
Abstract
Background
The aim of this study was to assess trends in drug resistance and associated clinical and programmatic factors at a national level during the rapid scale up of ART.
Methods
Logistic regression was used to identify the factors associated with HIVDR. Variables associated with drug resistance in multivariable logistic regression were included in the Cochran–Armitage test for trend.
Results
A total of 11,976 patients were enrolled in the study. The prevalence of HIVDR among patients who received ART for 9–24 months during 2003–2008, 2009–2012, and 2013–2015 significantly decreased (15.5%, 6.3%, and 2.3%, respectively, P < 0.01). With respect to the class of antiretroviral, there were substantial increases in resistance to both non-nucleoside reverse transcriptase inhibitors (NNRTIs) and nucleoside reverse transcriptase inhibitors (NRTIs) (2003–2008, 2009–2012, and 2013–2015: 49.7%, 58.9%, and 73.0%, respectively, P < 0.01). The prevalence of DR to protease inhibitors (PIs) was low, which supported their continued use as second-line therapy in China.
Conclusions
Our results provide evidence for the effectiveness of China’s “Treat All” approach to guide policy makers to improve training for healthcare providers and education on ART adherence among patients.
Similar content being viewed by others


Background
The global expansion in the use of antiretroviral therapy (ART) has markedly reduced HIV-related morbidities, mortalities, disease transmission, and adult HIV incidence [1,2]. However, the emergence and spread of high levels of HIV-1 drug resistance (HIVDR) in low- and middle-income countries (LMICs), where a marked increase in the use of combined antiretroviral treatment has occurred, could compromise the effectiveness of national HIV treatment programs [2,3,4]. Recent studies showed that the HIVDR rates were 21% in Namibia, 18.8% in the African regions, and 15.0% in the Southern African regions [5].
With the continued roll-out of ART in LMICs, evidence is emerging of increasing levels of drug resistance prevalence [5, 6]. To extend the benefits of ART to resource-limited settings, which bear most of the HIV burden [7], the World Health Organization (WHO) encourages country ownership through national HIVDR working groups, plans and strategic investment. In some LMICs, national health systems have limited infrastructure, a shortage of healthcare professionals, and weak enforcement of quality standards [8]. These conditions parallel the ones in China 10 years previously. However, throughout the period of increasing implementation of ART, China’s National Free Antiretroviral Treatment Program (NFATP) has been largely successful, with an overall reduction in virological failure and HIV drug resistance since 2008 [9]. Although there is limited access to many antiretrovirals (ARVs) in China, data from the NFATP study prove that understanding the scientific basis and clinical implications of HIVDR is useful in order to shape appropriate surveillance, inform treatment algorithms, and manage difficult cases [9,10,11,12].
Three phases of ART were established according to development stages of NFATP in China: initial and scale-up ART, 2003–2008; standardization and scale-up, 2009–2012; and rapid scale-up, 2013–2015 [13,14,15]. Enormous efforts have been made to develop the capability of treating large numbers of people across wide geographic areas. Important policy changes included increased HIV testing among at-risk populations, as well as an update to the National Free ART Guideline to include patients with higher CD4 cell counts or WHO stage I/II disease and to replace didanosine (ddI) with lamivudine (3TC) in the standard first-line ART regimen in order to significantly decrease HIV-related mortality and HIV transmission. The aim of this study was to evaluate the trends of HIV drug resistance prevalence in treated individuals since the initiation of ART in China. We also examined the effects of the NFATP and the changes in potential clinical and programmatic factors over the past 10 years.
Methods
Study design and study participants
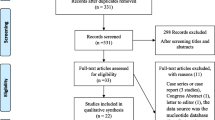
Data collected through the Chinese National HIVDR Surveillance and Monitoring Network since 2003 were analyzed using a retrospective method to assess HIVDR and associated program factors in populations of patients on ART. The database included annual cross-sectional surveys of HIV drug resistance from 2003 to 2015 in China which were described in the previous studies [9, 10, 14, 16,17,18]. and the methodology was endorsed by WHO for HIVDR Monitoring Survey [6,19]. The eligibility criteria were as follows: [1] age ≥ 18 years; [2] receipt of national free initial first-line ART for ≥ 9 months of treatment; [3] visit to a participating clinic for routine NFATP; [4] blood specimens collected for viral load (VL) testing; and [5] consent and willingness to participate in the study. By the end of December 2015, 11,976 cases (ART for at least 9 months) met the inclusion criteria, which represented 2.5% of the 471,140 patients treated by the NFATP. 4679 participants (ART for 9–24 months) were selected in order to compare with other studies and facilitate follow-up treatment.
Laboratory tests
Blood samples of the participants were collected by the local CDC at enrolment and every follow-up visit. Within 8 h, blood samples were sent at ambient temperature to the laboratory of NCAIDS in Beijing, where a team was on-call 24 h for 7 days a week for receipt. Within 2 h after arriving at the laboratory, CD4 cell count was conducted using flow cytometry (FACS Calibur, BD Company, Franklin Lakes, New Jersey, USA). Plasma was isolated and frozen at − 80 °C until testing for viral load and HIVDR. According to the manufacturers’ recommendations, plasma HIV RNA in this study was quantified with real-time NASBA (NucliSense Easy Q, bioMe′rieux, Lyon, France) or with Amplicor HIV-1 monitor test (COBAS, Roche Applied Science, Penzberg, Germany). A VL ≥ 1000 was classified as virologic failure based on WHO HIVDR surveillance guideline. In samples with virologic failure on ART, HIVDR genotyping was performed at the WHO Accreditation Laboratory of NCAIDS, China CDC by using an in-house method as previously described [9, 17, 20, 21]. Drug resistance mutation analysis and viral subtype determination were performed on a 1.3 kb section of the HIV pol gene using the Stanford University HIVDR Database online sequence analysis tool (http://hivdb.stanford.edu/, accessed 2 November 2018). All HIVDR mutations that conferred low (total score 15 to 29), intermediate (total score 30 to 59) or high-level (total score ≥ 60) resistance were included [9, 22]. The frequency of resistance to specific ARV drugs and resistance to both NRTI and NNRTI drugs was calculated by SAS program according to the results of the Stanford online sequence analysis tool. Study participants were informed of the laboratory tests results and the results were used to select subsequent ART regimen.
Statistical analysis
Logistic regression was used to identify the factors associated with HIVDR. The factors associated with HIVDR that were significant in the univariate logistic regression analysis were included in the multivariate logistic regression. Variables associated with resistance in the multivariable logistic regression model and those clinically meaningful were included in the Cochran–Armitage test for trend. Somers’ D (R|C) was used to measure the association between the variables (considered as the response) and the time of initial ART (year; considered as a predictor). Statistical significance was defined as a P value < 0.05. All the statistical analyses were performed with SAS 9.4 software (SAS Institute, Cary, NC, USA).
Results
Factors associated with drug resistance among patients who received first-line ART
Among the 4679 patients who received first-line ART for 9–24 months, 8.6% (402) patients had HIVDR. The prevalence of HIVDR during 2003–2008 (n = 1882), 2009–2012 (n = 1163), and 2013–2015 (n = 1634) significantly decreased (15.5%, 6.3%, and 2.3%, respectively, Cochran-Armitage test, P < 0.01). The factors significantly associated with HIVDR in the multivariate logistic regression model were education, occupation, route of HIV infection, WHO clinical stage III/IV, CD4 cell count before ART, and time of beginning ART. Compared with patients with post-secondary school or higher education, those with secondary school or lower education were more likely to show DR (adjusted odds ratio [AOR]: 1.5, 95% confidence interval [CI] 1.0–2.1). Compared with people from other occupations, farmers were more likely to show DR (AOR: 1.8, 95% CI 1.3–2.5). With regard to route of HIV infection, compared with heterosexual intercourse, homosexual intercourse was likely to show less DR (AOR: 0.8, 95% CI 0.4–1.5); blood or plasma transfusion was more likely to show DR (AOR: 2.9, 95% CI 2.0–4.4); intravenous drug use was more likely to show DR (AOR: 2.1, 95% CI 1.4–3.1); and other or unknown routes were more likely to show DR (AOR: 1.8, 95% CI 1.1–3.1). Furthermore, compared with patients with other WHO clinical stages, those with WHO clinical stage III/IV were more likely to show DR (AOR: 1.6, 95% CI 1.1–2.1). Patients with CD4 count ≥ 349 cells/mm3 showed less DR than patients with CD4 count < 349 cells/mm3 (AOR: 0.6, 95% CI 0.3–0.9), and patients who began ART from or after 2009 showed less DR than patients who began ART before 2009 (AOR: 0.5, 95% CI 0.4–0.7). With regard to the location of ART drug distribution, county hospital or CDC showed lower DR than township hospital or village clinic (AOR: 0.4, 95% CI 0.3–0.5). Patients who missed any dose in the past month were more likely to show DR than those who did not miss any dose (AOR: 1.7, 95% CI 1.1–2.5). Compared with lamivudine-based regimens, other regimens were more likely to show DR (AOR: 1.6, 95% CI 1.2–2.1) (Table 1).
Changes in factors associated with drug resistance in patients who commenced first-line ART during 2003–2008, 2009–2012, and 2013–2015
Variables associated with HIVDR in the multivariable regression model were included in the Cochran–Armitage test for trend over time. These variables included education, occupation, marital status, route of HIV infection, CD4 cell count before ART, initial ART regimen, missed doses in the past month, location of ART drug distribution, and adverse drug reactions. The proportions of these variables were compared among patients who received ART during 2003–2008, 2009–2012, and 2013–2015. A trend test showed statistically significant changes in factors associated with drug resistance over time for: education level of high school and above, farming occupation, heterosexual or homosexual intercourse, WHO clinical stage III/IV before ART, CD4 cell count ≥ 350 before ART, lamivudine-based regimens, drug receipt from a county hospital or CDC, and adverse drug reactions. However, there was no significant change related to missed doses in the past months (Table 2).
HIVDR mutations
There were substantial increases in resistance to both NNRTI and NRTIs (2003–2008, 2009–2012, and 2013–2015: 49.7%, 58.9%, and 73.0%, respectively, P < 0.01). The most-common NNRTI mutations occurred at positions 101 (9.5%), 103 (49.5%), 181 (12.9%), and 190 (9.5%) in the RT region; the most-common NRTI mutations occurred at codons 41 (10.2%), 67 (13.4%), and 184 (32.3%) in the RT region; and protease inhibitors (PI) mutations were most frequently seen at codons 32 (0.7%), 46(1.5%) and 54 (0.7%) in the protease (PR) region (Table 3).
Discussion
This retrospective analysis of the Chinese National HIVDR Surveillance Database from 2003 to 2015 showed the overall prevalence of HIVDR has declined significantly since the commencement of programs for ART use in China (2018). The recent (2009–2012, 2013–2015) prevalence of HIVDR among patients who received first-line ART for 9–24 months was found to be 6.3 and 2.3%, respectively. The prevalence of HIVDR found in our study was significantly lower than that in some developed countries or countries where free ART was available nationwide [3, 23]. The drug resistance prevalence was found to be relatively low in China, as compared with the prevalence in other LMICs, even after the rapid scale up of ART [3, 24].
The overall low prevalence of DR may reflect the relatively low coverage and short duration of free ART or, equally, may reflect the success of first-line ART regimens and HIV prevention programs. Our study assessed the clinical and programmatic factors associated with HIVDR in patients who received first-line ART during 2003–2015. Virologic failure among Chinese patients who received ART for 9–24 months during 2003–2008, 2009–2012, and 2013–2015 significantly improved (25.7%, 17.3%, and 7.0%, respectively, P < 0.01).The significant improvements in virologic outcome in Chinese patients receiving ART treatment over the past 10 years may be attributable to changes in a number of clinical and programmatic factors. Firstly, the Chinese NFATP policy has changed since 2003, due to the availability of an expanded range of antiviral drug resources. For instance, AZT, d4T, ddI, and NVP were generically produced in China and used as standard prescriptions from the beginning of the NFATP, whereas 3TC and EFV were branded drugs that became available in 2005 and were gradually more commonly prescribed. First-line ART regimens were revised to consist of tenofovir (TDF)/AZT + EFV/NVP in 2008 [9]. Our previous study showed that the decline in virologic failure and HIVDR were strongly associated with the standardized use of 3TC-based regimens instead of ddI-based regimens; this study confirmed the previous finding, showing since 2008, virological failure at 12–15 months of treatment had improved from 26.6 to 12.1%, and HIVDR rates were also significantly decreased from 15.4 to 5.4% [9]. Our studies also showed that patients who initiated 3TC-based regimens showed improvements in adherence compared with those who initiated ddI-based regimens. 3TC-based regimens have more curative effect than ddI-based regimens, and it is advantageous in improving the patient’s quality of life and the compliance of medicine. Replacing ddI-based regimens may explain some of the difference seen in terms of the tolerability in the treatment population, and this improvement could greatly improve adherence and subsequently less HIVDR. Secondly, adverse effects were reduced from 2003 to 2015 due to a revision of the first-line ART regimen in China, since 2003 patients had started ART when the CD4 cell count was < 200 cells/mm3; this threshold then increased to 350 cells/mm3 in 2012 and further increased to 500 cells/mm3 in 2014. A further important policy change in NFATP included the location of ART drug distribution; increased rates of distribution at county hospitals or CDC have occurred over time, which has improved the quality of care and treatment. The stratified analysis showed that patients receiving ART at county hospitals had lower HIVDR rates than those treated at village- or town-level clinics.
Changes in social and demographic factors among patients since the initiation of NFATP in 2003 had also been associated with treatment outcome over time. The proportion of HIV patients with a higher education level (high school and above) increased from 14.5% in 2003–2008 to 43.7% in 2013–2015. In addition, more HIV patients were from non-agricultural occupations (increased from 30.1 to 53.8%) and the number that had contracted HIV due to heterosexual or homosexual intercourse, compared to other routes such as drug use, increased from 31.6 to 53.0% (Table 2). Our previous studies showed that a low education level, the occupation of farming, drug use, and being a blood recipient were associated with a high prevalence of HIVDR [9, 18.] Although a significant change in these factors may have substantially contributed to the overall reduction in HIVDR in China, patient adherence (non-missed doses in the past month) did not significantly improve over time. Due to the rapidly increasing number of patients treated through the NFATP, more drug resistance could emerge in the future, especially if treatment adherence is not sustained. Therefore, it is crucial for the NFATP to focus on improving the quality of care and ART education in its next phases of implementation.
Rapid expansion of ART raises concerns for long-term sustainability and emerging dual-class resistance (NNRT and NRTIs) in China. Among the 402 treatment-experienced patients with DR mutations, 215 (53.5%) harbored dual-class resistance. With respect to the class of ART drugs, there were substantial increases in resistance to both NNRT and NRTIs over time (from 49.7 to 73.0%). In particular, expanded ART without improved adherence is likely to result in dual-class resistance, which may lead to poor treatment outcomes and HIVDR. The most common NNRTI mutations were K103 and Y181, and the most common NRTI mutations were M184, D67 and M41. In addition, the prevalence of DR to PIs was low, which supported their continued use as second-line therapy in China.
Apart from important findings, our study has several limitations. First, unlike a cohort study, in which a group of patients is assessed continuously over time, a cross-sectional survey, by its very nature, excludes patients who are no longer receiving ART and therefore cannot be observed because they have died, been lost to follow-up, or have stopped treatment. This survivor bias can significantly impact the interpretation of outcomes. In order to adjust for such a possible bias, we collected nationally representative data on retention at 12 months. By the end of 2015, 10.2% of the patients had died, whilst 8.7% were found to have terminated treatment among those treated by the NFATP in China. Accordingly, the adjusted prevalence of virologic failure and DR among patients who received first-line ART for 9–24 months during 2013–2015 was 7.0–8.3 and 2.3–2.7%, respectively. Second, a large proportion of patients began initial ddI treatment during the earlier years of the NFATP, when the baseline CD4 cell count was not required to be of a certain threshold and the standards of care and follow-up were low, which might have contributed to the poor treatment outcomes in the first few years of the NFATP.
Conclusions
However, these limitations do not have a considerable bearing on our conclusion on the changes in HIVDR from 2003 to 2015 in China. To our knowledge, this is the first large observational study worldwide to assess the outcomes of ART over the past 10 years. The results provide evidence for the effectiveness of China’s HIV control and prevention efforts such as the “Treat All” approach. Furthermore, the findings will help guide policy makers to improve training for healthcare providers and enhance patient education on ART adherence. Further monitoring of virologic outcomes is needed to elucidate the determinants of long-term programmatic success. Government advocacy, specialist physician management, laboratory monitoring and constantly raising the level of education, all played a role in the success of NFATP. This study had the advantage of having thoroughly examined these factors and their relationship in one analysis, and the results were particularly important for countries with limited resources.
Availability of data and materials
The datasets used or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ART:
-
Antiretroviral therapy
- HIV:
-
Human immunodeficiency virus
- HIVDR:
-
HIV drug resistance
- NNRTIs:
-
Non-nucleoside reverse transcriptase inhibitors
- NRTIs:
-
Nucleoside reverse transcriptase inhibitors
- PIs:
-
Protease inhibitors
- LMICs:
-
Low- and middle-income countries
- WHO:
-
World Health Organization
- NFATP:
-
National Free Antiretroviral Treatment Program
- ARVs:
-
Antiretrovirals
- ddI:
-
Didanosine
- 3TC:
-
Lamivudine
- D4T:
-
Stavudine
- AZT:
-
Zidovudine
- TDF:
-
Tenofovir
- CDC:
-
Centers for disease control
References
Bor J, Herbst AJ, Newell ML, Barnighausen T. Increases in adult life expectancy in rural South Africa: valuing the scale-up of HIV treatment. Science. 2013;339(6122):961–5.
Gregson J, Kaleebu P, Marconi VC, van Vuuren C, Ndembi N, Hamers RL, et al. Occult HIV-1 drug resistance to thymidine analogues following failure of first-line tenofovir combined with a cytosine analogue and nevirapine or efavirenz in sub Saharan Africa: a retrospective multi-centre cohort study. Lancet Infect Dis. 2017;17(3):296–304.
Godfrey C, Thigpen MC, Crawford KW, Jean-Phillippe P, Pillay D, Persaud D, et al. Global HIV antiretroviral drug resistance: a perspective and report of a national institute of allergy and infectious diseases consultation. J Infect Dis. 2017;216:S798.
Hunt GM, Kainne Dokubo E, Takuva S, de Oliveira T, Ledwaba J, Dube N, et al. Rates of virological suppression and drug resistance in adult HIV-1-positive patients attending primary healthcare facilities in KwaZulu-Natal, South Africa. J Antimicrob Chemother. 2017;72:3141.
Hong SY, Jonas A, DeKlerk M, Shiningavamwe A, Desta T, Badi A, et al. Population-based surveillance of HIV drug resistance emerging on treatment and associated factors at sentinel antiretroviral therapy sites in Namibia. J Acquir Immune Defic Syndr. 2015;68(4):463–71.
Jordan MR, Bennett DE, Bertagnolio S, Gilks CF, Sutherland D. World Health Organization surveys to monitor HIV drug resistance prevention and associated factors in sentinel antiretroviral treatment sites. Antivir Ther. 2008;13(Suppl 2):15–23.
Bekker LG, Gray GE. Hope for HIV control in southern Africa: the continued quest for a vaccine. PLoS Med. 2017;14(2):e1002241.
Global AIDS Update 2016. Geneva: UNAIDS; 2016. http://www.unaids.org/sites/default/files/media_asset/global-AIDS-update-2016_en.pdf. Last accessed 20 September 2016.
Xing H, Ruan Y, Hsi JH, Kan W, Liao L, Leng X, et al. Reductions in virological failure and drug resistance in Chinese antiretroviral-treated patients due to lamivudine-based regimens, 2003-12. J Antimicrob Chemother. 2015;70(7):2097–103.
Liu P, Feng Y, Wu J, Tian S, Su B, Wang Z, et al. Polymorphisms and mutational covariation associated with death in a prospective cohort of HIV/AIDS patients receiving long-term ART in China. PLoS ONE. 2017;12(1):e0170139.
Luo XL, Mo LD, Su GS, Huang JP, Wu JY, Su HZ, et al. Incidence and types of HIV-1 drug resistance mutation among patients failing first-line antiretroviral therapy. J Pharmacol Sci. 2019;139:275.
Hu X, Liang B, Zhou C, Jiang J, Huang J, Ning C, et al. HIV late presentation and advanced HIV disease among patients with newly diagnosed HIV/AIDS in Southwestern China: a large-scale cross-sectional study. AIDS Res Ther. 2019;16(1):6.
Zhao DC, Wen Y, Ma Y, Zhao Y, Zhang Y, Wu YS, et al. Expansion of China’s free antiretroviral treatment program. Chin Med J (Engl). 2012;125(19):3514–21.
Liu P, Liao L, Xu W, Yan J, Zuo Z, Leng X, et al. Adherence, virological outcome, and drug resistance in Chinese HIV patients receiving first-line antiretroviral therapy from 2011 to 2015. Medicine (Baltimore). 2018;97(50):e13555.
Liu P, Tang Z, Lan G, Zhu Q, Chen H, You Y, et al. Early antiretroviral therapy on reducing HIV transmission in China: strengths, weaknesses and next focus of the program. Sci Rep. 2018;8(1):3431.
Liao L, Xing H, Su B, Wang Z, Ruan Y, Wang X, et al. Impact of HIV drug resistance on virologic and immunologic failure and mortality in a cohort of patients on antiretroviral therapy in China. AIDS. 2013;27(11):1815–24.
Xing H, Wang X, Liao L, Ma Y, Su B, Fu J, et al. Incidence and associated factors of HIV drug resistance in Chinese HIV-infected patients receiving antiretroviral treatment. PLoS ONE. 2013;8(4):e62408.
Zuo Z, Liang S, Sun X, Bussell S, Yan J, Kan W, et al. Drug resistance and virological failure among HIV-infected patients after a decade of antiretroviral treatment expansion in eight provinces of China. PLoS ONE. 2016;11(12):e0166661.
WHO. World Health Organization global strategy for the surveillance and monitoring of hiv drug resistance 2012. http://www.who.int/hiv/pub/ drugresistance/drug_resistance_strategy/en/.
Wang X, Yang L, Li H, Zuo L, Liang S, Liu W, et al. Factors associated with HIV virologic failure among patients on HAART for one year at three sentinel surveillance sites in China. Curr HIV Res. 2011;9(2):103–11.
Liao L, Xing H, Shang H, Li J, Zhong P, Kang L, et al. The prevalence of transmitted antiretroviral drug resistance in treatment-naive HIV-infected individuals in China. J Acquir Immune Defic Syndr. 2010;53(Suppl 1):S10–4.
Liu TF, Shafer RW. Web resources for HIV type 1 genotypic-resistance test interpretation. Clin Infect Dis. 2006;42(11):1608–18.
Liao L, Xing H, Dong Y, Qin G, Ma Y, Lu H, et al. Surveys of transmitted HIV drug resistance in 7 geographic Regions in China, 2008–2009. Clin Infect Dis. 2012;54(Suppl 4):S320–3.
Gupta RK, Jordan MR, Sultan BJ, Hill A, Davis DH, Gregson J, et al. Global trends in antiretroviral resistance in treatment-naive individuals with HIV after rollout of antiretroviral treatment in resource-limited settings: a global collaborative study and meta-regression analysis. Lancet. 2012;380(9849):1250–8.
Acknowledgements
We are grateful to all members of the national HIVDR working group, and to the study participants and their communities, for their contributions to the research. We thank the patients and doctors throughout China for their consent and support for the study.
Funding
This study was supported by grants from the National Natural Science Foundation of China (11971479, 81471962, 11471336), the Ministry of Science and Technology of China (2008ZX10001-004, 2012ZX10001-002, 2017ZX10201101-002-004, 2018ZX10721102-006), the Chinese State Key Laboratory for Infectious Disease Develop Grant, Shandong medical and health science technology development program (2017WS410), and the Guangxi Honor Scholar.
Author information
Authors and Affiliations
Contributions
Conceptualization: PL HX YR YS. Data curation: YR HX LL YF PL XL JW WK JY YL ZZ YY. Formal analysis: PL YR. Funding acquisition: HX YR YS. Investigation: YR HX LL YF PL XL WK JY YL ZZ. Methodology: PL YR YS. Project administration: PL HX YR YS. Software: PL YR YF. Supervision: YL YY LL YF YR. Validation: YY YL YF. Writing ± original draft: PL YR YY. Writing ± review & editing: PL YR YY YS YR. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
All subjects provided written informed consent to participate in this study. The institutional review board of the National Center for AIDS/STD Control and Prevention (NCAIDS), Chinese Center for Disease Control and Prevention (China CDC) approved this study (ethical Approval Number: X140617334).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Liu, P., Xing, H., Liao, L. et al. HIV drug resistance in patients in China’s national HIV treatment programme who have been on first-line ART for at least 9 months. AIDS Res Ther 17, 9 (2020). https://doi.org/10.1186/s12981-020-00264-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12981-020-00264-5