented more regularly in clinical practice, given the high prevalence of mood and anxiety disorders in the opioid dependent population. Systematic screening for depression and anxiety, including in newly admitted patients, can reduce under-identification of comorbid disorders, which is a structural barrier to mental health treatment [58, 65]. Practitioners should use instruments with good validity for drug using populations, such as the BSI-18 [66].
As our study had a cross-sectional design, we could not determine if unemployment was a cause or consequence of poor HRQOL. Considering unemployment status was the most important factor correlating with HRQOL, future research should investigate this relationship further. Moreover, longitudinal studies could evaluate the effects of work rehabilitation programs on OST patients’ HRQOL, and qualitative studies could investigate patients’ perspectives and needs with regard to employment and HRQOL. It is also important to clarify if and how re-integration in the labor market is a reasonable treatment goal for opioid dependent patients. So far, in Germany, work rehabilitation plays virtually no role in OST in practice [67].
A limitation of this study is its possible selection bias. Due to missing or incomplete patient questionnaires, 358 patients (14.5%) had to be excluded. Differences between the included and excluded samples were small, although it is worth noting that excluded patients had greater impairments in (clinician-reported) mental health and functioning, meaning the HRQOL of this study sample might be higher than that of the actual overall population of OST patients. A second limitation is the interpretation and validity of our drug use and treatment variables. As we collected routine data, which differed between study sites, the frequency of urine sampling and the substances that were tested varied between OST practices. Moreover, we did not record which patients were prescribed benzodiazepine, so that we cannot distinguish between prescribed and non-prescribed benzodiazepine use. We also did not keep track of what other interventions or services the participants were using and suggest that future research explores their additional impact on HRQOL. A third limitation is that we used data from the German normative sample from 1998. However, (a) the HRQOL of the German general population has improved since 1998, especially in individuals over the age of 50 [68], and (b) our sample is about 4 years younger and includes more men than the German general population and SF-12 norm samples [69, 70]. This is important, because younger age and male gender are associated with better HRQOL [68]. Therefore, if we compared our sample of OST patients to a more recent norm sample with younger and more male individuals, there would be an even bigger difference in HRQOL scores.
This study highlights the need for more patient-centered care. Rather than just focusing on clinical symptoms, we should also measure the subjective experiences and needs of OST patients to be able to provide more effective and patient-oriented interventions and care. HRQOL is a useful patient-reported outcome measure in this regard. Given the high comorbidity of opioid dependence and given that diseases and symptoms are burdensome to different degrees to different people, a measure of subjective wellbeing is arguably a better indicator of patients’ needs than symptom-based instruments such as the BSI-18 and OTI-HSS. It should be noted that the SF-12 is a generic HRQOL instrument and may therefore not provide sensitive data on the HRQOL of OST patients. Future research should use a drug-user specific HRQOL instrument with items that are relevant and specific to OST patients.
The differences in mental and physical HRQOL of OST patients demonstrate the need to measure wellbeing in multiple life domains. However, also the concept of HRQOL is limited in its scope and future research should examine the broader concept of QOL for a more comprehensive understanding of patients’ wellbeing and a holistic approach to patient’s recovery. The concept of QOL goes beyond symptoms of physical and mental health and broadens the view on a person’s condition by including aspects such as social and economic participation. Given that opioid dependence is a complex chronic disease, the improvement of QOL is a more adequate treatment goal than the absence of symptoms. To monitor long-term treatment success, a short but reliable QOL instrument, such as the Opioid Substitution Treatment Quality of Life scale (OSTQOL, [71]) could be a useful tool for OST providers.
Conclusions
Compared to general population norms, we found substantially lower HRQOL in OST patients, especially in their mental HRQOL. Interestingly, our sample also comprised a considerable albeit smaller proportion of high-functioning OST patients with good physical and mental health, employment, stable housing, and/or stable family situation. However, the biggest proportion of OST patients had severe deficits in physical and mental health and HRQOL, suggesting that OST programs could benefit from further improvement to better serve their patients’ needs, particularly with regard to their mental health. An integrated health care approach is needed in which different physical and mental health care services are offered in combination, such as psychosocial support, therapy, and case management, as well as medical care specializing in the physical problems of opioid users. Moreover, more patient-centered care is needed to incorporate the patients’ perspectives and experiences in the treatment plan. Clinicians may consider the use of patient-reported outcome measures to enhance patient engagement in treatment.
Abbreviations
- BSI-18:
-
Brief Symptom Inventory-18
- CGI:
-
Clinical Global Impression
- ECHO:
-
Epidemiology Of Hepatitis C Virus Infection Among People Receiving Opioid Substitution Therapy
- GAF:
-
Global Assessment of Functioning
- GSI:
-
Global Severity Index
- HCV:
-
Hepatitis C Virus
- HIV:
-
Human Immunodeficiency Virus
- HRQOL:
-
Health-Related Quality Of Life
- MCS:
-
Mental Component Summary (composite of the 12-Item Short Form Health Survey)
- OST:
-
Opioid Substitution Treatment
- OTI-HSS:
-
Opiate Treatment Index - Health Symptoms Scale
- PCS:
-
Physical Component Summary (composite of the 12-Item Short Form Health Survey)
- QOL:
-
Quality Of Life
- SF-12:
-
12-Item Short Form Health Survey
- SVR:
-
Sustained Virologic Response
References
Degenhardt L, Bucello C, Mathers B, Briegleb C, Ali H, Hickman M, McLaren J. Mortality among regular or dependent users of heroin and other opioids: a systematic review and meta-analysis of cohort studies. Addiction. 2011;106(1):32–51.
Mattick RP, Breen C, Kimber J, Davoli M. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database Syst Rev. 2014;(2):CD002207.
WHO. WHO/UNODC/UNAIDS position paper : substitution maintenance therapy in the management of opioid dependence and HIV/AIDS prevention. Geneva: World Health Organization, United Nations Office on Drugs and Crimes, UNAIDS; 2004.
Larney S, Peacock A, Leung J, Colledge S, Hickman M, Vickerman P, Grebely J, Dumchev KV, Griffiths P, Hines L, et al. Global, regional, and country-level coverage of interventions to prevent and manage HIV and hepatitis C among people who inject drugs: a systematic review. Lancet Global Health. 2017;5(12):e1208–20.
Degenhardt L, Peacock A, Colledge S, Leung J, Grebely J, Vickerman P, Stone J, Cunningham EB, Trickey A, Dumchev K, et al. Global prevalence of injecting drug use and sociodemographic characteristics and prevalence of HIV, HBV, and HCV in people who inject drugs: a multistage systematic review. Lancet Global Health. 2017;5(12):e1192–207.
UNODC. World Drug Report 2018 (United Nations publication, Sales No. E.18.XI.9). Booklet 4: Drugs and Age: United Nations; 2018.
Ageing and addiction:challenges for treatment systems [http://www.emcdda.europa.eu/system/files/publications/3435/05_LXAddictions_AP_ageing_FINAL.pdf]. Accessed 12 Dec 2008.
Han B, Polydorou S, Ferris R, Blaum CS, Ross S, McNeely J. Demographic Trends of Adults in New York City Opioid Treatment Programs—An Aging Population. Subst Use Misuse. 2015;50(13):1660–7.
Searby A, Maude P, McGrath I. An Ageing Methadone Population: A Challenge to Aged Persons’ Mental Health Services? Issues Ment Health Nurs. 2015;36(11):927–31.
Rosen D, Smith ML, Reynolds CF 3rd. The prevalence of mental and physical health disorders among older methadone patients. Am J Geriatr Psychiatry. 2008;16(6):488–97.
Rosen D, Heberlein E, Engel RJ. Older adults and substance-related disorders: trends and associated costs. ISRN Addict. 2013;2013:905368.
Moons P, Budts W, De Geest S. Critique on the conceptualisation of quality of life: a review and evaluation of different conceptual approaches. Int J Nurs Stud. 2006;43(7):891–901.
Astals M, Domingo-Salvany A, Buenaventura CC, Tato J, Vazquez JM, Martin-Santos R, Torrens M. Impact of substance dependence and dual diagnosis on the quality of life of heroin users seeking treatment. Subst Use Misuse. 2008;43(5):612–32.
Calsyn DA, Saxon AJ, Bush KR, Howell DN, Baer JS, Sloan KL, Malte CA, Kivlahan DR. The Addiction Severity Index medical and psychiatric composite scores measure similar domains as the SF-36 in substance-dependent veterans: concurrent and discriminant validity. Drug Alcohol Depend. 2004;76(2):165–71.
Karow A, Verthein U, Pukrop R, Reimer J, Haasen C, Krausz M, Schafer I. Quality of life profiles and changes in the course of maintenance treatment among 1,015 patients with severe opioid dependence. Subst Use Misuse. 2011;46(6):705–15.
Karow A, Reimer J, Schafer I, Krausz M, Haasen C, Verthein U. Quality of life under maintenance treatment with heroin versus methadone in patients with opioid dependence. Drug Alcohol Depend. 2010;112(3):209–15.
Maremmani I, Pani PP, Pacini M, Perugi G. Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroin-addicted patients. J Subst Abuse Treat. 2007;33(1):91–8.
Raisch DW, Campbell HM, Garnand DA, Jones MA, Sather MR, Naik R, Ling W. Health-related quality of life changes associated with buprenorphine treatment for opioid dependence. Qual Life Res. 2012;21(7):1177–83.
Villeneuve PJ, Challacombe L, Strike CJ, Myers T, Fischer B, Shore R, Hopkins S, Millson P. Change in health-related quality of life of opiate users in low-threshold methadone programs. J Subst Use. 2006;11(2):137–49.
Bizzarri J, Rucci P, Vallotta A, Girelli M, Scandolari A, Zerbetto E, Sbrana A, Iagher C, Dellantonio E. Dual diagnosis and quality of life in patients in treatment for opioid dependence. Subst Use Misuse. 2005;40(12):1765–76.
Carpentier PJ, Krabbe PF, van Gogh MT, Knapen LJ, Buitelaar JK, de Jong CA. Psychiatric comorbidity reduces quality of life in chronic methadone maintained patients. Am J Addict. 2009;18(6):470–80.
Wittchen HU, Bühringer G, Rehm JT, Soyka M, Träder A, Trautmann S. The social, clinical and treatment situation of opioid maintenance treatment in a prevalence sample of patients at baseline. Suchtmedizin in Forschung und Praxis. 2011;13:227–37.
Wang PW, Wu HC, Yen CN, Yeh YC, Chung KS, Chang HC, Yen CF. Change in quality of life and its predictors in heroin users receiving methadone maintenance treatment in Taiwan: an 18-month follow-up study. Am J Drug Alcohol Abuse. 2012;38(3):213–9.
Ponizovsky AM, Grinshpoon A. Quality of life among heroin users on buprenorphine versus methadone maintenance. Am J Drug Alcohol Abuse. 2007;33(5):631–42.
Habrat B, Chmielewska K, Baran-Furga H, Keszycka B, Taracha E. Subjective Quality of Life in opiate-dependent patients before admission after six months and one-year participation in methadone program. Przeglad lekarski. 2002;59(4-5):351–4.
Korthuis PT, Tozzi MJ, Nandi V, Fiellin DA, Weiss L, Egan JE, Botsko M, Acosta A, Gourevitch MN, Hersh D, et al. Improved quality of life for opioid-dependent patients receiving buprenorphine treatment in HIV clinics. J Acquir Immune Defic Syndr (1999). 2011;56(Suppl 1):S39–45.
Millson P, Challacombe L, Villeneuve PJ, Strike CJ, Fischer B, Myers T, Shore R, Hopkins S. Determinants of health-related quality of life of opiate users at entry to low-threshold methadone programs. Eur Addict Res. 2006;12(2):74–82.
Preau M, Protopopescu C, Spire B, Sobel A, Dellamonica P, Moatti JP, Carrieri MP. Health related quality of life among both current and former injection drug users who are HIV-infected. Drug Alcohol Dependence. 2007;86(2-3):175–82.
Puigdollers E, Domingo-Salvany A, Brugal MT, Torrens M, Alvaros J, Castillo C, Magri N, Martin S, Vazquez JM. Characteristics of heroin addicts entering methadone maintenance treatment: quality of life and gender. Subst Use Misuse. 2004;39(9):1353–68.
Korthuis PT, Zephyrin LC, Fleishman JA, Saha S, Josephs JS, McGrath MM, Hellinger J, Gebo KA. Health-related quality of life in HIV-infected patients: the role of substance use. AIDS Patient Care STDS. 2008;22(11):859–67.
Miranda JF, Ga- Portilla MG, Martínez PS, Cienfuegos EG, García JB. Calidad de vida y severidad de la adicción en heroinómanos en mantenimiento prolongado con metadona. Adicciones. 1999;11:43–52.
Schäfer A, Wittchen HU, Backmund M, Soyka M, Golz J, Siegert J, Schafer M, Tretter F, Kraus MR. Psychopathological changes and quality of life in hepatitis C virus-infected, opioid-dependent patients during maintenance therapy. Addiction (Abingdon, England). 2009;104(4):630–40.
Strada L, Schulte B, Schmidt CS, Verthein U, Cremer-Schaeffer P, Kruckeberg S, Reimer J. Epidemiology of hepatitis C virus infection among people receiving opioid substitution therapy (ECHO): study protocol. BMC Infect Dis. 2015;15:563.
Perneger TV, Burnand B. A simple imputation algorithm reduced missing data in SF-12 health surveys. J Clin Epidemiol. 2005;58(2):142–9.
Gandek B, Ware JE, Aaronson NK, Apolone G, Bjorner JB, Brazier JE, Bullinger M, Kaasa S, Leplege A, Prieto L, et al. Cross-validation of item selection and scoring for the SF-12 Health Survey in nine countries: results from the IQOLA Project. International Quality of Life Assessment. J Clin Epidemiol. 1998;51(11):1171–8.
Morfeld M, Kirchberger I, Bullinger M. SF-36 Fragebogen zum Gesundheitszustand: Deutsche Version des Short Form-36 Health Survey; 2011.
Ware J Jr, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–33.
Brazier JE, Harper R, Jones NM, O'Cathain A, Thomas KJ, Usherwood T, Westlake L. Validating the SF-36 health survey questionnaire: new outcome measure for primary care. BMJ. 1992;305(6846):160–4.
Bray JW, Aden B, Eggman AA, Hellerstein L, Wittenberg E, Nosyk B, Stribling JC, Schackman BR. Quality of life as an outcome of opioid use disorder treatment: A systematic review. J Subst Abuse Treat. 2017;76:88–93.
De Maeyer J, Vanderplasschen W, Broekaert E. Quality of life among opiate-dependent individuals: A review of the literature. Int J Drug Policy. 2010;21(5):364–80.
Derogatis LR. Brief Symptom Inventory: BSI; Administration, scoring, and procedures manual. Minneapolis: National Computer Systems; 1993.
Darke S, Hall W, Wodak A, Heather N, Ward J. Development and validation of a multi-dimensional instrument for assessing outcome of treatment among opiate users: the Opiate Treatment Index. Br J Addict. 1992;87(5):733–42.
Darke S, Ward J, Zador D, Swift G. A scale for estimating the health status of opioid users. Br J Addict. 1991;86(10):1317–22.
APA. American Psychiatric Association (APA): Diagnostic and statistical manual of mental disorders (DSM-IV). In: 4th. Washington, DC: American Psychiatric Publishing; 1994.
Guy W: The clinical global impression scale. The ECDEU assessment manual for psychopharmacology revised, vol. DHEW. Rockvillee, MD: US Department of Health, Education, and Welfare. Public Health Service, Alcohol, Drug Abuse, Mental Health Administration, NIMH Psychopharmacology Research Branch, Division of Extramural Research.; 1976.
Christopher J. Ferguson, (2009) An effect size primer: A guide for clinicians and researchers. Professional Psychology: Research and Practice 40 (5):532–538.
Mravcik V, Strada L, Stolfa J, Bencko V, Groshkova T, Reimer J, Schulte B. Factors associated with uptake, adherence, and efficacy of hepatitis C treatment in people who inject drugs: a literature review. Patient Prefer Adherence. 2013;7:1067–75.
Scheiner B, Schwabl P, Steiner S, Bucsics T, Chromy D, Aichelburg MC, Grabmeier-Pfistershammer K, Trauner M, Peck-Radosavljevic M, Reiberger T, et al. Interferon-free regimens improve health-related quality of life and fatigue in HIV/HCV-coinfected patients with advanced liver disease: A retrospective study. Medicine. 2016;95(27):e4061.
Smith-Palmer J, Cerri K, Valentine W. Achieving sustained virologic response in hepatitis C: a systematic review of the clinical, economic and quality of life benefits. BMC Infect Dis. 2015;15:19.
Moreira Tde C, Figueiro LR, Fernandes S, Justo FM, Dias IR, Barros HM, Ferigolo M. Quality of life of users of psychoactive substances, relatives, and non-users assessed using the WHOQOL-BREF. Cien Saude Colet. 2013;18(7):1953–62.
te Vaarwerk MJ, Gaal EA. Psychological distress and quality of life in drug-using and non-drug-using HIV-infected women. Eur J Public Health. 2001;11(1):109–15.
Fingleton N, Matheson C, Jaffray M. Changes in mental health during opiate replacement therapy: A systematic review. Drugs: Education, Prevention and Policy. 2015;22(1):1–18.
Marsden J, Gossop M, Stewart D, Rolfe A, Farrell M. Psychiatric symptoms among clients seeking treatment for drug dependence. Intake data from the National Treatment Outcome Research Study. Br J Psychiatry. 2000;176:285–9.
Lai HM, Cleary M, Sitharthan T, Hunt GE. Prevalence of comorbid substance use, anxiety and mood disorders in epidemiological surveys, 1990-2014: A systematic review and meta-analysis. Drug Alcohol Depend. 2015;154:1–13.
Reissner V, Kokkevi A, Schifano F, Room R, Storbjork J, Stohler R, DiFuria L, Rehm J, Geyer M, Holscher F, et al. Differences in drug consumption, comorbidity and health service use of opioid addicts across six European urban regions (TREAT-project). Eur Psychiatry. 2012;27(6):455–62.
Soyka M, Strehle J, Rehm J, Buhringer G, Wittchen HU. Six-Year Outcome of Opioid Maintenance Treatment in Heroin-Dependent Patients: Results from a Naturalistic Study in a Nationally Representative Sample. Eur Addiction Res. 2017;23(2):97–105.
Ottar N, Marit B, Larry D. Facilitators and barriers in dual recovery: a literature review of first-person perspectives. Adv Dual Diagnosis. 2014;7(3):107–17.
Priester MA, Browne T, Iachini A, Clone S, DeHart D, Seay KD. Treatment Access Barriers and Disparities Among Individuals with Co-Occurring Mental Health and Substance Use Disorders: An Integrative Literature Review. J Subst Abuse Treat. 2016;61:47–59.
Schulte B, Schmidt CS, Kuhnigk O, Schafer I, Fischer B, Wedemeyer H, Reimer J. Structural barriers in the context of opiate substitution treatment in Germany--a survey among physicians in primary care. Subst Abuse Treat Prev Policy. 2013;8:26.
Eiroa-Orosa FJ, Haasen C, Verthein U, Dilg C, Schafer I, Reimer J. Benzodiazepine use among patients in heroin-assisted vs. methadone maintenance treatment: findings of the German randomized controlled trial. Drug Alcohol Depend. 2010;112(3):226–33.
Lader M. Benzodiazepines revisited--will we ever learn? Addiction (Abingdon, England). 2011;106(12):2086–109.
Lugoboni F, Mirijello A, Faccini M, Casari R, Cossari A, Musi G, Bissoli G, Quaglio G, Addolorato G. Quality of life in a cohort of high-dose benzodiazepine dependent patients. Drug Alcohol Depend. 2014;142:105–9.
Caldirola D, Grassi M, Riva A, Dacco S, De Berardis D, Dal Santo B, Perna G. Self-reported quality of life and clinician-rated functioning in mood and anxiety disorders: relationships and neuropsychological correlates. Compr Psychiatry. 2014;55(4):979–88.
Uher R, Perlis RH, Placentino A, Dernovsek MZ, Henigsberg N, Mors O, Maier W, McGuffin P, Farmer A. Self-report and clinician-rated measures of depression severity: can one replace the other? Depress Anxiety. 2012;29(12):1043–9.
Dauber H, Braun B, Pfeiffer-Gerschel T, Kraus L, Pogarell O. Co-occurring Mental Disorders in Substance Abuse Treatment: the Current Health Care Situation in Germany. Int J Mental Health Addict. 2018;16(1):66–80.
Wang J, Kelly BC, Booth BM, Falck RS, Leukefeld C, Carlson RG. Examining factorial structure and measurement invariance of the Brief Symptom Inventory (BSI)-18 among drug users. Addict Behav. 2010;35(1):23–9.
DHS: German Centre for Addiction Issues (DHS, Deutsche Hauptstelle für Suchtfragen): Suchthilfe und Versorgungssituation in Deutschland. Retrieved from: http://www.dhs.de/fileadmin/user_upload/pdf/dhs_stellungnahmen/2014-08-27_DHS-Systemanalyse_Finale_01.pdf 2014. Accessed 12 Dec 2008.
Ellert U, Kurth BM. Health related quality of life in adults in Germany: results of the German Health Interview and Examination Survey for Adults (DEGS1). Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz. 2013;56(5-6):643–9.
DESTATIS: German Federal Statistical Office (DESTATIS, Statistisches Bundesamt). Bevölkerungsstand – Durchschnittsalter nach Geschlecht und Staatsangehörigkeit. 2018. Retreived from: https://www.destatis.de/DE/ZahlenFakten/GesellschaftStaat/Bevoelkerung/Bevoelkerungsstand/Tabellen/Durchschnittsalter_Zensus.html. Accessed 12 Dec 2008.
Ellert U, Bellach BM. Der SF-36 im Bundes-Gesundheitssurvey – Beschreibung einer aktuellen Normstichprobe. Gesundheitswesen. 1999;61(Sonderheft 2):S184–90.
Strada L, Franke GH, Schulte B, Reimer J, Verthein U. Development of OSTQOL: A Measure of Quality of Life for Patients in Opioid Substitution Treatment. Eur Addict Res. 2017;23(5):238–48.
Acknowledgements
We thank Christine Götzke and Dr. Philipp Hiller for their support in the data collection and data management.
Funding
The ‘Epidemiology of Hepatitis C Virus Infection among People Receiving Opioid Substitution Therapy (ECHO)’ study is co-financed by Janssen-Cilag GmbH. Janssen-Cilag GmbH had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Availability of data and materials
The dataset of the current study is not yet publicly available, because analyses on further research questions using this data are still ongoing. However, the parts of the dataset used for this publication are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
BS, UV and JR designed the study; CS and MR performed the data analyses; LS wrote the manuscript; NS contributed to the discussion and commented on the manuscript. All authors reviewed and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was granted by the Ethics Committee of the Medical Association of Hamburg, Ref. PV4603, and by each local Ethics Committee in Germany.
Consent for publication
Not applicable; no details on individuals are reported within the manuscript
Competing interests
JR received unrestricted educational grants, adviser and/or speakers remuneration from AbbVie, Desitin, Gilead, Janssen-Cilag, Mundipharma, Otsuka-Lundbeck, Hexal.
NS received honoraria for several activities (advisory boards, lectures, manuscripts and educational material) by the factories AbbVie, Lundbeck, Medice, Mundipharma, Reckitt-Benckiser/Indivior, and Sanofi-Aventis. During the last three years he participated in clinical trials financed by the pharmaceutical industry.
BS, UV, LS, CS, MR declare no potential conflicts of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Strada, L., Schmidt, C.S., Rosenkranz, M. et al. Factors associated with health-related quality of life in a large national sample of patients receiving opioid substitution treatment in Germany: A cross-sectional study. Subst Abuse Treat Prev Policy 14, 2 (2019). https://doi.org/10.1186/s13011-018-0187-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13011-018-0187-9