
Abstract
Background
Alzheimer’s Disease (AD) is a chronic neurodegenerative disorder characterized by extracellular plaques, intracellular neurofibrillary tangles and neuronal loss in the central nervous system (CNS). Pathogens are suspected to have a role in the development of AD; herpes simplex virus type 1 (HSV-1), in particular, is suggested to be a risk factor for the disease. The gamma receptor for the Fc portion of IgG molecules (FCGRs) plays a crucial role in regulating immune responses, and among FCGRs, FCGRIIB is endowed with an inhibitory function. Notably, the rs1050501 polymorphism of FCGRIIB gene associates with autoimmune diseases and with neuronal uptake and interneuronal accumulation of amyloid beta in animal AD models.
Methods
Genotype and allelic distribution of ApoE4 and FCGRIIB rs1050501 were evaluated in a case–control population of 225 AD patients, 93 MCI individuals and 201 sex and age matched healthy controls (HC). HSV-1 total IgG titers and IgG subclasses were detected and quantified in a subgroup of the main study population by ELISA.
Results
Genotype and allelic distribution of FCGRIIB was comparable in the study population. HSV-1-specific antibody titers were significantly higher in AD and MCI compared to HC (p < 0.01 for both); IgG3 titers, in particular, were increased in MCI compared to AD (p = 0.04). Analyses of possible correlations between the FCGRIIB rs1050501 genotype polymorphism and IgG subclasses showed that the presence of IgG3 was more frequent in MCI carrying the FCGRIIB TT (94.1%) compared to those carrying the CT genotype (63.6%) (p = 0.03).
Conclusion
Results herein show an association between humoral immune response against HSV-1 and FCGRIIB rs1050501 genetic variation in the first stage of the disease.
Similar content being viewed by others


Background
Alzheimer’s Disease (AD) is an inflammatory chronic neurodegenerative disease characterized by a progressive deterioration in global intellectual ability that interferes with social and occupational performance [1]. Mild cognitive impairment (MCI), on the other hand, is an intermediate condition between physiological neurocognitive aging and AD [1, 2]. Over time, MCI can convert to AD with an estimated conversion rate of 10-to-15% [3]. The etiopathogenesis of AD likely includes both genetic and environmental factors. Among genetic factors Apolipoprotein E (APOE) is the only confirmed risk factor for the disease, but other genes [4], including those of the SNARE complex [5, 6], PILRA [7] and TREM2 [8] are strongly suggested to play a role in AD. Pathogens are also suspected to be involved in AD [9]; herpes simplex virus type 1 (HSV-1), in particular, is a likely culprit [10,11,12].
HSV-1-specific immune response is classically mediated by antibodies (Abs), thus, the gamma receptor for the Fc portion of IgG Abs (FCGRs) forms immune complexes and activates the effector arm of the immune system [13]. Six different FCGRs are known in humans: FCGRI, FCGRIIA, FCGRIIB, FCGRIIC, FCGRIIIA, and FCGRIIIB [14]. FCGRIIB is the only FCGR endowed with inhibitory functions [15], and FCGRIIB impairments are associated with inflammatory conditions [14]. The human FCGRIIB gene, located on 1q23.3, includes a number of single nucleotide polymorphisms (SNPs); amongst the nonsynonymous SNPs, the T-to-C transition in exon 5 (rs1050501), which leads to a replacement of isoleucine at position 232 by threonine (FCGRIIB-I232T variant), is relatively frequent and correlates with autoimmune disease [16,17,18,19]. HSV-1 evasion from the immune response can be mediated by the expression of a viral receptor, homologous to human FCGR, which binds all human IgG subclasses, with the exception of IgG3 [20]. Susceptibility to HSV-1 infection was shown to associate with FCGRIIIA polymorphisms [21], but the possible role of FCGRIIB variants in HSV-1 infection has not been explored. Importantly, results obtained in the animal model of AD showed that the rs1050501 polymorphism of FCGRIIB results in neuronal uptake and interneuronal accumulation of amyloid beta [22].
We evaluated possible correlations between the HSV-1-specific humoral immune response and FCGRIIB rs1050501 SNP in a cohort of Italian AD, MCI, and sex- and age-matched Healthy Control (HC) subjects.
Methods
Patients and controls
Five-hundred-nineteen individuals were included in the study: 225 Alzheimer’s Disease (AD) patients, 93 Mild Cognitive Impairment (MCI) individuals, and 201 sex and age matched Healthy Controls (HC). All subjects were recruited by the Rehabilitative Neurology Unit of the IRCCS Santa Maria Nascente, Don Gnocchi Foundation, in Milan, Italy. Patients were diagnosed as probable AD according to the NINCDS-ADRDA criteria [1], or as MCI according to Petersen and Grundman criteria [23, 24]. Patients were excluded if they suffered from malnutrition or vitamin deficiency syndromes, and recent introduction or dose modification of the following pharmacological treatments: cholinesterase inhibitor, nemantine, antidepressant or antipsychotic drugs.
The study conformed to the ethical principles of the Declaration of Helsinki; all subjects or their care-givers gave informed and written consent according to a protocol approved by the local ethics committee of the Don Carlo Gnocchi Foundation–ONLUS, Milan, Italy (#12_21/6/2018).
SNPs typing
Whole blood was collected for all the subjects of the main study population and genomic DNA was isolated by phenol–chloroform extraction. Customer-design TaqMan® probes for the 112 and 158 codons were used to determine the genotype of APOE [25].
FCGRIIB SNP rs1050501 (C > T) [26], was determined by a custom-designed TaqMan® genotyping assay from Applied Biosystems Inc. (by Life Technologies, Foster City, CA, USA), using a two-step approach. First, using the following primers, a 494-base pair fragment was amplified:
Forward primer: 5′-CTAAGAGGAGCCCTTCCCTATGT-3′
Reverse primer: 5′-AATACGGGCCTAGATCTGAATGTG-3′
This was followed by a TaqMan RT-PCR using two probes specific for each allele (C and T). The primer and probe sequences for this reaction are listed below:
Forward primer: 5′-CCTAGCTCCCAGCTCTTCAC-3′
Reverse primer: 5′-CCACTACAGCAGCAACAATGG-3′
Reporter 1 (C-specific): HEX-TCACTGGGACTGCTGTAGCG-NFQ
Reporter 2 (T-specific): FAM-TCACTGGGATTGCTGTAGCG-NFQ
Anti-HSV-1 IgG antibody measurements
For a subgroup of 170 subjects (69 AD, 52 MCI and 49 HC) serum samples were available for the detection of HSV-1 IgG titers, using a commercial enzyme-linked immunosorbent assay (ELISA) (IBL International, Hamburg, Germany). The optical densities (OD) were determined at 450 nm, using 620 nm reading as reference wavelength, as reported by datasheet. HSV-1 Ab titers were expressed as antibody index (AI), calculated by dividing OD measurement generated from the assay by OD cut-off calibrator. Quantitation of the four different HSV-1 IgG subclasses was carried out by a modified ELISA assay (IBL International), using four biotinylated subtype-specific monoclonal antibodies (Sigma-Aldrich, St. Louis, Mo, US), as previously described [27].
Statistical analysis
Chi‐square goodness of fit test was used to verify that genotypes were in Hardy–Weinberg (HW) equilibrium and contingency. Chi square was used to evaluate differences between groups. FCGRIIB allelic polymorphism distribution in AD, MCI and HC was analyzed by odds ratio (OR) and 95% confidence interval (95% CI). p‐value was considered significant when < 0.05 after Bonferroni correction for two degrees of freedom (Pc) in 2 × 3 and 2 × 2 contingency tables.
The parametric data were expressed as mean ± standard deviation, whereas the non-parametric data as median and interquartile range (IQR). AD, MCI and HC were compared on demographic data using Chi square test and One-way ANOVA with Bonferroni post hoc test for categorical and continuous variables, respectively. Differences in experimental data among groups were tested using Kruskal–Wallis test and, when appropriate, the Mann–Whitney U test, and the correlations using Spearman’s correlation coefficient. The p-values corresponding to < 0.05 were described as statistically significant in the text. The statistical analyses were accomplished using commercial software (MedCalc Statistical Software version 14.10.2, Ostend, Belgium). A priori power analysis was run with the G-power software [28].
Results
Clinical characteristics
Demographic and clinical characteristics of the study population are summarized in Table 1. Gender and age were similar in all groups examined. As expected, the MMSE score was lower in AD (18.66 ± 5.53) compared to MCI (24.85 ± 2.89) (p < 0.01).
APOE and FCGRIIB genotype distribution
As expected, ApoE4 variant was more frequently seen in AD (52.0%) and MCI (39.5%) patients compared to HC (17.7%) (p < 0.0001 for both), and in AD compared to MCI (p = 0.046). The genotype distribution of the FCGRIIB polymorphism was in HW equilibrium in the three groups of individuals enrolled in the study. Genotype and allelic distribution of FCGRIIB was comparable in the study population (Table 1). Moreover, we analyzed the FCGRIIB genotype distribution after categorization for APOE4 (pos/neg) and sex (male/female) in the study population, but no differences were found (data not shown).
Virological data
HSV-1 seropositivity was 97%, without difference among the three examined subgroups (95.6% for AD, 98.1% for MCI and 97.9% for HC). Results confirmed [29] that HSV-1 titers were significantly higher in AD (p = 0.001) and MCI patients (p = 0.008) compared to HC; HSV-1 avidity index was reduced, although not significantly, in AD compared to the other two groups of individuals (Table 1). The percentage of individuals showing serum HSV-1-specific IgG1, IgG2 and IgG4 was comparable in AD, MCI and HC individuals, whereas IgG3 were more frequently observed in MCI (87.2%) compared to AD (75.0%, p = 0.04) and HC (74.3%) (Fig. 1).

Frequency of HSV-1-specific IgG3 in 69 AD, 52 MCI and 49 HC subjects. The Chi square test was used to analyze the statistical differences among groups(AD vs. MCI: p = 0.04)
FCGRIIB polymorphism
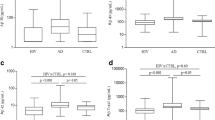
No associations were detected between serum HSV-1 antibody and FCGRIIB genotypes when the entire study population or the three groups alone were analyzed (Table 2). No correlations were detected either between FCGRIIB genotypes and HSV-1-specific IgG1, IgG2 and IgG4 in the study population. In MCI though, the FCGRIIB TT genotype correlated with a significantly increased likelihood to observe HSV-1-specific serum IgG3 antibodies (94.1%), whereas MCI carrying CT genotype were less likely to present IgG3 antibodies (63.6%) (p = 0.03) (Fig. 2).

Frequency of HSV-1-specific IgG3 in 69 AD, 52 MCI and 49 HC subjects according to FCGRIIB rs1050501 genotypes distribution. The Chi square test was used to analyze the statistical differences among groups (MCI CT vs. MCI TT: p = 0.03)
Discussion
We focused our attention on FCGRIIB, a receptor of the FCGR family that plays an important role in the immune cell activation, balancing immunoprotection and immunopathology [30]. FCGRs are glycoproteins that bind the Fc component of IgG. FCGRIIB length is 310 aminoacids, and because of its tertiary structure–with one intracellular, one extracellular and one transmembrane domain–the protein localizes in the plasma membrane [31, 32]. FCGRIIB is widely expressed on immune cells, including monocytes, neutrophils, macrophages, basophils, eosinophils and B-cells [33,34,35] and plays an inhibitory role, preventing an inappropriate activation of immune cells in the absence of antigens [15]. Interestingly, FCGRIIB is associated with the accumulation of amyloid beta in 3xTg-AD mice, suggesting its possible involvement in AD [22]. FCGRIIB is characterized by several polymorphisms and recent results indicated that the SNP rs1050501 (I232T), located in exon 5, is associated with autoimmune diseases [36]. Although no differences were observed in FCGRIIB genotype distribution in our study population, we found an association between rs1050501 and IgG3 distribution in MCI, i.e. MCI individuals carrying the FCGRIIB TT genotype were much more likely to express HSV-1-specific IgG3 antibodies compared those carrying the CT genotype.
HSV-1 evades the host immune response by binding all IgG subclasses, except for IgG3, with a viral Fc receptor. The more common detection of HSV-1-specific IgG3 in MCI suggests that these individuals try to suppress HSV-1 reactivation by increasing the expression of the IgG3 subclass, the only one which mounts an effective antiviral immune response. Results herein allow to speculate that in MCI the ability to block the viral reactivation is due not only to IgG3 production but probably depends on the FCGRIIB rs1050501 genotype.
Further analyses with a larger cohort, as well as a longer clinical follow-up to verify if and when MCI and in particular, MCI carrying FCGRIIB TT genotype, will develop AD, and if the correlation with IgG3 in these converted patients remains significant, will be necessary to further confirm these data.
Moreover, future studies are needed to shed light on the mechanism linking FCGR polymorphisms, in particular FCGRIIB rs1050501, and IgG3. Thus, it will be important to verify whether FCGR polymorphisms leading to aminoacidic variants (i.e. FCGRIIB rs1050501 to I232T variant) could affect the protein structural conformation, possibly influencing signalling pathways and Ab affinity for antigens.
Conclusion
Findings of the present work offer further support for HSV-1 being a factor in the pathogenesis of AD: all together these results suggest, for the first time, the presence of an association between HSV-1 humoral immune responses and FCGRIIB rs1050501 SNP in the setting of MCI and AD.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available due to privacy or ethical restrictions but are available from the corresponding author on reasonable request.
Abbreviations
- AD:
-
Alzheimer’s disease
- MCI:
-
Mild cognitive impairment
- HC:
-
Healthy control
- CNS:
-
Central nervous system
- HSV-1:
-
Herpes simplex virus type 1
- APOE:
-
Apolipoprotein E
- Ab:
-
Antibodies
- FCGRs:
-
Gamma receptor for the Fc portion of IgG Abs
- SNPs:
-
Single nucleotide polymorphisms
- OD:
-
Optical densities
- AI:
-
Antibody index
- HW:
-
Hardy–Weinberg
- OR:
-
Odds ratio
- IQR:
-
Interquartile range
References
McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR Jr, Kawas CH, Klunk WE, Koroshetz WJ, Manly JJ, Mayeux R, Mohs RC, Moris JC, Rossor MN, Scheltens P, Carrillo MC, Thies B, Weintraub S, Phelps CH. The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7:263–9.
Albert MS, DeKosky ST, Dickson D, Dubois B, Feld man HH, Fox NC, Gamst A, Holtzman DM, Jagust WJ, Petersen RC, Snyder PJ, Carrillo MC, Thiers B, Phelps CH. The diagnosis of mild cognitive impairment due to Alzhimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Demen. 2011;7:270–9.
Petersen RC. Clinical practice. Mild Cognitive 487 impairment. N Engl J Med. 2011;364:2227–34.
Nikolac Perkovic M, Pivac N. Genetic markers of Alzheimer’s disease. Adv Exp Med Biol. 2019;1192:27–52.
Guerini FR, Agliardi C, Sironi M, Arosio B, Calabrese E, Zanzottera M, Bolognesi E, Ricci C, Costa AS, Galimberti D, Griffanti L, Bianchi A, Savazzi F, Mari D, Scarpini E, Baglio F, Nemni R, Clerici M. Possible association between SNAP-25 single nucleotide polymorphisms and alterations of categorical fluency and functional MRI parameters in Alzheimer’s disease. J Alzheimers Dis. 2014;42:1015–28.
Costa AS, Guerini FR, Arosio B, Galimberti D, Zanzottera M, Bianchi A, Nemni R, Clerici M. SNARE complex polymorphisms associate with alterations of visual selective attention in Alzheimer’s Disease. J Alzheimers Dis. 2019;69:179–88.
Agostini S, Costa AS, Mancuso R, Guerini FR, Nemni R, Clerici M. The PILRA G78R variant correlates with higher HSV-1-specific IgG titers in Alzheimer’s Disease. Cell Mol Neurobiol. 2019;39:1217–21.
Guerreiro R, Wojtas A, Bras J, Carrasquillo M, Rogaeva E, Majounie E, Cruchaga C, Sassi C, Kauwe JS, Younkin S, Hazrati L, Collinge J, Pocock J, Lashley T, Williams J, Lambert JC, Amouyel P, Goate A, Rademakers R, Morgan K, Powell J, St George-Hyslop P, Singleton A, Hardy J, Alzheimer Genetic Analysis Group. TREM2 variants in Alzheimer’s disease. N Engl J Med. 2013;368:117–27.
Itzhaki RF, Lathe R, Balin BJ, Ball MJ, Bearer EL, Braak H, Bullido MJ, Carter C, Clerici M, Cosby SL, Del Tredici K, Field H, Fulop T, Grassi C, Griffin WS, Haas J, Hudson AP, Kamer AR, Kell DB, Licastro F, Letenneur L, Lövheim H, Mancuso R, Miklossy J, Otth C, Palamara AT, Perry G, Preston C, Pretorius E, Strandberg T, Tabet N, Taylor-Robinson SD, Whittum-Hudson JA. Microbes and Alzheimer’s Disease. J Alzheimers Dis. 2016;51:979–84.
Ball MJ. Limbic predilection of Alzheimer’s dementia: is reactivated herpes virus involved? Can J Neurol Sci. 1982;9:303–6.
Harris SA, Harris EA. Molecular mechanisms for herpes simplex virus type 1 pathogenesis in Alzheimer’s disease. Front Aging Neurosci. 2018;10:48.
Mancuso R, Sicurella M, Agostini S, Marconi P, Clerici M. Herpes simplex virus type 1 and Alzheimer’s disease: link and potential impact on treatment. Expert Rev Anti Infect Ther. 2019;17:715–31.
Jenks JA, Goodwin ML, Permar SR. The roles of host and viral antibody Fc receptors in herpes simplex virus (HSV) and human cytomegalovirus (HCMV) infections and immunity. Front Immunol. 2019;10:2110.
Pincetic A, Bournazos S, Dilillo DJ, Maamary J, Wang TT, Dahan R, Fiebiger BM, Ravetch JV. Type I and type II Fc receptors regulate innate and adaptive immunity. Nat Immunol. 2014;15:707.
Smith KG, Clatworthy MR. FcgammaRIIB in autoimmunity and infection: evolutionary and therapeutic implications. Nat Rev Immunol. 2010;10:328–43.
Kyogoku C, Dijstelbloem HM, Tsuchiya N, Hatta Y, Kato H, Yamaguchi A, Fukazawa T, Jansen MD, Hashimoto H, van de Winkel JG, Kallenberg CG, Tokunaga K. Fcgamma receptor gene polymorphisms in Japanese patients with systemic lupus erythematosus: contribution of FCGR2B to genetic susceptibility. Arthritis Rheum. 2002;46:1242–54.
Siriboonrit U, Tsuchiya N, Sirikong M, Kyogoku C, Bejrachandra S, Suthipinittharm P, Luangtrakool K, Srinak D, Thongpradit R, Fujiwara K, Chandanayingyong D, Tokunaga K. Association of Fcgamma receptor IIb and IIIb polymorphisms with susceptibility to systemic lupus erythematosus in Thais. Tissue Antigens. 2003;61:374–83.
Chu ZT, Tsuchiya N, Kyogoku C, Ohashi J, Qian YP, Xu SB, Mao CZ, Chu JY, Tokunaga K. Association of Fcgamma receptor IIb polymorphism with susceptibility to systemic lupus erythematosus in Chinese: a common susceptibility gene in the Asian populations. Tissue Antigens. 2004;63:21–7.
Willcocks LC, Carr EJ, Niederer HA, Rayner TF, Williams TN, Yang W, Scott JA, Urban BC, Peshu N, Vyse TJ, Lau YL, Lyons PA, Smith KG. A defunctioning polymorphism in FCGR2B is associated with protection against malaria but susceptibility to systemic lupus erythematosus. Proc Natl Acad Sci USA. 2010;107:7881–5.
Johansson PJ, Hallberg T, Oxelius VA, Grubb A, Blomberg J. Human immunoglobulin class and subclass specificity of Fc receptors induced by herpes simplex virus type 1. J Virol. 1984;50:796–804.
Moraru M, Black LE, Muntasell A, Portero F, López-Botet M, Reyburn HT, Pandey JP, Vilches C. NK cell and Ig interplay in defense against herpes simplex virus type 1: epistatic Interaction of CD16A and IgG1 allotypes of variable affinities modulates antibody-dependent cellular cytotoxicity and susceptibility to clinical reactivation. J Immunol. 2015;195:1676–84.
Gwon Y, Kam TI, Kim SH, Song S, Park H, Lim B, Lee H, Lee W, Jo DG, Jung YK. TOM1 regulates neuronal accumulation of Amyloid-β oligomers by FcγRIIb2 variant in Alzheimer’s Disease. J Neurosci. 2018;38:9001–18.
Petersen RC. Mild cognitive impairment as a diagnostic entity. J Intern Med. 2004;256:183–94.
Grundman M, Petersen RC, Ferris SH, Thomas RG, Aisen PS, Bennett DA, Foster NL, Jack CR Jr, Galasko DR, Doody R, Kaye J, Sano M, Mohs R, Gauthier S, Kim HT, Jin S, Schultz AN, Schafer K, Mulnard R, van Dyck CH, Mintzer J, Zamrini EY, Cahn-Weiner D, Thal LJ, Alzheimer’s Disease Cooperative Study. Mild cognitive impairment can be distinguished from Alzheimer disease and normal aging for clinical trials. Arch Neurol. 2004;61:59–66.
Costa AS, Agostini S, Guerini FR, Mancuso R, Zanzottera M, Ripamonti E, Racca V, Nemni R, Clerici M. Modulation of immune responses to herpes simplex virus type 1 by IFNL3 and IRF7 polymorphisms: a study in Alzheimer’s disease. J Alzheimers Dis. 2017;60:1055–63.
Chen JY, Wang CM, Ma CC, Luo SF, Edberg JC, Kimberly RP, Wu J. Association of a transmembrane polymorphism of Fcgamma receptor IIb (FCGR2B) with systemic lupus erythematosus in Taiwanese patients. Arthritis Rheum. 2006;54:3908–17.
Agostini S, Mancuso R, Hernis A, Costa AS, Nemni R, Clerici M. HSV-1-specific IgG subclasses distribution and serum neutralizing activity in Alzheimer’s disease and in Mild Cognitive Impairment. J Alzheimers Dis. 2018;63:131–8.
Faul F, Erdfelder E, Lang AG, Buchner A. G*power 3: 566 A flexible statistical power analysis program for the social, 567 behavioral, and biomedical sciences. Behav Res Methods. 2007;39:175–91.
Mancuso R, Baglio F, Agostini S, Cabinio M, Laganà MM, Hernis A, Margaritella N, Guerini FR, Zanzottera M, Nemni R, Clerici M. Relationship between herpes simplex virus-1-specific antibody titers and cortical brain damage in Alzheimer’s disease and amnestic mild cognitive impairment. Front Aging Neurosci. 2014;6:285.
Amigorena S, Bonnerot C, Choquet D, Fridman WH, Teillaud JL. Fc-Gamma-Rii expression in resting and activated Lymphocytes-B. Eur J Immunol. 1989;19:1379–85.
Brooks DG, Qiu WQ, Luster AD, Ravetch JV. Structure and expression of human IgG FcRII(CD32). Functional heterogeneity is encoded by the alternatively spliced products of multiple genes. J Exp Med. 1989;170:1369–85.
Espéli M, Smith KG, Clatworthy MR. FcγRIIB and autoimmunity. Immunol Rev. 2016;269:194–211.
Daeron M, Malbec O, Latour S, Bonnerot C, Segal DM, Fridman WH. Distinct intracytoplasmic sequences are required for endocytosis and phagocytosis via murine Fc gamma RII in mast cells. Int Immunol. 1993;5:1393–401.
Ravetch JV, Kinet JP. Fc receptors. Annu Rev Immunol. 1991;9:457–92.
Starbeck-Miller GR, Badovinac VP, Barber DL, Harty JT. Cutting edge: expression of FcgammaRIIB tempers memory CD8 T cell function in vivo. J Immunol. 2014;192:35–9.
Wang J, Li Z, Xu L, Yang H, Liu W. Transmembrane domain dependent inhibitory function of FcγRIIB. Protein Cell. 2018;9:1004–12.
Acknowledgements
We would like to thank the patients and their families for their participation in our study as well as the staff of the Rehabilitative Neurology Unit of the IRCCS Santa Maria Nascente, Don C. Gnocchi Foundation. We thank Ronald Kothera and Shufeng Liu for their expert technical assistance.
Funding
This work was supported by Ricerca Corrente 2018 [talian Ministry of Health] and the US National Institutes of Health.
Author information
Authors and Affiliations
Contributions
ASC: Methodology, Investigation, Formal analysis, Data curation, Visualization, Writing—review & editing. SA: Methodology, Investigation, Formal analysis, Data curation, Visualization, Writing—review & editing. FRG: Resources, Investigation. RM Resources, Investigation. MC Data curation, Supervision. JPP: Project administration, Supervision, Conceptualization. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All subjects or their care-givers gave informed and written consent according to a protocol approved by the local ethics committee of the Don Carlo Gnocchi Foundation–ONLUS, Milan, Italy.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Costa, A.S., Agostini, S., Guerini, F.R. et al. Relation between FCGRIIB rs1050501 and HSV-1 specific IgG antibodies in Alzheimer’s disease. J Transl Med 18, 325 (2020). https://doi.org/10.1186/s12967-020-02495-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12967-020-02495-6